Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
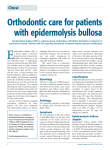
Inherited epidermolysis bullosa
Epidermolysis bullosa
•
•
•
Inherited epidermolysis bullosa (EB) is a group of genetically transmitted skin
disorders characterized by spontaneous blistering or blistering caused by minor
trauma. There are three classic types of inherited EB (simplex, junctional and
dystrophic). They are differentiated by the level of blister cleavage and subdivided
according to the pattern of genetic inheritance, morphology/topography of lesions and
genetic mutation involved. After the Third International Consensus on Diagnosis and
Classification of Inherited EB, there was the addition of a fourth entity to the group of
inherited EB - Kindler syndrome (KS) previously considered a photosensitive
poikiloderma. Currently, over 30 phenotypiccally and genetically distinct nosological
entities have been described illustrates the key molecules involved in the
pathogenesis of EB.
Despite their rarity, inherited EB cause a huge impact on the lives of patients and
their families, due to physical pain, emotional suffering or economic repercussions.
EB is an inherited disease, which means that you have inherited one or two EB
genes. In autosomal dominant EB, only one abnormal gene is needed to express the
disease. This means only one parent needs to carry the EB gene. On the other hand,
autosomal recessive inherited EB requires you to have two EB genes (one from each
parent) to have the disease. If a person has one recessive EB gene paired with a
normal gene they are called a carrier and do not have the disease.
The clinical presentation of inherited EB varies according to the type of disease, and
diagnosis can only be reached by skin biopsy and immunofluorescence or electron
microscopy, the latter being considered the gold standard
Representation of the proteins affected in different types of inherited
epidermolysis bullosa
CLASSIFICATION
I. Epidermolysis bullosa simplex
•
•
•
•
•
Epidermolysis bullosa simplex (EBS) is characterized by a disorder of keratinocytes,
intraepidermal blistering and little systemic involvement. Nail dystrophy, alopecia and mucosal
lesions may occur in more severe forms of the disease. Skin lesions usually disappear without
scarring. Blistering decreases with age. Inheritance is typically autosomal dominant, although rare
cases of autosomal recessive inheritance have been documented.
The intraepidermal cleavage observed in EBS is the result of mutations in the K5 and K14 genes,
which encode the production of keratin and type I and II intermediate filament proteins, expressed
in keratinocytes of the basal layer of the epidermis and epithelial-related complexes.
EBS is subdivided as follows: localized EBS (Weber-Cockaine subtype), generalized EBS
(Köebner subtype), and EBS herpetiformis (Dowling-Meara subtype). The milder forms of EBS
present with blisters that are usually caused by an identifiable traumatic event. The WeberCockaine subtype (EBS-WC) is characterized by mild to severe blistering and palmoplantar
topography, and patients may concomitantly show hyperhidrosis. In its severe forms, hands, feet
and limbs are also commonly involved, although in these cases blisters generally develop soon
after birth. Palmoplantar hyperkeratosis and erosions occur mainly in the Köebner subtype. In the
Dowling-Meara subtype (EBS-DM) there is involvement of the oral mucosa and formation of
herpetiform blisters.
Variable blistering, followed by muscular dystrophy in adulthood, can be seen in EBS with
muscular dystrophy, a defect in the expression of plectin. Late myopathy is due to the fact that
there is plectin in the composition of the cytoskeleton of skeletal muscles. The severity of skin
lesions does not necessarily correlate with the degree of muscular dystrophy. Some patients may
also present dental abnormalities.
As its name suggests, EBS with pyloric atresia presents with pyloric atresia at birth and, usually,
blistering is widespread. In most patients, even with correction of pyloric atresia, prognosis is
unfavorable, given the extent of systemic involvement. Although the disease is described as
precociously fatal, some individuals with milder symptoms can survive during childhoo
Epidermolysis bullosa simplex
Dowling-Meara Epidermolysis Bullosa Simplex
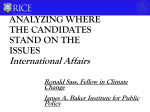
Schematic of desmosomes. Components in red characters are target proteins
of suprabasal EBS
Schematic of the skin basement membrane zone. Components in red
characters are target proteins of basal EBS.
Epidermolysis bullosa simplex
• Mutations in genes encoding keratinocyte components involved in
the organization of the cytoskeleton or cell-cell junctions are
responsible for EBS. EBS can be subclassified into basal and
suprabasal according to the level of skin split .
• Basal EBS is caused by defects in skin basement membrane (BMZ)
proteins. diagrams the skin BMZ. Among the BMZ components,
keratin 5/14 and plectin are the main targets in EBS . A few EBS
cases have been reported to have mutations in ITGB4 and COL17,
which encode β4 integrin and type XVII collagen, respectively .
Recently, BPAG1-e was added to the list of basal EBS target
proteins .
• In contrast, suprabasal EBS is associated with abnormalities in
desmosomal proteins . So far, plakophilin-1, plakoglobin and
desmoplakin are known to be the target proteins of suprabasal EBS
Epidermolysis bullosa simplex
•
•
•
•
•
Target proteins in basal EBS
3.1. KERATIN 5/14
Keratin is one of the most abundant components of the epithelial cytoskeleton . Typically, type I and type II
keratins form heteropolymers that function in cells . Keratin 5 (K5) and keratin 14 (K14) are specifically expressed
in epidermal basal cells . In the 1980’s, disorganization of those keratins was recognized in the basal keratinocytes
of EBS patients . From those findings, it had been hypothesized that EBS patients have mutations
in KRT5 or KRT14, which encodes K5 or K14, respectively. In the early 1990’s, transgenic mice overexpressing
mutated K14 were reported to have severe skin fragility . Soon after this discovery, two groups of researchers
identified EBS cases with heterozygosity for KRT14 misense mutations , which were followed by the identification
of the first EBS family with a heterozygous KRT5 mutation . Since then, several hundreds of EBS patients have
been described as having KRT5 or KRT14 mutations
There are several subtypes of keratin-associated EBS,]. Classical and common EBS subtypes, in which traits are
autosomal-dominantly inherited, are Dowling-Meara type EBS (EBS-DM), non Dowling-Meara type (EBS-gen-nonDM) and localized type (EBS-loc), from the severest to the mildest. Ultrastructurally, basal keratinocytes of EBSDM are characterized by keratin aggregates . Hot spots of the mutations in KRT5 or KRT14 are located within the
helix-boundary motifs of each keratin . A misense mutation in one allele of those regions (which leads to an amino
acid alteration) typically exerts a dominant-negative effect on keratin organization. The severity of the clinical
manifestations among EBS-DM, EBS-gen-non-DM and EBS-loc is generally determined by the site of the
mutations and the difference between the original and the mutated amino acids . However, it is not always easy to
predict the phenotype from the underlying mutations and, in some cases, two different amino acid substitutions at
the same codon result in different clinical manifestations . As a single amino-acid alteration does not necessarily
cause a pathological change, in vitro and in silico systems to validate mutational effects have been proposed
where keratin organization is visualized in cells transfected with mutated or wild-type keratins ..
Therapeutic interventions for EBS have been confined to palliative modalities. However, recent innovations in RNA
interference have led to therapeutic strategies for dominant-negative disorders including keratin-associated EBS,
where aberrant mutated keratin is knocked down while normal keratin synthesis on another allele is left intact [46].
This RNAi strategy is promising and will be further validated in clinical trials.
Epidermolysis bullosa simplex
•
•
•
•
•
•
3.2. PLECTIN
Plectin is a cross-linking protein between the cytoskeleton and membranous proteins including hemidesmosomal
components . Plectin has been known to have many transcript isoforms that differ from each other in N-terminal
sequences at the protein level . Among the many transcript isoforms, plectin 1a is the one that is mainly expressed
in epidermal keratinocytes . In addition to 5’ transcript complexity, plectin has a rodless splicing variant. There are
several EBS subtypes that are caused by plectin deficiencies .
In the mid-1990’s, mutations in the gene encoding plectin (PLEC) were discovered in patients with EBS with
muscular dystrophy (EBS-MD) . Since then, many PLEC mutations, mostly located in the region encoding the rod
domain of plectin, have been reported in EBS-MD patientsIn 2005, two groups independently reported a new EBS
subtype with PLEC mutations: EBS with pyloric atresia (EBS-PA) . EB with pyloric atresia (PA) had been known in
patients withITGA6 or ITGB4 mutations . However, skin specimens from those patients with integrin mutations
show skin-split at the level of the lamina lucida, leading to the diagnosis of junctional EB (JEB). In contrast, EBSPA cases with PLEC mutations were characterized by skin-split within epidermal basal cells .
The reason PLEC mutations lead to two distinct subtypes of EBS was clarified only recently. The development of
monoclonal antibodies against several portions of plectin allowed us to understand the plectin expression patterns
that distinguish between EBS-MD and EBS-PA . EBS-MD skin typically shows the expression of rodless plectin
without that of full-length plectin, whereas neither rodless nor full-length plectin is present in EBS-PA skin .
The next big question was whether EBS-MD and EBS-PA can occur simultaneously in a single patient or those
two distinct EBS subtypes are mutually exclusive. Recently, one case was reported to have the phenotype of both
EBS-MD and EBS-PA (EBS-MD-PA) . The patient had truncation mutations at the last exon of PLEC, which
resulted in the expression of diminished and shortened full-length and rodless plectin without the intermediate
filament binding domain .
Apart from autosomal recessive EBS subtypes associated with PLEC mutations (EBS-MD, EBS-MD and EBSMD-PA), there is one distinct autosomal dominant EBS with a PLEC mutation: EBS, Ogna (EBS-Og). EBS-Og is
caused by a heterogeneous mutation of p. Arg2000Trp and is characterized by mild blister formation without MD or
PA phenotype . To date, 5 unrelated families of EBS-Og have been reported to have the same mutation .
Epidermolysis bullosa simplex
• . BPAG1-E
• Dystonin, encoded by DST, has various isoforms in neural, muscle
and epithelial tissue. BPAG1-e, also called BP230, is a major skin
isoform of dystonin and a component of hemidesmosomes . BPAG1e is known to be an autoantigen in bullous pemphigoid as well as
type XVII collagen (C17) . Since COL17, which encodes C17, was
identified as a causative gene for non-Herlitz JEB , DST, which
encodes BPAG1-e, had also been hypothesized for decades to be a
target gene in other EB subtypes. However, it was only recently that
mutations in DST were identified in autosomal recessive EBS
patients . Those two patients typically had a mild acral blistering
phenotype and had truncation mutations in the coiled-coil rod
domain of BPAG1-e. Electron microscopy observation revealed loss
of the inner plaque of hemidesmosomes in both cases . Dst-null
mice show neural degeneration and mild skin fragility upon
mechanical stress
Epidermolysis bullosa simplex
•
•
•
•
•
•
•
•
. Target
proteins in suprabasal EBS
4.1. DESMOPLAKIN
Desmoplakin is a plakin family protein located in desmosome . Two isoforms (desmoplakins I and II) are generated
through alternative splicing [65]. Desmoplakin I is mainly expressed in the heart, whereas desmoplakin II is
abundant in the skin . In the early 1990’s, desmoplakin was determined as a major autoantigen in paraneoplastic
pemphigus . Mutations in the gene encoding desmoplakin, DSP, have been reported in several genodermatoses,
mostly with cardiac manifestations In 2005, a very severe EB case, referred to as lethal acantholytic
epidermolysis bullosa (LAEB), was reported to have a homozygous deletion mutation in DSP . The patient showed
severe skin blistering and early demise. There have been only three reports on LAEB with DSP mutations . Skin
specimens in all the cases revealed acantholytic features in histopathology. From the correlation of clinical
manifestations and mutational sites, it seems that complete or almost complete loss of desmoplakin might lead to
LAEB . However, at least one full-length desmoplakin (either isoform I or II) may be enough to prevent the
development of LAEB .
4.2. PLAKOPHILIN-1
Plakophilin-deficient EBS is listed in the newest classification of EB . This entity has also been called ectodermal
dysplasia-skin fragility syndrome (ED-SF). An excellent review on this EBS subtype was published recently . The
first case of ED-SF and the mutations in the gene encoding plakophilin-1, PKP1, were reported in 1997 . Since
then, many cases of ED-SF with PKP1mutations have been published. The clinical manifestations of ED-SF
include skin fragility, perioral cracking, alopecia and palmoplantar keratoderma .
The desmosomal expression of plakophilin-1 accounts for skin fragility and histological features of skin specimens
characterized by widening of spaces between keratinocytes. However, the phenotype of ectodermal dysplasia may
not be explained solely by desmosomal proteins. Recently, plakophilin-1 has been identified as a regulator of
protein synthesis and proliferation through a pathway associated with eIF4A1 . It is speculated that the role of
plakophilin-1 in translation and proliferation is involved in abnormalities in skin appendages of ED-SF patients .
4.3. PLAKOGLOBIN
JUP, which encodes plakoglobin, was not listed as a causative gene of EB in the report of the Third International
Consensus Meeting on Diagnosis and Classification of EB . It was only recently that a homozygous nonsense
mutation of this gene, leading to complete loss of plakoglobin, was revealed to be responsible for one subtype of
suprabasal EBS . Lethal congenital EB (LCEB), named by the authors, has manifestations similar to those of
LAEB, which is caused by DSP mutations . This similarity is accounted for by the expression pattern of plakoglobin
and desmoplakin in desmosomes .
Epidermolysis bullosa simplex
Epidermolysis bullosa simplex
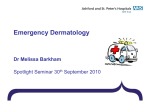
Circinate grouping of blisters arising on the skin of a patient with
the Dowling-Meara variant of generalized EBS
Epidermolysis bullosa simplex
II. Junctional epidermolysis bullosa
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Junctional epidermolysis bullosa (JEB) is an autosomal recessive disorder characterized by separation of the
lamina lucida in the dermo-epidermal junction. A mutation in the LAMB3 gene, which encodes laminin-5, occurs in
more than half of patients with JEB. Mutations in the genes encoding collagen XVII and integrin α6β4 are also
seen.
Classification
Junctional epidermolysis bullosa with pyloric atresia
Junctional epidermolysis bullosa with pyloric atresia is a rare autosomal recessive form of junctional epidermolysis
bullosa that presents at birth with severe mucocutaneous fragility and gastric outlet obstruction. It can be
associated with ITGB4 or ITGA6.
Herlitz type
Junctional epidermolysis bullosa gravis (also known as "Herlitz disease," "Herlitz syndrome," and "Lethal junctional
epidermolysis bullosa") is the most lethal type of epidermolysis bullosa, a skin condition in which most patients do
not survive infancy, characterized by blistering at birth with severe and clinically distinctive perorificial granulation
tissue.
JEB-H is generally caused by mutations in one of the three laminin-332 coding genes: LAMA3 (18q11.2), LAMB3
(1q32) and LAMC2 (1q25-q31).
Non-Herlitz type
These include:
@ Generalized atrophic benign epidermolysis bullosa is a skin condition that is characterized by onset at birth,
generalized blisters and atrophy, mucosal involvement, and thickened, dystrophic, or absent nails.
@ Mitis junctional epidermolysis bullosa (also known as "Nonlethal junctional epidermolysis bullosa") is a skin
condition characterized by scalp and nail lesions, also associated with periorificial nonhealing erosions. Mitis
junctional epidermolysis bullosa is most commonly seen in children between the ages of 4 and 10 years old.
@ Cicatricial junctional epidermolysis bullosa is a skin condition characterized by blisters that heal with scarring
Pathophysiology
α6β4 integrin is a transmembrane protein found in hemidesmosomes. As a heterodimer molecule containing two
polypeptide chains its extracellular domain enters the basal lamina and interacts with type IV collagen
suprastructure containing laminins (laminin-5), entactin/nidongen or the perlecan. on the extracellular surface of
the hemidesmosome, laminin-5 molecules form threadlike anchoring filaments that extend from the integrin
molecules to the structure of the basement membrane of epithelial adhesion. Mutation of the genes encoding
laminin-5 chains results in junctional epidermolysis bullosa.
Appearance of lesions in patients with junctional epidermolysis bullosa
Herlitz type of junctional EB
•
H&E
PAS stain
In the patient's case, the clinical
presentation was suggestive of the
Herlitz type of junctional EB — the most
severe of all types and with poor
prognosis. The differential diagnoses
included dystrophic recessive type. The
demonstration of the lamina densa in the
floor of the blister by means of
immunoperoxidase staining with
antibody to collagen type IV clearly
identifies this lesion as one of the
junctional types of EB. Clinical features
make it most likely Herlitz type. This
child has been found to have related
abnormalities, including pyloric atresia,
and areas of aplasia cutis congenita
features occasionally seen in this
subtype . Most patients in this group will
have involvement of skin and multiple
mucous membranes, most prominently
in the upper respiratory and
gastrointestinal tracts. Epithelial erosions
are followed by formation of large
masses of granulation tissue, which can
cause airway obstruction and GI
obstruction, among other things. These
unfortunate patients rarely survive more
than one year.
Herlitz type of junctional EB (continue)
•
Collagen IV immunoperoxidase
Herlitz JEB (laminin 5, AR). "EB lethalis"
Junctional epidermolysis bullosa
Junctional epidermolysis
bullosa
Junctional epidermolysis bullosa
EB - enamel pitting
Rather profound enamel
pitting in a patient with JEB
Exuberant granulation tissue arising on the nape of the neck of a
child with Herlitz JEB.
Non-Herlitz JEB
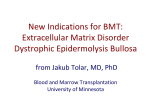
39 year old patient with (a) enamel hypoplasia and severe caries; (b) chronic erosions
and atrophic scarring on the lower legs; (c) periodically recurring erosions and blistering
on the back of the patient; (d) complete toe nail dystrophy
PYLORIC ATRESIA in JEB
•
•
•
•
•
•
•
ULTRASOUND
Dilated esophagus.
Dilated stomach (± a thick
wall) (3).
Marked gastric peristalsis
(due to impairment of
gastric filling and
emptying).
Polyhydramnios.
Color Doppler has been
used to detect biphasic
flow during breathing
movement
suggesting gastroesophag
eal reflux (2).
The lower intestines in
pyloric atresia appear
normal because of the
passage of bile
PYLORIC ATRESIA in JEB
Epidermolysis Bullosa with Congenital Pyloric Atresia Pediatric
Research (2001) 49, 618
Junctional epidermolysis
bullosa
III. Dystrophic epidermolysis bullosa
•
•
•
Dystrophic epidermolysis bullosa (DEB) is due to mutations in the gene encoding type VII
collagen, resulting in defective anchoring fibrils and consequent separation of the sub-basal
lamina. When healed, blisters give way to dystrophic lesions . Millium formation occurs due to
damage in the hair follicles.
DEB may be associated with autosomal recessive or dominant inheritance. In the dominant
subtype (DDEB) clinical manifestations usually occur at birth or during childhood, with generalized
blistering. With increasing age, blisters tend to be more localized. A common variable described
as Cockayne-Touraine has acral distribution and minimal oral/dental involvement. In another
variant, described by Pasini, there is also involvement of the oral mucosa and teeth, but blistering
is more extensive and similar to papules on the trunk (albopapuloid lesions). Dystrophy or
anonychia are common to both forms of DDEB.
The recessive subtype (RDEB) may have a mild to severe clinical presentation. The mild/localized
form is called RDEB mitis, usually with acral and nail involvement, but little involvement of the
mucous membranes. It usually shows clinical manifestations similar to those of other inherited
forms of dystrophic EB. The severe form, described by Hallopeau and Siemens (RDEB-HS)
usually shows generalized blistering, predominantly in acral surface, which can lead to
pseudosyndactyly of the hands ("boxing glove hands") and feet. Flexural contractures of the
extremities are common and intensify with age. Nails and teeth are usually affected, and inner
mucosal involvement can lead to esophageal obstruction, urethral and anal stenosis, phimosis,
and corneal lesions. Malabsorption often leads to iron-deficiency anemia, and protein-calorie
malnutrition causes deficit in global development. Patients with severe RDEB who survive
Appearance of lesions in patients with dystrophic epidermolysis bullosa
Dystrophic epidermolysis bullosa
•
•
EB - atrophic scarring
In a patient with dominant DEB
Dystrophic epidermolysis bullosa
Atrophic scarring and postinflammatory hypopigmentation on the
extremity of a patient with DDEB.
•
Hypertrophic scarring
in a patient with
generalized DDEB.
• Clinical features
of dystrophic
epidermolysis
bullosa. Notes:
(A) Nail
dystrophy of the
toenails in
dominant
dystrophic
epidermolysis
bullosa. (B)
Mitten deformity
of the right hand
of a patient with
recessiv
Dystrophy of all twenty nails in a patient with DDEB.
Partial mitten deformity of the hand of a child with severe
generalized RDEB.
Complete mutilating deformities of the hands of a young adult
with severe generalized RDEB.
Dystrophic epidermolysis bullosa
IV. KINDLER SYNDROME
• Kindler syndrome (KS) is an autosomal recessive genodermatosis
that can clinically simulate all three classic types of inherited EB. It is
a rare dermatosis characterized by acral blistering, fusion of
fingers/toes, and generalized progressive poikiloderma. Other
clinical findings include trauma-induced blistering (common to all
inherited EB), dry and atrophic skin, lichenification and
photosensitivity of proximal surfaces. Generally, KS is associated
with disruption of the basement membrane and abnormal deposition
of type VII collagen both in regions with active lesions and in lesionfree areas. Immunohistochemical examination shows that blistering
occurs in the lamina lucida. Recently, it was shown that this entity
results from mutation in the gene encoding Kindlin-1, a focal
component of contact between basal keratinocytes. As opposed to
other mechano-bullous diseases, there are multiple cleavage planes
(intradermal, junctional or sub-lamina densa) and other
dermatological findings such as poikiloderma and photosensitivity
also differentiate KS from all other forms of inherited EB.
Scanning electron microscopy of a blister roof in dystrophic
epidermolysis bullosa An. Bras. Dermatol. 88 no.6 Rio de Janeiro , 2013
Scanning electron microscopy – A. lower magnification
with identification of the stratum corneum (x 300); B.
Detail of a net attached to the blister roof
The basement membrane is an important structure
involved in dermal-epidermal adherence. In
Dystrophic Epidermolysis Bullosa (DEB), a
welldefined subset of EB, the epidermal loss
includes the basement membrane, which
remains attached to the blister roof. This
level of cleavage can be easily demonstrated
with monoclonal antibodies against collagen
IV (the basement membrane), in so-called
immunomapping. DBE is secondary to
inherited dysfunction of collagen VII, the
protein that forms the anchoring fibrils, which
adhere the basement membrane to the
dermal collagen
Scanning electron microscopy (SEM) of an
inverted blister from a case of DBE in order
to examine the basement membrane, which
is normally found in the blister roof. The
diagnosis was confirmed with
immunomapping and DNA sequencing. The
first showed collagen IV in the roof of the
blister. It was also positive for collagen VII,
ruling out recessive DEB. DNA sequencing
identified in exon 75 of COL7A1 gene a
pathologic mutation: c.6235G>A
(p.Gly2079Arg), establishing the diagnosis of
dominant DEB,
Scanning electron microscopy of a blister roof in dystrophic
epidermolysis bullosa An. Bras. Dermatol. 88 no.6 Rio de Janeiro , 2013
•
Scanning electron
microscopy – A.
Projections from the
cell membrane
(asterisks), (x
2.000). B. Adherence
of the net to the cell
membrane,
IV. Kindler syndrome
• Kindler syndrome is inherited as an autosomal recessive disorder.
This means that an abnormal gene must be inherited from each
parent. On average, one-in-four children in a family are affected, and
the familial nature of the disorder may be unnoticed.
• clinical features of Kindler syndrome
• Blistering and photosensitivity beginning in infancy or early
childhood
• Gradual poikiloderma (altered pigmentation) and cutaneous atrophy
(wasting)
• Trauma related blistering on hands and feet
• Can also develop mucosal involvement, ophthalmic and dental
abnormalities
• Early development of actinic keratoses
KINDLER SYNDROME
•
Clinical features of Kindler syndrome. a, b Poikiloderma with hyperpigmentation and
hypopigmentation on the face, neck, trunk, and extremities. c Large, irregular,
ulcerated tumor present on the patient's left knee. d Ectropion and dental loss (e)
Kindler syndrome
•
•
Kindler syndrome was first described in 1954
by Theresa Kindler. Kindler syndrome is a
rare autosomal recessive genodermatosis
characterized by congenital acral skin
blistering, photosensitivity, progressive
poikiloderma, and diffuse cutaneous atrophy.
The syndrome is a combination of features of
inherited blistering skin disorders (eg,
dystrophic epidermolysis bullosa) and
congenital poikilodermas (eg, RothmundThompson syndrome).
Images show the progression of lesions. A
and B: At birth, acral blisters and erosions are
present. C and D: At age 5 years, atrophy
and reticulated erythema with dyschromic
patches are noted. E and F: At age 7 years,
progressive poikilodermatous changes with
reticulated erythema and telangiectasia
occur. G and H: At age 10 and 15 years,
poikiloderma with telangiectasia and
depigmentation are observed. Excoriations
are due to pruritus. J Am Acad Dermatol 2002
; 46(3): 447.
Kindler syndrome
KINDLER SYNDROME
clinical features of epidermolysis bullosa
Epidermolysis bullosa simplex (EBS)
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Epidermolysis bullosa simplex (EBS)
EBS SubtypesFeatures
Localised EBS
Previously known as Weber-Cockayne
Most common and localised form of EBS
Blisters develop on hands and feet in response to friction
Usually presents in infancy as child is starting to crawl and walk
Wounds heal without scarring but there may be thickening of the skin on soles and palms
Generalised EBS
Previously known as Koebner
Generalised EBS where blisters develop all over the body but commonly on hands, feet and extremities
Presents at birth or early in infancy
May be mild involvement of mucous membranes and nails
Thickening of skin and plaques develop on palms and soles
Generalised severe EBS
Previously known as Dowling Meara
Generalised and severe form of EBS
Present at birth with blistering on the face, trunk and limbs
Thickened skin may cause calluses that limit or interfere with joint movement
Nails often affected
May involve other organs including inside the mouth, gastrointestinal and respiratory tract
Widespread involvement may cause death in infancy but usually there is significant improvement with age
Junctional epidermolysis bullosa (JEB)
•
Junctional epidermolysis bullosa (JEB)
•
•
JEB SubtypesFeatures
Generalised severe JEB
Previously known as Herlitz
Generalised and most severe form of JEB where blisters appear all over the body
and often involve mucous membranes and internal organs
May only present at birth with small single blister but becoming more widespread
soon after
Hoarse cry or cough is indicative of internal organ involvement
Complications such as infection, malnutrition and dehydration usually lead to early
death in infancy
Most cases are lethal within the first 12–24 months of life
Generalised intermediate JEB
Previously known as Non-Herlitz
Generalised blistering and mucosal involvement present at birth or soon after
Scalp, nails and teeth more involved
Complications such as infection, malnutrition and dehydration may cause death in
infancy but those who survive clinically improve with increasing age
•
•
•
•
•
•
•
•
•
Dystrophic epidermolysis bullosa (DEB)
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Dystrophic epidermolysis bullosa (DEB)
DEB SubtypesFeatures
Dominant generalised DEB
Generalised blistering present at birth
Blistering becomes localised to hands, feet, elbow or knees as child grows older and in response
to friction
Small white spots called milia are often present at healed but scarred sites
Bart syndrome: aplasia cutis, lesions in the mouth, and abnormal nails due to abnormal type 7
collagen in anchoring fibrils
May also get blistering of the oesophagus
Generalised severe recessive (R) DEB
Previously known as Hallopeau-Siemens; and;
Generalised intermediate RDEB (previously Non-Hallopeau-Siemens)
May present with severe blistering (generalised severe RDEB) or mild disease (generalised
intermediate RDEB)
Generalised severe blistering is more common and involves large areas of skin and mucous
membranes
Blisters heal but with scarring and deformity causing limited movement as fingers and toes may
be fused together (mitten hands)
Complications such as infection, malnutrition and dehydration may cause death in infancy
Those that survive are at great risk of developing squamous cell carcinoma (SCC) within chronic
EB wounds. SCC look and behave differently in EB than in unaffected individuals, thus a low
threshold for review by a specialist dermatologist should be considered.
Kindler syndrome
•
•
•
•
•
•
•
•
•
Kindler syndrome
Kindler syndrome Features
Kindler syndrome
Blistering and photosensitivity beginning in infancy or early
childhood
Gradual poikiloderma (altered pigmentation) and cutaneous atrophy
(wasting)
Trauma related blistering on hands and feet
Can also develop mucosal involvement, ophthalmic and dental
abnormalities
Early development of actinic keratoses
There are many other subtypes of EB. The presentation and severity
of EB is affected by the specific genetic changes and can at times
be difficult to classify.
CLINICAL MANIFESTATIONS
•
•
•
•
•
Besides the typical blistering and erosions secondary to the mechanical fragility of the skin,
inherited EB may lead to the formation of millium, nail dystrophy or anonychia. Exuberant
granulation tissue (periorificial, in the axillary, occipital, lumbosacral, and periungual regions or at
fingertips) and palmoplantar keratoderma (localized or confluent) may be present. Other less
common and nonspecific findings include reduced or absent hair, recurrent albopapuloid lesions
on the lower trunk, hypo-or hyperhidrosis.
Alopecia. Even in the recessive form of DEB, patients show no specific alopecia. In the presence
of anemia, reversible telogen effluvium may occur. Complete absence of hair, eyelashes and
eyebrows is a distinct finding that occurs in lethal acantholytic EB. Localized or diffuse alopecia
can be observed in Herlitz JEB. In some patients, alopecia presents a typical androgenetic
pattern. The degree of capillary involvement varies considerably between individuals with deficient
type XVII collagen. There is gradual alopecia in areas of frictional trauma and blistering in patients
with DEB. Kindler syndrome is not associated with alopecia.
Gastrointestinal Tract. In theory, any portion of the gastrointestinal tract, except the gallbladder,
pancreas and liver, may be affected in patients with Herlitz JEB, occurring more intensely in
RDEB. The most severe complication is stenosis of the esophagus because it compromises
swallowing. Malabsorptive syndrome may be secondary to denudation of the small bowel mucosa.
As previously mentioned, patients with EBS and JEB may have pyloric atresia at birth.
Anemia. Herlitz JEB patients may present with severe anemia caused by multiple factors,
especially those with JEB and generalized RDEB. Anemia can be partially improved with iron
supplementation and blood transfusions.
Wound healing. This process is compromised by multiple factors including foreign bodies,
bacteria, deficiency of nutritional factors and tissue hypoxia. Exogenous agents such as
glucocorticoids and penicillamine contribute to impaired wound healing. Optimization of healing
occurs with control of these factors. Patents with Herlitz JEB heal slowly, probably due to
deficiency of laminin-5.
CLINICAL MANIFESTATIONS
•
•
•
•
•
•
•
Infections. Extensive areas of bare skin show loss of stratum corneum barrier and allow microbial penetration.
The accumulation of lymph and moisture in the surface increases bacterial growth. Severe subtypes of Herlitz JEB
correlate with immunological abnormalities, including reduced production of lymphocytes. Along with poor
nutritional status, there is decreased resistance to infections. Staphylococcus aureus and Streptococcus
pyogenes are often the etiological agents, although infections with gram-negative bacteria may also occur.
Patients usually show greater susceptibility to develop sepsis, with a high risk of death in early
childhood.Prevention of infection is the preferred strategy. With extensive bare areas or areas of crusting, strict
care must be taken. This regimen includes the use of topical antibiotics. Self-adhesive dressing is a good choice to
keep the areas covered.
Genitourinary Tract. The formation of recurring vesicles along the urethra, in the ureterovesical junction and
ureters can generate obstructive processes culminating with hydronephrosis. There may be chronic renal failure
secondary to hydronephrosis, streptococcal glomerulonephritis, mesangial IgA disease and amyloidosis. They are
the most common complications in RDEB, causing the death of around 12% of these patients.
Eyes. They may be affected by recurring erosions or blisters, with greater frequency in JEB and RDEB. Both can
occur in childhood, causing scarring and progressive visual impairment, if not treated.
Ears, nose and throat. The most significant complication is partial or complete occlusion of the airways, usually
resulting from stenosis of the vocal cords, which can quickly lead to death. It is seen almost exclusively in some
subtypes of JEB and can occur in the first year of life.
Dental manifestations. Tissues of the oral mucosa may be affected in RDEB and JEB. Enamel hypoplasia, which
facilitates the formation of cavities and tooth loss, is a pathognomonic characteristic of all types of JEB, while
microstomia and ankyloglossia are typical of RDEB. Aggressive dental intervention can increase functionality and
contribute to increased nutrient uptake.27
Musculoskeletal system. Progressive contracture of the hands and feet (mitten deformities) may develop in the
first year of life and is seen primarily in the Hallopeau-Siemenes subtype of RDEB. Surgical intervention may
improve hand functionality, although repeated procedures are necessary to maintain this functionality. Osteopenia
and osteoporosis are common in RDEB. Muscular dystrophy beginning in adulthood is typical of EBS with
muscular dystrophy.
Cardiomyopathies. Although uncommon in patients with RDEB-HS, there may be dilated cardiomyopathy,
possibly fatal, especially when there is associated renal failure. The cause may be multifactorial, including
micronutrient deficiencies (selenium and carnitine), transfusion-related iron loss and viral myocarditis.
CLINICAL MANIFESTATIONS
•
•
•
Skin tumors. Squamous cell carcinoma (SCC) usually occurs in multiple primary
sites of chronic lesions, particularly in patients with DEB, especially in RDEB/RDEBHS. In cases of DEB, there is no predilection for photoexposed areas. The peak of
incidence of SCC increases dramatically in the second and third decades of life.
These lesions may recur frequently even with aggressive surgical excision. Recent
studies on the pathogenesis of SCC in patients with RDEB suggest that cancer
occurs due to decreased expression of type VII collagen in the NC1 domain. Type VII
collagen is required for Ras activation in epidermal tumorigenesis.
About 80-90% of patients with HS-RDEB between 45 and 55 years of age have or
have already had SCC. This high risk shows that early detection and treatment of
SCC has great importance in the management of adults with RDEB, considering the
development of severe and recurrent lesions or chronic skin ulcerations and erosions.
However, the presence of scar tissue in patients with chronic Herlitz JEB cannot
explain this phenomenon alone, because SCC that affect scar tissue are not usually
as aggressive as those involving patients with RDEB, suggesting that other factors
may be involved in its pathogenesis.
EBS-DM patients have a substantial risk of developing basal cell carcinoma (BCC).
Possibly, repeated injury to keratinocytes promotes tumorigenesis. The risk of BCC is
low in other subtypes of EBS. The risk of melanoma and BCC in other subtypes is
comparable to that of the general population.
CLINICAL MANIFESTATIONS
•
•
•
•
•
•
•
•
•
•
Fifty-five percent of patients with Herlitz JEB show significant disease impact on quality of life. There is also a
correlation between the Dermatology Life Quality Index - DLQI -and intensity of the psychological disorders
presented by these patients. Psychiatric symptoms are observed in all types of Herlitz JEB. Family is a major
influence, with love and affection being important to improve the quality of life of Herlitz JEB patients, regardless of
financial status, difficulties, emotional factors or time.
The coexistence of symptoms such as depression, anxiety and behavioral disorders should be taken into
consideration, as they may compromise treatment strategies and worsen symptoms.
DIAGNOSIS
The diagnosis of Herlitz JEB is based on clinical and laboratory findings. As genetic differentiation is not available
in most Brazilian cities, subtypes are usually distinguished by immunological and ultra-structural
analysis. Subclassification is important in determining prognosis (risk of mucosal involvement, development of
malignancies and premature death), as well as in providing subsidies for genetic counseling.
Electron microscopy (EM) is still the gold standard in the diagnosis of Herlitz JEB, even though it has some
limitations. Improper handling or problems in skin tissue sample fixation can result in misdiagnosis. These
limitations can be overcome with the concomitant use of immunofluorescence to map the basement membrane in
frozen tissue sections with a variety of antibodies, including laminin-1 and 5, collagen V, VII and XVII, bullous
pemphigoid antigen, integrin α6β4 and plectin. EM is a relatively expensive method and one that is not yet
routinely performed. Immunohistochemical study uses a limited number of antibodies and can be a useful
alternative
DEB, dystrophic epidermolysis bullosa, EB, epidermolysis bullosa; EBS, epidermolysis bullosa simplex; JEB,
junctional epidermolysis bullosa, JEB-H, Herlitz-type junctional epidermolysis bullosa
In the dominant subtypes of EB, where an informative family tree is known, it is often acceptable for a clinical
diagnosis (based on the presenting signs) to be made by a specialist dermatologist.
Diagnostic tests are also available in some countries and include skin biopsy of a newly induced blister which
undergoes immunofluorescence antigen mapping (IFM) and/or transmission electron microscopy (EM). Mutational
analysis (blood testing of genes), although not currently considered the first-line diagnostic test, is also available in
some countries.
.
.
Epidermolysis bullosa
histology
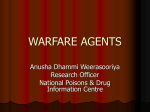
Immunofluorescence antigen mapping for hereditary epidermolysis
bullosa
Photomicrograph showing normal expression of laminin 332 in the control
skin and complete absence of staining in JEB-H (a and b, respectively) and
normal expression of type VII in the control skin and complete absence of staining
in RDEB (c and d, respectively)
THERAPEUTIC MANAGEMENT
•
•
•
•
•
•
•
•
•
•
•
There is no cure for EB. However, significant research, including gene therapy and cell-based
therapy, continue in the aim to improve quality of life.
Most current treatment is symptomatic. The primary aim is to protect the skin and stop blister
formation, promote healing, and prevent complications.
Because EB can affect so many different parts of the body, a team of medical specialists is usually
required for overall care. When necessary, treatment with oral and topical medications may be
prescribed by your doctor to assist healing or prevent complications.
The following are some general measures used in caring for a patient with EB.
@ Avoidance of activities that induce friction on the skin. This includes the handling of infants and
children – alternative handling techniques are easily learnt from a trained health care professional.
@ Maintain a cool environment and avoid overheating
@ Use foam padding or sheepskins to help reduce friction on furniture such as beds, chairs and
infant car seats
@ Choose clothing (including nappies) and footwear that is light, has no irritating seams or detail
eg zips and tight elastic.
@ Pierce, drain and dress blisters to promote healing (this should be done only by people whom
have received training on wound care)
@ Many traditional adhesive tapes and dressings may be unsuitable for people with EB —
especially those with the more severe forms (eg RDEB) — as their removal can cause additional
trauma to the skin. Use of advanced wound care products such as low-adherent silicone tapes
and dressings is recommended. However, resourcefulness by using items readily available, such
as applying additional lubrication (eg Vaseline/paraffin oil) to some traditional wound dressings, is
helpful.
@ When EB affects other parts of the body, various cares and treatments are adopted. For
example, a soft diet when the oesophagus is involved, or using stool softeners for constipation, or
if patient has anal blisters.
Epidermolysis Bullosa – Current Therapies
THERAPEUTIC MANAGEMENT
•
•
•
•
•
•
•
There is no specific therapy for any form of Herlitz JEB. First, an inventory of the affected body
surface area and the type of skin involvement (intact blisters, erosions and chronic lesions) should
be made.
@ Infants require greater care and control of the environment around them to prevent trauma.
This includes gentle manipulation techniques by their caregivers, use of foam to cover bony
prominences and zinc oxide anti-adherent diapers. In older children, the use of special shoes and
foam in the knee to prevent blistering is recommended.
@ With respect to the treatment of lesions, blister puncturing to prevent dissemination and use of
sterile dressings are recommended. The skin should be left in place, functioning as a biological
dressing and preventing bacterial colonization. Firm and easily torn crusts require debridement to
prevent maintenance of the inflammatory process.
The basic principle underlying the care of patients with Herlitz JEB is to prevent blistering with
meticulous skin protection and prevention of infections through wound care. This is done with the
use of non-adhesive synthetic hydrocolloid dressing. Treatment decision should consider the
location of the lesions, need for extra cushioning and protection, use of special dressings and
clothing. Lesions should be cleaned with solutions of low toxicity, such as saline solution and
water.
The antiadherent and absorbent characteristics of dressings were crucial in the choice of
materials, for this is a disease that evolves with bullous lesions, extensive exulcerated wounds,
high chances of infection and scarification. Dressings should also be protective - considering the
development of lesions after minimal trauma - and durable enough for the exchanges to occur
with the minimum possible frequency.
@ Silicone foam is the most complete and effective type of coverage in the healing process,
offering protection, fluid absorption, hydration of the lesions, and antimicrobial properties when
combined with additives such as silver. For drier wounds, foam continues to be the coverage with
the broadest action. Hydrogel dressings, contact layers and biosynthetic cellulose can also be
used. For scarified wounds, hydrogel dressings, biosynthetic cellulose and hydrocolloid are the
best choices, given their debriding action.
.
THERAPEUTIC MANAGEMENT
•
•
•
•
•
@ Nutritional support plays a critical role in the resolution of wounds. Some patients require a
gastrostomy tube for optimal nutritional status. It is also important to monitor and maintain
hemoglobin levels above 8mg/dl. Iron supplementation (oral or intravenous) may be required in
some patients. In symptomatic cases, even blood transfusion may be needed.
@ Topical or systemic antibiotics may be used for short periods following established criteria to
avoid bacterial resistance and sensitization. More than three of the following characteristics
recommend the use of topical antibiotics: wound that does not heal, increased exudate, erythema,
presence of friable tissue, presence of dead tissue and stench. Occurrence of at least three of the
following characteristics indicates the use of systemic antibiotics: increased wound size,
temperature difference greater than 5.4 º C in relation of degradation, erythema or swelling at the
border of the lesion, excessive exudation and stench.
@ Avoiding trauma is essential to manage pain. Analgesic drugs should be prescribed according
to pain severity, with the use of acetaminophen, NSAIDs, and even morphine in case of severe
pain.
@ Patients with Herlitz JEB subtypes showing a well-known risk of extra-cutaneous complications
require careful monitoring and appropriate intervention (medical, surgical, dental, nutritional and
psychological) before the tissues involved become severely injured. Signs and symptoms
suggestive of early disease activity in the cornea require a quick assessment by an
ophthalmologist to avoid permanent scarring and visual impairment. Patients with esophageal
stenosis must undergo dilation to maintain an adequate intake of nutrients orally. Children unable
to ingest food orally should receive supplementation via gastrostomy.
@ Hand deformities should be prevented with appropriate dressings involving all fingers at night.
The "boxing glove hands" can be temporarily improved with surgical procedures. SCC, which may
develop early in these patients, should be treated by wide surgical excision, and the patient
should be monitored to prevent recurrences.3 Patients with generalized forms of JEB and RDEB
should be monitored for prevention and/or early detection of osteoporosis and osteopenia.
NUTRITIONAL COMPROMISE AND REQUIREMENTS IN EB
An. Bras. Dermatol. 90 no.2 Rio de Janeiro . 2015
• The nutritional impairment in patients with EB is directly related to
the severity of associated problems, i.e., the more severe the EB
type, the more extensive the nutritional impairment. Children and
adolescents with junctional or recessive dystrophic EB, as well as
Dowling-Meara, a subtype of EB simplex, have a significant risk of
nutritional deficits. This is due to numerous complications such as
blisters and oral ulcerations, compromised esophageal mobility,
esophageal stenosis, dysphagia, dental problems, digestive and
absorptive disorders, anal erosions and fissures and rectal
constriction. These events result in chronic constipation, blood and
protein loss through the blisters, hypermetabolism secondary to the
increase in thermogenesis and protein turnover, especially in the
presence of infection. These issues have the greatest significance in
children and adolescents due to their immense nutritional
requirements to achieve proper growth. The interactions between
these and other factors are a challenge to the establishment of the
best conduct and it becomes very difficult to determine which
interventions are priorities
Cause-effect correlation of inadequate nutritional intake in patients with severe
types of EB An. Bras. Dermatol. 90 no.2 Rio de Janeiro . 2015
•
•
Malnutrition in EB patients, being the result
of a combination of decreased food intake
and increased nutrient demand, leads to
failure to thrive , delayed puberty, anemia
and a cascade of clinical and biological
events that, together, culminate with the
interruption or retardation of wound
healing. Nutritional depletion and proteinenergy malnutrition can result in alteration of
immunocompetence, and secondary
bacterial infections have been reported in EB
patients.
The nutritional needs of children and
adolescents with minimal blisters and little or
no gastrointestinal involvement are unlikely
to be higher than those of their healthy peers
with matching age and sex. In severe forms
of EB, however, it is difficult to quantify the
nutritional needs due to a number of factors,
such as: 1- the multisystemic, inflammatory
and infectious nature of the disease; 2variable nutritional requirements reflecting
the age, extent of blisters, presence of
infection, need for catch-up growth, among
others; 3-difficulties associated with desirable
weight gain estimates, since height is also
affected by chronic inflammation, pain,
osteoporosis and articular contractures and
4-difficulty in conducting clinical trials due to
the limited number of patients.
Energy requirement estimate for patients with EB
An. Bras. Dermatol. 90 no.2 Rio de Janeiro . 2015
Epidermolysis Bullosa (EB) — The Worst Disease
You've Never heard of