Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
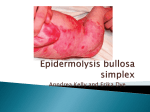
Twelve-month Efficacy and Safety Findings of SD-101 Cream From an Open-label Extension Study on Reducing Body Surface Area Coverage of Lesional Skin in Patients With Epidermolysis Bullosa Amy Paller, John Browning, Rummana Aslam, Susan J. Bayliss, Aida Lugo-Somolinos, Robert Sidbury, Eric Cantor, Christopher Viereck, Allen Reha, Willistine Lenon, Lindsay Reklis, Ronald V. Nardi, Jamie Gault, Jay Barth 1 2 3 4 5 6 7 7 7 8 8 8 8 7 Northwestern University Feinberg Medical School, Chicago, IL, USA; Texas Dermatology and Laser Specialists, San Antonio, TX, USA; Center for Advanced Wound Care, Hackensack University Medical Center, Hackensack, NJ, USA; Dermatology Division, Washington University School of Medicine, St. Louis, MO, USA; 5 6 7 8 Department of Dermatology, University of North Carolina, Chapel Hill, NC, USA; Seattle Children’s Hospital, Seattle, WA, USA; Amicus Therapeutics, Inc., Cranbury, NJ, USA; Scioderm - An Amicus Therapeutics Company, Durham, NC, USA 3 Epidermolysis Bullosa • A rare group of life-threatening genetic disorders that are characterized by mechanical fragility and blistering or erosion of the skin, mucosa, or epithelial lining of other organs, in response to little or no or trauma1 • High risk of infection and electrolyte loss associated with fragile skin and the resultant shearing1 • Usually diagnosed in neonates; occurs in 19 per million live births in the United States2 • Subtypes differ by physical manifestations, genetic makeup, and prognosis (Figure 1 and Table 1)1,3 • Symptoms of epidermolysis bullosa—blistering, scarring, disfiguration, pain—can vary in severity and lead to premature death1,3 Figure 1. Sites of Primary Blister Formation for Major Epidermolysis Bullosa Subtypes4 • In patients with epidermolysis bullosa, quality of life and family burden (as assessed via validated tools such as the Family Strain Questionnaire and General Health Questionnaire-12) have been shown to correlate with disease severity as assessed by the BSAi8,9 • BSAi is weighted as 50% of the total severity score assignment in the Birmingham Epidermolysis Bullosa Severity Score, which was specifically developed to capture the impact of the disease10 Figure 3. Body Subdivision of 4 Regions Assessed in the BSAi Figure 5. Change in BSA Affected by Wounds/Lesions at Each Body Region From Baseline to Month 12 Head and Neck OBJECTIVE Arms Trunk • Evaluate the safety and efficacy of SD-101 6% in patients with epidermolysis bullosa in an ongoing phase 2b 12-month, open-label extension study (SD-004; NCT02090283) ◦◦ Although the open-label extension study will continue for up to 1080 days, only the 12-month results are reported in this analysis Total BSAi 1.0 Junconal Herlitz EB Basement membrane Dermis Anchoring fibrils Dystrophic EB EB=epidermolysis bullosa. Table 1. Epidermolysis Bullosa Types (representing ≈99% of the patient population)1,2,4 Subtypes Junctional Dystrophic Simplex Symptoms • Blistering of skin/mucosa • Severe complications, especially infection • Usually fatal early in life • Skin and mucosal blistering • Narrowing of esophagus • Higher risk of skin cancer • Superficial blistering Frequency Mortality Risk ≈5% SD-003 SD-004 ≈25% ≈70% SD-101 • A topical, proprietary formulation of highly stable, soluble allantoin designed to deliver a high concentration (up to 6%) ◦◦ FDA-designated breakthrough therapy for the daily treatment of wounds caused by all major types of epidermolysis bullosa5 ◦◦ Allantoin appears to have multiple wound-healing effects, including anti-inflammatory and antimicrobial activity and tissue formation and differentiation, specifically in stimulating development of granulations and a tendency towards epithelialization6,7 5 Body Surface Area Index (BSAi) in Epidermolysis Bullosa • The extent of skin lesions can vary markedly in the different epidermolysis bullosa types and subtypes and in relation to age1 • The BSAi is a clinically meaningful endpoint commonly used in epidermolysis bullosa and psoriasis trials as a global measure of disease “spread” with weighting factors (NCT00825565, NCT02670330) Supported by Amicus Therapeutics, Inc. • The efficacy and safety of SD-101 was evaluated in a phase 2b multicenter, randomized, double-blind, placebo-controlled 3-month study investigating the safety and efficacy of SD-101 cream (3% and 6%) applied daily to the entire body for treatment of all major forms of epidermolysis bullosa (SD-003; NCT02014376) (Figure 2) ◦◦ Key inclusion criteria –– Diagnosis of simplex, recessive dystrophic, or junctional non-Herlitz epidermolysis bullosa –– Aged ≥6 months –– Epidermolysis bullosa-related target wound ≥21 days old and between 5 and 50 cm2 in size ◦◦ Key exclusion criteria –– No clinical evidence of local infection in the selected target wound –– Use of any investigational drug ≤30 days before enrollment –– Use of immunotherapy or cytotoxic chemotherapy ≤60 days before enrollment –– Use of systemic or topical steroidal therapy ≤30 days before enrollment (inhaled steroids and ophthalmic drops containing steroids are allowed) –– Use of systemic antibiotics ≤7 days before enrollment –– Arterial or venous disorder resulting in ulcerated lesions • Upon completion of the 3-month study, patients had the option to continue treatment in this long-term (up to 1080 days) open-label extension study, in which all patients would receive SD-101 6% applied once daily to the entire body for the treatment of epidermolysis bullosa (Figure 3) ◦◦ For this analysis, efficacy and safety outcomes were assessed at 14, 90, 180, 270, 360, and 450 ± 7 days from baseline ◦◦ Open-label extension inclusion criteria: informed consent, successful completion of SD-003, and willingness to comply with SD-004 protocol requirements ◦◦ Open-label extension exclusion criteria: female patients who were pregnant or breast feeding, or with childbearing potential who were not practicing abstinence or a medically acceptable method of contraception • Efficacy was assessed using the BSAi (expressed as % of body surface) ◦◦ A physician assessment of the extent of epidermolysis bullosa lesions over the entire body, calculated as a total sum of 4 regions (head/neck, upper limbs, trunk including groin, and lower limbs) with relevant weighting factors specific to age and body region included Figure 2. SD-004 Study Design Patients With EB (N=48) Age: ≥6 months Randomized 1:1:1 • SD-101 6% (n=15) • SD-101 3% (n=16) • Placebo (n=17) Phase 2b, 3-month, placebo-controlled study SD-101 6% Optional SD-004 open-label Baseline extension 14 (N=42) 90 180 −3.0 270 360 Continuing up to day 1080 450 Safety and Efficacy Assessment Visits (Days) 1.0 • Safety and tolerability were evaluated based on tolerability at the application sites, adverse events (AEs), and physical examinations throughout the course of the study ◦◦ AEs may be volunteered spontaneously by the patient and will also be recorded by the physician during study visits ◦◦ AEs will be followed to resolution or until a persistent AE is determined to be stable or clinically insignificant or until information is not obtainable from the patient P=0.0088 Week 2 (n=41) Month 3 (n=37) Visit Month 9 (n=30) SD-101 6% −0.4 −0.6 −0.8 P=0.1643 Week 2 (n=41) Month 3 (n=37) Month 6 (n=33) Visit Month 9 (n=30) Month 12 (n=28) SD-101 6% 0.0 −0.3 −0.6 Baseline (N=42) Trunk Region Upper Limbs 0.3 −0.9 Month 12 (n=28) −0.2 Baseline (N=42) Baseline Characteristics Month 6 (n=33) 0.0 −1.0 RESULTS • • • • Change From Baseline Epidermis −2.0 Limbs 1.0 0.0 −0.2 −0.4 −0.6 −0.8 −1.0 −1.2 −1.4 −1.6 Baseline (N=42) P=0.1662 Week 2 (n=41) Month 3 (n=37) Month 6 (n=33) Visit Month 9 (n=30) Month 12 (n=28) Lower Limbs SD-101 6% P=0.0946 Week 2 (n=41) Month 3 (n=37) Month 6 (n=33) Visit Month 9 (n=30) Month 12 (n=28) Values represent the mean change in BSA affected by wounds/lesions from baseline to each study visit for given body regions for all patients who received at least 1 dose of SD-101 6%. 42 patients (88%) provided informed consent to continue in the SD-004 extension study In study SD-003, patients were treated with placebo, SD-101 3%, or SD-101 6% Dystrophic epidermolysis bullosa was the most common subtype Mean lesional BSAi was 11.3% ± 10.1% CONCLUSIONS BSAi Changes • Total lesional BSAi decreased from baseline to 12 months (P=0.06) (Figure 4) • Mean change from baseline also showed a decrease for all 4 regions measured: head/neck, upper limbs, trunk including groin, and lower limbs (Figure 5) ◦◦ Although all body regions demonstrated a decrease in BSAi affected by wounds/lesions, only the head and neck region showed a significant decrease at month 12 (P=0.0088) Figure 4. Change in Total BSA Affected by Wounds/Lesions From Baseline to Month 12 • Treatment with SD-101 6% cream demonstrated long-term (up to 12-month) improvements in the BSAi, with decreases in percentage of total BSA affected by wounds/lesions as well as decreases for each specific region analyzed, including the head/neck, upper limbs, trunk including groin, and lower limbs • The results of the SD-004 extension study provide further support for the safety of SD-101 6% in patients with epidermolysis bullosa ◦◦ This ongoing study will continue through 1080 days, and future analyses will further determine the long-term efficacy and safety of SD-101 6% • Ongoing phase 3 clinical trials will continue to examine the safety and efficacy of SD-101 6% cream compared with placebo 3 2 Change in Total Lesional BSAi From Baseline (%) EB simplex −1.0 Baseline (N=42) SD-004 Study Design 1 0.0 −4.0 METHODS Head and Neck Region SD-101 6% Change From Baseline INTRODUCTION 4 Change From Baseline 2 Change From Baseline 1 Mean Absolute Change to Month 12 (95% CI): −3.41% (−7.0%, 0.2%) 1 0 P=0.06 −1 −2 −3 −4 Mean ± SEM Mean Relative Change to Month 12 (95% CI): −12.9% (−37.8%, 11.9%) REFERENCES 1. El Hachem M et al. Orphanet J Rare Dis. 2014:9;76. 2. Fine JD. Orphanet J Rare Dis. 2010:5;12. 3. Pagliarello C, Tabolli S. Expert Rev Pharmacoecon Outcomes Res. 2010;10:329-338. 4. DEBRA International website. Epidermolysis bullosa. http://www.debra-international.org/ epidermolysis-bullosa.html. Accessed June 13, 2016. 5. Paller A et al. Presented at: Society for Investigative Dermatology 75th Annual Meeting; May 11-14, 2016; Scottsdale, AZ. 6. Araújo LU et al. Acta Cir Bras. 2010:25;460-466. 7. Özçelik B et al. Pharm Biol. 2011:49;396-402. 8. Tabolli S et al. Acta Derm Venereol. 2010:90;607-611. 9. Tabolli S et al. Br J Dermatol. 2009:161;869-877. 10.Moss C et al. Br J Dermatol. 2009:160;1057-1065. ACKNOWLEDGEMENTS −5 Baseline 3 6 Time, Months 9 12 BL N=42 M3 n=37 M6 n=33 M9 n=30 M12 n=28 Third-party writing assistance was provided by ApotheCom, which was supported by Amicus Therapeutics, Inc. Open-label, long-term, extension study (SD-004, NCT02090283) Primary objective: demonstrate the continued safety of SD-101 6% in patients with EB Secondary objective: continue to assess the change in body surface area of blisters or lesions Note: baseline BSAi for the entire group=11.3%; baseline BSAi for the group at 12 months=10.9%. BL=baseline; CI=confidence interval; M=month; SEM, standard error of mean. http://bit.ly/2958kHL Presented at: 42nd Annual Meeting of The Society for Pediatric Dermatology; July 14-17, 2016; Minneapolis, MN