Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
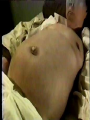
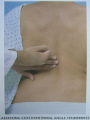
Abdominal Examination Xue Huiping Introduction Question1 : What do you think is the better or more appropriate sequence of abdominal examination compared with that in other areas? And why? Normal sequence: inspection, palpation, percussion, and auscultation Abdominal examination: inspection, auscultation, percussion, and palpation It’s convenient to perform the auscultation of abdomen after the auscultation of the heart. To avoid the negative impacts of a series of palpations on auscultation of bowel sounds due to the alteration of peristalsis. Question 2: Can we say that abdominal examination will be outmoded and superseded because of remarkable advances in supplementary examination methods such as X-ray, ultrasound, endoscopy, isotope, angiography, CT, MRI, etc. ? Definitely Not. Because the abdominal examination is a fundamental method of detecting abnormal signs of abdomen. Palpation is the most difficult step of abdominal examination, requiring more practice. Anatomic Landmarks — xiphoid (ensiform) process(剑状突起) of sternum(胸骨) — costal margin肋弓缘 — umbilicus脐 — anterior superior iliac spine髂前上棘 — inguinal ligament 腹股沟韧带 — superior margin of os pubis耻骨上缘 — anterior midline/midabdominal line前中线/ 腹中线 — lateral border of rectus muscles 腹直肌外缘 — symphysis pubis (耻骨联合) xiphoid process 腹中线 midabdominal line costal margin Lateral border of rectus muscle umbilicus Anterior superior iliac spine 腹股沟韧带 耻骨上缘 superior margin of os pubis inguinal ligament Zones used of abdomen Commonly methods of subdividing 腹 部 the 分abdomen 区 Four quadrants Nine sections right upper quadrant left upper quadrant right lower quadrant left lower quadrant √ The anterior surface of the abdomen is divided into four quadrants by two intersecting lines, one extending vertically from the xiphoid, through the umbilicus, to the symphysis pubis (耻 骨联合)and the other extending horizontally across the abdomen at the level of the umbilicus. √ This divides the abdomen into the RUQ (right upper quadrant), RLQ (right lower quadrant), LUQ (left upper quadrant), and LLQ (left lower quadrant. √ The content of the abdomen underlying each of the four quadrants should be known as follows: Right upper quadrant Liver Gallbladder胆囊 Duodenum十二指肠 Caput pancreas胰头 Right kidney右肾 Hepatic flexure of colon结肠肝曲 Left upper quadrant Stomach Spleen脾 Left kidney左肾 Cauda pancreas胰尾 Splenic flexure of colon结肠睥曲 Right lower quadrant Cecum盲肠 Appendix阑尾 Right ovary and uterine tube右侧卵巢 及输卵管 Right ureter右输尿管 Left lower quadrant Sigmoid colon乙状结肠 Left ovary and uterine tube左 侧卵巢及输卵管 Left ureter左输尿管 right hypochondrial epigastric region right lumber region left hypochondrial left lumber region umbilical region right iliac region hypogastric region left iliac region Two imaginary, parallel, horizontal lines √across the lowest border of the costal margin √across the anterior superior iliac spine Two imaginary, parallel, vertical lines √ across the middle of linking line formed by left anterior superior iliac and midabdominal line √ across the middle of linking line formed by right anterior superior iliac and midabdominal line Left hypochondrial region 左上腹部;左季肋部 Spleen; stomach; splenic flexure of colon; cauda pancreas; left kidney; left adrenal gland(左肾上腺) Left lumber region左侧腹 部;左腰部 Descending colon(降结肠); jejunum(空肠) or ileum(回肠); left kidney Left iliac region左下腹部; 左髂部 Sigmoid colon; female left ovary and uterine tube; male left varicosity(精索) and lymph node Right hypochondrial region右上腹部;右季肋部 Right lobe of liver(肝右叶); gallbladder; hepatic flexure of colon; right kidney; right adrenal gland Right lumber region 右侧腹部;右腰部 Ascending colon; jejunum(空肠); right kidney Right iliac region右下腹 部;右髂部 Cecum(盲肠); appendix; lower part of ileum(回肠); lymph node; female right ovary and uterine tube; male right varicosity Epigastric region上腹部 Stomach; left lobe of liver; duodenum(十二指肠); caput pancreas and body of pancreas; transverse colon; aorta abdominalis(腹主动脉); omentum majus/the greater omentum (大网膜) Umbilical region中腹部; 脐部 Lower part of duodenum; jejunum; ileum; ptosis(下垂) part of the stomach or transverse colon; ureter(输尿管); aorta abdominalis; mesentery(肠系膜) and lymph nodes; omentum majus Hypogastric region下腹部 Ileum; sigmoid colon; ureter; full bladder; pregnant uterus(子宫) Question 3: What are the distinct benefits and disadvantages in Four-quadrant and Ninesection methods? Four-quadrant √ simple, practical, √ rough, imprecise (tenderness of epigastric regin) Nine-section √ elaborates more clearly and more exactly √ inconvenient √ limited scope of left or right hypochondrial region, left or right iliac region Inspection notes position (supine) scope of exposure (adequate, xiphoid process -- symphysis pubis, others covered ) sequence angle (side, tangent) Before any physical examination is carried on, you should do several general preparations as follows: 1. To ask the patient to urinate completely to be sure that the bladder is empty. 2. Patient should be lying on his back with a pillow under his head and his knees bent to relax his abdominal muscles. Be sure the arms are on either side, not behind his head. A little conversation or repeating of the patient’s history might help to relax the patient. 3. To expose abdomen completely from the breasts to pubis. For female patients, breasts should be covered with a sheet. The major contents of inspection abdominal contour respiratory movements abdominal veins gastral or intestinal pattern(胃型或肠型) peristalsis(蠕动波) abdominal rash, hernia(疝), striae(纹), etc. Pay attention to √ whether the abdomen is symmetrical √ whether it is bulged or retracted √ whether it is indicative of ascites or enclosed mass(包块) Normal √abdominal flatness(腹部平坦) √ abdominal fullness(腹部饱满) √ abdominal lowness(腹部低平) Abdominal flatness √the abdomen is at the same level or lower as between costal margin and symphysis pubis. √ If you ask the patient to sit, the lower part of umbilicus can become more or less protruded or bulged. abdominal fullness If he or she is very fat or is a child, the abdomen is a little bit round. The level of the abdomen is higher than that of the surface between costal margin and symphysis pubis. abdominal lowness If a patient is very thin or slender, the level of the abdomen is lower than that of the surface between costal margin and symphysis pubis, as a result of little subcutaneous fat. √Abdominal flatness, abdominal fullness, and abdominal lowness are all normal cases. √ If the abdomen is obviously or extremely protruded or bulged, or it is conspicuously or exceedingly retracted or depressed, that phenomenon is abnormal and usually indicates pathological. some important pathological conditions Abdominal protuberance/bulge 腹部膨隆 I. Overall/generalized abdominal protuberance/bulge全腹膨隆 √Overall abdominal bulge can be caused by several pathological factors besides overly obesity or physiological pregnancy. i. Peritoneal fluid If there is a large amount of free fluid within the abdomen, i, e. ascites, abdominal wall can be lax in supine position, fluid can deposit at both lateral sides, the contour just like a frog belly. √If the patient lies on one side or sits, the lower part of abdominal wall will be bulged, as from the movement of free fluid. √ This is commonly found in ascites complicated by portal hypertension of liver cirrhosis. At that case, esp. in long-standing ascites, the appearance of the umbilicus is protruded or everted. √ In obesity and fat, the umbilicus is usually deeply inverted. Apical belly尖腹 Apical belly is caused by peritonitis or infiltration of cancers, and hence abdominal muscle is tense, usu. with the apical shape. ii. Peritoneal air 腹腔积气 √Peritoneal air is caused by a large amount of air accumulating in the cavity of stomach. √ The general shape of abdomen is globular and two sides of lumber region is not obviously protrudent. √ If you ask the patient to move or change the position, the shape of abdomen remains globular. √ This is commonly found in intestinal obstruction or enteroparalysis(肠麻痹). Pneumoperitoneum气腹 √ Pneumoperitoneum is caused by air accumulating in the abdominal cavity. √ It is commonly found in perforation of gastrointestinal diseases or artificial pneumoperitoneum meant to treat. iii. Huge abdominal enclosed mass 腹内巨大包块 Huge abdominal enclosed mass is usually found in full-term pregnancy, huge ovarian cyst(卵巢囊肿), teratoma, etc. For any generalized abdominal bulge, circumference of abdomen should be measured in centimeters at the level of the umbilicus with a soft tape measure during normal abdominal breathing. II. Local abdominal bulge局部膨隆 Local abdominal bulge is usually caused by enlarged viscera, tumor, inflammatory enclosed mass, gastrointestinal flatulence(肠胃胀气), hernia, etc. Abdominal concavity/ retraction 腹部凹陷 In supine position, if the abdomen is at the level much lower than that between costal margin and symphysis pubis, we call it abdominal concavity/retraction. There are two kinds of retraction, that is, overall abdominal retraction and local abdominal retraction. The former one is of great significance. I. Overall abdominal concavity/retraction 全腹凹陷 Overall abdominal retraction is usually found in patients severely emaciated or seriously dehydrated. Scaphoid abdomen舟状腹 √Scaphoid abdomen is so called because the contour of abdomen is shaped like a boat, with the anterior abdomen almost approximating to spinal column and arch of rib, iliac crest (髂嵴), as well as symphysis pubis all appearing. √ This sign is commonly seen in cachexia(恶病质). II. Local abdominal retraction 局部凹陷 Local abdominal retraction is caused by the contraction of scar after operation and is less common. abdominal contour abdominal protuberance (腹部膨隆) Overall/generalized abdominal protuberance/bulge: ascites, frog belly, apical belly peritoneal air ; pneumoperitoneum abdominal enclosed mass Local: 局部包块:炎性、肿瘤、粘连。 注意包块的部位、外形、移位、搏动。 腹部凹陷 (abdominal concavity) 全腹凹陷:舟状腹(scaphoid abdomen), 见于恶液质、糖尿病、甲亢、 Sheehan病等。 局部凹陷:疤痕收缩。 腹壁情况 Rash皮疹:部位、形态、色彩、时间等。 Pigment色素:Addison’s disease;Cullen sign;GreyTurner sign。 Abdominal striae腹纹:白纹、妊娠纹、紫纹。 Scar 瘢痕:手术史的证实。 Hernia 疝:腹股沟斜、直疝;腹壁疝;脐疝。 Umbilicus 脐部: Body hairs 体毛:男、女性差异。 Groin 腹股沟:包块、结节、疤痕、异常搏动。 Cullen sign ----- A bluish discoloration of the umbilicus occasionally is seen after major intraperitoneal hemorrhage. Grey-Turner sign ----- A similar discoloration of the flanks, in the absence of trauma, occasionally is seen following the extravasation of blood from intra-abdominal organs into extraperitoneal sites, as in hemorrhagic pancreatitis. √ In the normal female the pubic hair is roughly triangular with the base above the symphysis, whereas in the male it is in the shape of a diamond, often with hair continuing to the umbilicus. √ The distribution and quantity of hair may be altered by chronic liver disease and various endocrine abnormalities. 腹壁静脉及其血流方向 上腔静脉阻塞: 向下 下腔静脉阻塞: 向上 门静脉阻塞: 脐为中心,放射状, 水母头(caput medusae)。 abdominal veins Normally, abdominal veins do not appear unless the patient is thinner or is light-complexioned, or abdominal inner pressure is elevated, as from ascites, huge abdominal tumor, pregnancy, etc. √ The presence of distended abdominal veins indicates impairment of circulation caused by portal hypertension or obstruction of superior or inferior vena cava. √ Prominence of these vessels, called abdominal wall varicosis(腹壁静脉曲 张), indicates increased collateral circulation as a result of obstruction in the portal venous system or in the vena cava. √ With obvious portal hypertension, the dilated veins appear to radiate outward from the umbilicus, like the head of medusa(水母), so these distended veins are called caput medusae(海蛇神头). Remember: √ It is known that the normal direction of flow in abdominal vessels is away from the umbilicus, that is, the upper abdominal veins carry blood upward to the superior vena cava and the lower abdominal veins drain downward to the inferior vena cava. √ If a vein is engorged, the direction of flow can be demonstrated by a simple maneuver. maneuver: √ placing the index fingers side by side over the vein, pressing laterally, separating the fingers one by one, and observing the time it takes the veins to refill from each direction; √ The flow of venous blood is in the direction that fills the fastest. Remember Usually the rate of filling is obviously faster in one direction than in the other, indicating the direction of flow in that portion of the collateral venous system. In portal hypertension normal flow direction is maintained. In contrast, obstruction of the vena cava alters the flow direction in these veins. In obstruction of the superior vena cava, the flow direction in the upper abdominal venous collaterals is reversed or downward. In inferior vena cava obstruction the direction is reversed in the lower abdominal veins, and they will drain upward. 呼吸运动 正常表现:男性、小儿:腹式为主。 女性:胸式为主。 病理状态:腹式受限—腹部炎症、包块、 积液、膈肌麻痹。 腹式增强—癔症性呼吸、胸部疾病。 respiratory movements Respiration in a female is mainly costal, and little movement of the abdominal wall occurs; In males and children, the breathing is quiet with the major respiratory movement being abdominal. Restriction of the abdominal phase of respiration, especially in the male patient, may be found in disease and inflammation below the diaphragm (particularly peritonitis). In severe case, as in acute peritonitis from gastrointestinal perforation or phrenoplegia(膈 瘫痪), i.e., diaphragm paralysis, respiration entirely disappears. 胃肠型和蠕动波 gastric or intestinal pattern and peristalsis 正常人:见于经产妇与消瘦腹壁松软者。 幽门梗阻:上腹部逆蠕动。 小肠梗阻:不规则隆起,此起彼伏。 结肠梗阻:全腹膨隆、宽大肠型。 gastral or intestinal pattern(胃型或 肠型) and peristalsis(蠕动波) In lean individuals, even in the absence of disease, motility of the stomach and intestines may be reflected in the abdominal wall. When strong contractions are visible through an abdominal wall of average thickness, the possibility of bowel obstruction should be investigated. Reverse peristalsis indicates pyloric stenosis, duodenal stenosis, or malrotation of the 上腹部搏动 由腹主动脉搏动传导,可见于正常较瘦者。 异常情况:1.腹主动脉瘤和肝血管瘤 2.右心室增大:二尖瓣狭窄 或三尖瓣关闭不全 腹部听诊 肠鸣音(bowel sound,gurgling sound) 正常:4-5次/分 活跃:10次/分 亢进:次数多、调高 减弱:少于1次/分 消失:3-5分 Bowel sounds(borhorygmus) 肠鸣音 Auscultate bowel sounds with diaphragmatic head of stethoscope for at least one minute. If there are no bowel sounds, listen until you hear them or for at least 5 minutes. Normal bowel sounds are a glue-glue, glue-glue-like sound occurring either separately or together, approximately 4-5 times per minute. Pay attention to the frequency, pitch, and intensity. High-pitched (gurgling) sounds with increased frequency are regarded as hyperactivety. Lack of bowel sounds indicate little or no peristalsis. Bowel sounds(borhorygmus) 肠鸣音 The absence of any sound or extremely weak and infrequent sounds heard after several minutes of continuous auscultation ordinarily represent the immobile bowel of peritonitis or paralytic ileus. In contrast, increased sounds with a characteristic loud, rushing, high-pitched tinkling quality often occur in mechanical intestinal obstruction and may be accompanied by waves of pain. The latter findings are caused by distention of the bowel and increased peristaltic activity proximal to the site of the obstruction. 血管杂音(vessel murmurs) 动脉性:中腹部或腹部一侧、动脉瘤或 主动脉狭窄、收缩期杂音。 静脉性:脐周、门脉高压、无收缩期与 舒张期性质。 Murmurs(杂音) or bruits Murmurs from arteries are called bruits and are similar to low-pitched heart murmurs. Murmurs from veins sound like a hum and are more continuous; they are called venous bruits or venous hum . To be of significance a bruit must be heard consistently in the area if the patient is moved into various positions, and it must be heard with extremely light pressure on the diaphragm of the stethoscope or with belltype head of stethoscope: 摩擦音(friction rubs) 脾梗塞、脾周围炎、肝周围炎、或胆囊炎累 及腹膜。 搔刮试验(scratch test) 确定肝脏边缘; 确定腹水。 水坑试验(puddle test) 确定腹水少至120ml 叩 诊 正常腹部叩诊音 鼓音 (tympany)为主; 实音仅见于肝脾(肿大)部位. Percussion General percussion All four quadrants of the abdomen are evaluated by percussion. Light percussion is preferable, since it produces a clearer tone. Tympany(鼓音) is the most common percussion sound in the abdomen due to gas collection. It is appreciated over the stomach, small intestine, and colon. Percussion of the liver Percussion of the upper border of liver(肝 上界) is executed along the right midclavicular line(右锁骨中线), right midaxillary line(右腋中线), and right scapular line(右肩胛线). The level of the shift from resonance downward into dullness is defined as the upper border of liver. At this level, the liver is covered by lung and hence the border is also called the relative dullness border of liver(肝相对浊音界). Percussion of the liver Then percussing downward 1-2 intercostal space, the level of the shift from dullness into flatness(实 音) is identified as the absolute dullness border of liver(肝绝对浊音界), without lung covering, and also called the lower border of lung(肺下界). Normally the the upper border of liver locates at the 5th intercostal space along the right midclavicular line, the 7th intercostal space along the right midaxillary line, and the 10th intercostal space along the right scapular line. Percussion of the liver Percussion of the lower border of liver(肝下界) is executed along the right midclavicular line or anterior midline. The level of the shift from tympany upward into dullness is defined as the lower border of liver. Percussion of liver span (肝上下径) Percussion of liver span should be done with the patient breathing normally. Percussion should occur through the right midclavicular line from resonance over the lung field downward to dullness and from tympany over abdomen upward to dullness. Measure from upper to lower border of dullness for liver span. It is normally about 9-11 cm in the midclavicular line. 肝 脏 叩 诊 正常肝脏上界位置:右锁中线第5肋间。 肝浊音界扩大:肝癌、肝脓肿等。 肝浊音界缩小:暴发性肝炎、肝硬化等。 肝浊音界下移:肺气肿、张力性气胸等。 肝区叩痛:肝炎、肝脓肿等。 肝浊音界消失:消化道穿孔等。 Dullness extending into the normally tympanitic right upper quadrant indicates hepatic enlargement, a mass adjacent to the liver, or downward displacement of the liver. There may be an absence of liver dullness following perforation of a hollow viscus, which allows free air to enter the abdominal cavity. This indication of an intra-abdominal catastrophe must be correlated with the clinical situation, since on occasion interposition of the hepatic flexure of the colon between the diaphragm and the liver (间位结肠[结肠 位于肝与横膈之间]) will produce the same finding with no clinical consequences. 胃泡鼓音区与脾脏叩诊 Traube tympanic area (9.56cm): 上界:膈肌及肺下缘 下界:肋弓 左界:脾脏 右界:肝左缘 正常脾浊音界:左腋中线9~11肋间,长 4~7cm 脾浊音区增大:脾肿大 脾浊音区缩小:气胸、胃扩张、肠胀气等。 Percussion of the spleen To percuss for splenic dullness √This should be done when splenic enlargement is suspected. √ Normally splenic dullness can be percussed between 9 intercostal space to 11 intercostal space along left midaxillary line, the scope that is 4-7cm, without passing over left anterior axillary line. presence or absence of free fluid in the abdominal cavity (ascites) This may be detected by several maneuvers(1) shifting dullness, (2) fluid wave, and (3) elbow-knee position. 移动性浊音 (shifting dullness) 检查体位与方法: 侧卧位: >1000ml; 肘膝位 (elbow-knee position): 200500ml以上。 注意点: 肠道梗阻, 积液过多; 腹腔巨大肿瘤(如卵巢): 体位改变 (shifting dullness); 尺压试验 (ruler pressing test)。 Percussion for shifting dullness(移动 性浊音) The examiner should first tell the patient to lie on his back (in the supine position). , tympany at midabdomen could be found because of the underlying bowel. At the same time, dullness at the bilateral flanks could be found during percussion due to the accumulation of ascites. The reason is that when the patient with ascites lies on his back, the fluid will migrate into the flanks, producing dullness laterally. Percussion for shifting dullness(移动 性浊音) When dullness is found in the flanks, The line of demarcation between the dullness and tympany is marked. The examiner percusses the patient’s abdomen at the umbilicus level from the midabdomen toward the patient’s left side. If the examiner finds the point where percussion sound of tympany changes into dullness, the examiner should hold his pleximeter on that point, simultaneously, ask the patient to turn on his right side and then continue to percuss the same point again. If the sound changes from dullness to tympany, it means that the dullness has been shifted to a more dependent position. This implies that ascites is present. Percussion for shifting dullness(移 动性浊音) Similarly, the examiner percusses the patient’s abdomen toward the patient’s right side. If the examiner finds the point where percussion sound of tympany changes into dullness, the examiner should hold his pleximeter on that point, simultaneously, ask the patient to turn on his left side and then continue to percuss the same point again to confirm the shift of dullness. A volume of free fluid in the peritoneal cavity greater than 1000ml can be detected with this method. If the amount is too little, shifting dullness could not be found, the examiner could ask the patient to take elbow-knee position, letting the umbilicus at the lowest level, and then percusses the patient from flanks toward the umbilicus. If percussion sound could change from tympany to dullness, it indicates ascites. Huge ovary cyst Huge ovary cyst may also cause a large area of dullness, but at midabdomen with tympany at laterals, because bowels could be pushed to the bilateral flanks. The dullness of ovary cyst could not shift. Huge ovary cyst Ruler pressing test could be used to differentiate huge ovary cyst from real ascites. The patient should take the supine position, and the examiner puts a hard ruler on the patient’s abdominal wall horizontally and then presses the ruler downward with two hands. If huge ovary cyst exists, the pulsation of abdominal aorta will conduct to the ruler via the cyst, leading to rhythmic pulsation of the hard ruler. If free fluid not cyst exists in the abdominal cavity, the pulsation of abdominal aorta could not conduct, so the hard ruler has no such rhythmic pulsation. 膀胱叩诊: 确定膀胱内是否有尿,必要时导尿 证实。 肋脊角叩诊: 肋脊角叩痛: 肾盂肾炎、肾结石、 肾结核、肾周围炎等。 Palpation This procedure is usually the most important and often the most difficult to perform accurately. 1. the principle of palpation a) To relax the patient √ During palpation the patient should continue to lie supine with arms relaxed on the chest or at the sides. √ The examiner should make certain that his hands are warm. √ He should assure the patient that he will make an effort not to cause discomfort and follow up this assurance by avoiding at the outset an area already described as painful. √ If the patient exhibits ticklishness, the examiner should disregard it and try to continue. √ If this proves unsuccessful, it is useful to have the patient place his own hand on his abdomen, since this never tickles. √ The examiner may tentatively exert pressure on the abdomen through the patient’s own hand, and gradually increase the pressure, while assuring the patient that the examination will cause no discomfort. √ When the patient has relaxed, the examiner again places his own hand on the abdomen and allows the patient to maintain contact with his hand. This usually completes the relaxation of the ticklish patient, and the examination proceeds as usual. √ The examination begins with gentle exploration of the abdominal wall and with no effort made to palpate deeply. √ The patient may be further relaxed by instructing him to breathe slowly and deeply. √ As with inspection, the initial step in palpation may be facilitated by distracting conversation or questions regarding the history. √ If the patient remains tense or if the abdominal wall is very muscular, better results may be obtained by having the patient flex the thighs and knees. √ It should be emphasized again that during the preliminary stages muscle relaxation is the goal. At this time no attempt should be made either to elicit discomfort or to palpate for a mass or enlarged viscus. b) To palpate four quadrants superficially from LLQ counterclockwise √ To palpate all areas of the abdomen counterclockwise and superficially from left lower quadrant screening for tenseness(紧张 度), tenderness(压痛), masses, etc. √ Examination begins with gentle maneuvers and then palpation occurs more deeply. √ Examiner uses the palms of his hands with fingers together and arm relaxed and forearm on a horizontal plane. √ The examiner presses with his fingers. c) To palpate four quadrants deeply √Using the palmer surface of the fingers, examiner palpates in four quadrants to identify masses, tenderness, pulsations, etc. √ The abdominal wall should be depressed more than 2 cm. √ When deep palpation is difficult, examiner may want to use left hand placed over right hand to help exert pressure. 触诊基本方法 浅部触诊(light palpation) 深部触诊(deep palpation) 深部滑行触诊(deep slipping palpation): 腹腔包块、器官 双手触诊(bimanual palpation): 肝、脾、肾、腹腔肿物。 深压触诊 (deep press palpation): 确定腹腔压痛点与反跳痛 冲击触诊(ballottement): 适用于腹部大量积液时肝脾及腹腔包块难以触 及者。 触诊的注意点 对被检查者—— 1. 仰卧体位、曲膝、垫枕。 2. 腹部充分暴露。 对检查者—— 1.右侧站立;手臂与腹部表面同一水平 2.先左下逆时针;先正常后异常部位 3.边触诊边观察反应与表情,边谈话,减少患 者紧张 √ If a mass is suspected, determine its size, contour, mobility, tenderness, smoothness, irregularity, the hardness or softness and listen with stethoscope for a bruit over the mass. √ If there is tenderness, determine the point of maximum tenderness and distribution. √ To check for rebound tenderness, palpate deeply at the point of tenderness, pause briefly, then remove the fingers quickly. Watch the patient’s face to see whether it hurts. Then check other areas in the same manner for comparison. 压痛与反跳痛 压痛(tenderness) 腹壁与腹内病变的鉴别;检查力度。 压痛+反跳痛(rebound tenderness) 压痛的部位与范围。 压痛与全身表现。 腹膜刺激征(peritoneal irritation sign) 2. the contents of palpation a) abdominal tenseness腹壁紧张度 In normal persons, abdominal wall is somewhat tense, but usually soft when palpated and easily depressed , and is called abdominal softness(腹壁柔软). While some pathological conditions can lead to an abnormal increase or decrease of abdominal tenseness. 1) The increase of abdominal tenseness √ Abdominal tenseness increases, not accompanyed by muscle spasm, is due to the increase of abdominal contents, as gastrointestinal flatulence(肠胃胀气), artificial pneumoperitoneum(人工气腹), ascites, etc. Board-like rigidity板状腹 √ If abdominal wall is palpated as obviously tense, even as rigid as a board, board-like rigidity is so called. √ This sign is caused by the spasm of abdominal muscle due to peritoneal irritation, as the perforation of the gastrointeatinal diseases or rupture of the viscera. Dough kneading sensation 揉面感;柔韧感 √ If abdominal wall is palpated as pliable and tough, and if it has resistance and is not easily depressed, then the examiner feels the sensation of dough kneading. √ This sign is usually seen in tuberculose peritonitis or cancerous peritonitis. The decrease of abdominal tenseness √ caused by the decrease or disappearance of abdominal muscle’s tension(张力), the sign usually found in chronic deeline(消耗性疾病) or drainage of large amount of ascites tenderness and rebound tenderness 压痛和反跳痛 √ After relaxation is obtained, the examining hand is first moved gently over the entire abdomen, and an estimate of the muscle tone in the various quadrants is made. √ Following general palpation an attempt should be made to detect and localize any painful area (i. e. tenderness) within the abdomen. √ Two types of pain may be elicited by palpation. 1. Visceral(内脏的) √ arises from an organic lesion or functional disturbance within an abdominal viscus √ For example, it is the type seen in an obstructive lesion of the intestine in which there is a buildup of pressure and distention of the gut. √ sveral characteristics: dull, poorly localized, and difficult for the patient to characterize 2. Somatic(躯体的;体壁的) √ similar to the distress noted in painful lesions of the skin √ sharp, bright, and well localized. √ not caused primarily by involvement of the viscera √ indicates involvement of one of the somatic structures, such as the parietal peritoneum or the abdominal wall itself √ an inflammatory process originating in a viscus will produce visceral pain that may extend to involve the peritoneum. √ Inflammation of the peritoneum would then result in somatic pain. √ best illustuated by appendicitis(阑尾炎) in which the pain is at first poorly localized, dull, ill defined, and primarily midiline (when it is entriely visceral in origin). Later, as the inflammation spreads to the peritoneum, the pain becomes sharp, bright, and well localized in the right lower quadrant over the involved region. √ After a painful area is located, the examiner should determine whether the pain is constant under the pressure of the examing hand or if it is transient, tending to disappear even though pressure is continued over the area. √ Pain caused by inflammation usually remains unchanged or increases as pressure is applied. Visceral pain as the result of distention or contraction of a viscus tends to become less severe while pressure is maintained. √ Occasionally the examiner may have difficulty in distinguishing visceral pain from that arising in somatic structures, such as the spine and abdominal wall. An example of abdominal wall discomfort is seen in patients with fibrositis(纤维组织炎). These types of pain may be differentiated by having the patient tense his abdominal muscles, which may be accomplished by forcefully elevating his head while keeping his shoulders flat on the table. √ Under these conditions increased tension of the abdominal wall will accentuate the pain if it originates in somatic structures. √ On the other hand, discomfort from intraabdominal sources will be less severe with the abdomen tense than when relaxed. √ When pain has been elicited, the examiner should test for the phenomenon of rebound tenderness. √ This is found only when the peritoneum(壁层 腹膜) overlying a diseased viscus becomes inflamed. √ Although it may be produced in different ways, the most common is to press firmly over a region distant from the tender area and then suddenly release the pressure. The patient will feel a sharp stab of pain in the area of disease if true rebound tenderness is present. √ pressure applied in the right lower quadrant and then suddenly released will cause a marked increase in pain over an area of diverticulitis(憩室炎) in the left quadrant √ Rebound tenderness may also be elicited by having pressure over the tender area and having the patient cough or strain. √ Marked tenderness to percussion in the area is usually seen in this situation. √ At times, if the area involved is small, rebound tenderness may be elicited only over the most tender area of the abdomen. Palpation of Viscera ----- liver u To palpate liver at midclavicular and midsternal lines 腹部脏器触诊 肝脏触诊 方法: 单手触诊法 双手触诊法 钩指触诊法 肝脏触诊手法的注意点 四指并拢,食指前端桡侧(非指尖)接触 肝脏。 右锁中线、前正中线为描述部位。 腹直肌外缘稍外。 密切配合呼吸运动,吸气时手指上抬速度 落后于腹壁抬起,呼气时手指下压提前于 腹壁下陷。 大量腹水——冲击触诊。 不要误判(腹直肌腱划、肾、胃肠病变)。 Method: The right hand may be held either parallel or perpendicular to the long axis of the patient. In the midclavicular starting at the anterior superior iliac crest, examiner presses down firmly and asks patient to inhale deeply. This allows the liver to move down to meet your fingertips. √ If you feel nothing, press up a few centimeters toward the rib cage and repeat the maneuver. Do this continuously until you feel the liver or reach the coastal margin. √ Normally the liver is not palpable, but sometimes the examiner may feel the edge of the normal liver at or slightly below the right costal margin. √ When the liver is palpated, a firm edge will strike the fingers upon inspiration. √ In the midsternal line, from the level of the umbilicus, repeat the above maneuvers to palpate the liver. √ Most doctors like to use bimanual maneuvers to palpate the liver. To do this, place the left hand at right lower posterior chest wall parallel to, or supporting patient’s right 11-12th ribs or at lower sternal area to limit the chest respiration to make right hand palpation more effective. Note: (1)When felt more than 2cm. below the costal margin, however, the organ should be considered abnormally large. √ An exception is a congenitally large right lobe of the liver, which occasionally extends quite far into the right flank. √ Another exception is seen in severe, chronic emphysema(肺气肿), in which the diaphragms are depressed by the overexpanded lung, displacing the liver below the costal margin. In both instances the total mass of the liver is within normal limits. (2)If you feel the liver, detect the edge (sharp or round), tender or not, hard or soft and repeat the process laterally and medially to define the contour. For masses within the liver, describe the same characteristics as above and listen for a bruit over the mass. l Size √ Ordinarily the liver is not palpable, or the liver can not be felt more than 2cm below the lower coastal margin, and can not be felt more than upper 1/3 distance of the line from xiphoid to umbilicus or more than 3cm under the xiphoid. √ Failure to feel the liver does not mean that the liver is normal. √ Measurement of the liver is done in the midclavicular line and midsternal line. l Texture/quality质地 √ The quality of liver is classified into three grades: softness(质软), toughness(质韧), and hardness(质硬). √ Normally the quality of liver is soft and tender, just like the pouted(撅嘴) lip. √ In acute hepatitis or fatty liver(脂肪肝), the quality of liver is slightly tough. In chronic hepatitis or blood stasis of liver, liver is more tough and usually as tough as apex nasi(鼻尖). √ In liver cirrhosis, the quality of liver is hard. In liver carcinoma, the quality of liver is extremely hard or even as hard as forehead(前额). l Surface and edge √ To observe whether the surface of liver is smooth or not, whether there is any node(结节) or not, and whether the edge is thin or thick and is regular or irregular. The character of the surface of the liver should be described. √ Sometimes large metastatic masses may be present and palpable in the liver. √ In some persons with cirrhosis, the anterior surface of the liver will have a granular feel. This is easily felt in the thin individual. l Tenderness Normally liver cannot be palpated as tenderness unless the liver is irritated by the liver chitonitis (that is, inflammation of the diolame包膜 of the liver) or pulled by the enlargement of itself. l Pulsation搏动 √ Normally you cannot palpate any pulsation of the liver. √ If you palpate the pulsation of the liver, you should pay attention to its direction, that is, whether it is unidirectional(单向性) or expansile(扩张性). √ unidirectional pulsation is usually a conductive one(传导性搏动), caused by the the conduction of the pulsation of aorta abdominalis(腹主动脉). √ If you put your hand on the sufface of the liver, you will feel your hand is pushed upward. √ expansile pulsation is the pulsation of the liver per se and usually found in tricuspid valve insufficiency(三尖瓣关闭不全). √ Because the contractive pulsation of right ventricle conducts to liver through right atrium and then inferior vena cava. If you put your hand on the sufface of the liver, you will have the opening-closing sensation. The positive Hepatojugular reflux sign(肝- 颈静脉回流征): If you press the liver, you will find the dilated jugular vein becomes more bulged or distended, as from the enlargement of liver passive congestion resulted from right failure. l Liver friction sensation肝区摩擦感 l Liver thrill肝震颤 肝脏触诊判断描述的内容 大小 质地 表面与边缘 压痛 搏动(单向性.扩张性) 摩擦感 肝-颈回流征(hepatojugulor reflux) u To palpate spleen from umbilicus to left costal margin 脾 脏 触 诊 手法和体位; 脾脏测量三线法; 脾肿大的鉴别(左侧肾、肝、胰、 结肠); 脾肿大意义。 √ In examining for splenic enlargement, the examiner should stand at the patient’s right side. √ His left hand is placed over the patient’s left costovertebral angle, exerting pressure to move the spleen anteriorly. At the same time his right hand is worked gently under the left anterior costal margin. √ With the examiner’s hands stationary in this position, the patient is instructed to take a deep breath. √ If there is significant enlargement of the spleen, it will be palpated as a firm mass that slides out from under the ribs, bumping against the finger of the examiner’s right hand. √ The spleen normally moves down with inspiration. √ If splenic enlargement cannot be felt by the technique just described, the patient should then be rolled slightly toward the right so that the spleen may fall anteriorly . √The examining hands are again placed as described and the procedure is repeated. Occasionally a spleen that cannot be felt with the patient in the supine position may be palpated by this maneuver. √ When the spleen can be felt, it must be considered abnormal, since the normal spleen is not palpable. Notes: (1) Starting from the level of the umbilicus (or below the percussed dullness). (2) The maneuver is similar to that used to palpate the liver, but is more subtle because the spleen is more mobile and deeper than the liver. (3) If the spleen is not palpated, have the patient roll on his right side and repeat palpation. (4)Measurement of the spleen is the same as that of the liver and is usually expressed as centimeters under the costal margin in the midclavicular and under the xiphoid process in the midsternal lines. (5) A moderately or greatly enlarged spleen is best described by a drawing, especially the three lines which are presented schematically in the following diagram . (NOTE: Severe splenomegaly may cause rupture when spleen is vigorously palpated, so palpate gently and carefully). Line 1: The distance between left costal border and the lower edge of spleen along left midclavicular line Line 2: The distance between the crossing point of left midclavicular line and left costal border and the most remote point of the spleen Line 3: (when the spleen is extremely large and exceeds the anterior midline.) The distance between the right border of the spleen and the anterior midline. If the spleen indeed exceeds the anterior midline, The mark “+” is used to indicate “exceeding”, while “ – “ is used to indicate “not exceeding”. In clinical practice, splenomegaly is classified into three levels: level 1 (slight enlargement轻度肿大): During deep respiration, the lower edge of spleen is not more than 2cm below the costal border level 2 (moderate enlargement中度肿 大): During deep respiration, the lower edge of spleen is more than 2cm below the costal border but above the umbilical horizontal line level 3 (severe enlargement高度肿大): During deep respiration, the lower edge of Spleen is below the umbilical horizontal line or over anterior midline 脾脏肿大的意义 轻度肿大:急慢性肝炎、SBE、败血症、重 症结核、伤寒、急性疟疾等; 中度肿大:肝硬化、慢淋、慢性溶贫、淋巴 瘤、SLE、等; 高度肿大:慢粒、骨髓纤维化、慢性疟疾、 黑热病。 u To palpate gall bladder 胆 囊 触 诊 胆囊触诊的方法: 必需记住的两个重要体征: Murphy’s sign Courvoisier’s sign Method: Put right hand below the costal margin or lower border of liver at midclavicular line (grossly equal to the lateral border of the right rectus muscles) and palpate deeply to check for tenderness or bulging. √ Under normal circumstances, the gallbladder cannot be palpated. √ However, in a jaundiced patient, the right upper quadrant should always be carefully palpated for a soft, cystic mass, approximately 6 to 8 cm in diameter , which appears to be attached to the liver and moves with respiration. This is an exceedingly valuable sign in differentiating jaundice caused by cancer of the head of the pancreas or the common bile duct from that caused by gallstones. √ In the presence of tumor of the common bile duct or head of the pancreas, the wall of the gallbladder is normal, and consequently the organ is capable of distending to the point that it is palpable. Such sign is named Courvoisier sign. √ If the obstruction is caused by gallstones, the gallbladder wall is inflamed, and this diseased organ is not capable of distention. Therefore, the gallbladder will not become palpable. u sign To check for Murphy’s √ If pain is found in the gallbladder area but gallbladder is not palpated , the examiner should put his left hand on the lower lateral rib cage with the 4 fingers stretching superiorly and the thumb hooked under the costal margin. √ Press down to the point of gallbladder tenderness and ask the patient to breathe deeply and check to see whether the patient stops breathing, changes facial expression, or complaints of pain. √ The sign indicates the inflammation of gallbladder. u To palpate kidneys bimanually 肾 脏 触 诊 方 法: 尿路感染的5个压痛点: 前3: 季肋点;上、中输尿管 点; 后2: 肋脊点;肋腰点。 √ For palpation of the kidney, examiner puts his left hand below left rib cage, at the costospinal angle, and lifts up. Examiner uses his right hand to palpate deeply from umbilical level in the left midclavicular line, and moves progressively upward. The lower pole of the kidney may be felt as a smooth, round, and deep structure that moves relatively little with respiration. √ This maneuver is repeated on the right side to palpate the right kidney. √ Normally the kidney is not palpated. Sometimes the lower pole of the right kidney may be felt in normal patients. √ During deep inspiration, if more than half of the kidney is palpated, nephroptosis(肾下垂) is considered. √ Repeat the maneuver with the patient in sitting and standing positions if you wish to expose the kidney further. 关于膀胱触诊 只有尿潴留时才可以触到膀胱; 非常容易与增大子宫、卵巢肿块等 鉴别。 d) abdominal masses 腹部正常包块 腹直肌肌腹及腱划 腰椎椎体及骶骨岬 乙结肠粪块 横结肠 盲肠 腹部异常包块 位 置 大 小 形 态 质 地 压 痛 搏 动 移 动 度 Fluid wave thrill (液波震颤) With patient lying on his back, the examiner’s left hand is placed against the patient’s right flank. An assistant or the patient places the ulnar edge of one hand lightly against the middle of the abdomen to prevent the transmission of any wave through the tissues of the abdominal wall. The examiner’s right hand then lightly taps the left flank of the patient. Fluid wave thrill In the presence of a siguificant amount of ascites, a wave will be transmitted through the fluid that will be felt against the examiner’s left hand as a sharp impulse. This finding is present only when there is a reasonably large amount of fluid, usually 3000-4000 ml. So the fluid wave thrill is not so sensitive as shifting dullness. succussion splash振水音 Succession splash is the splash sound over the upper abdomen. It should be checked by rocking the upper abdomen to the left and right. In normal patients this is negative about 6-8 hours after eating food. If positive, it indicates gastric retention. 振水声与液波震颤 液波震颤(fluid wave thrill,fluctuation) 液体震动传向对侧的波动感;敏感 性差于移动性浊音。3000~4000ml。 振水声(succussion splash) 幽门梗阻的特征表现,确诊依据。 空腹6小时以上。 腹部触诊的特殊手法 1.腰大肌试验(iliopsoas test) 2.闭孔内肌试验(obturator maneuver) 3.牵涉性触痛(referred tenderness) 4.结肠充气试验(Rovsing试验) 5.腹主动脉触诊 腹部异常发现及其鉴别 1.腹水 2.腹部肿块 3.肝肿大 4.脾肿大 腹 水 1.病因 心血管系统疾病 肝脏及门脉系统疾病 肾脏疾病 腹膜疾病 营养缺乏 淋巴系统疾病 女性生殖系统疾病 腹腔脏器破裂 其他:黏液性水肿、Meig综合征 发生机制 液体静水压增加 血浆胶体渗透压下降 淋巴回流受阻 肾脏因素 诊断与鉴别 1.确定是否有腹水 2.腹水的类型和病史 病史: 体检: 实验室检查和特殊检查:腹水检 查(渗出液与漏出液)、其他检 查。 渗出液与漏出液鉴别 漏出液 渗出液 外观 清或微浑 浑浊 细胞数 <100106/L >500106/L 比重 <1.018 >1.018 蛋白定量 <25g/L >30g/L SAAD >11g/L <11g/L 腹部肿块 常见病因: 炎症性: 肿瘤性: 梗阻性: 先天性: 症状与体征 1.症状: 2.体征: 全身检查: 腹部检查:视、触、叩、听 诊断与鉴别 1.病史资料 2.是否腹部肿块 3.肿块的来源:腹壁内、外。 4.肿块的病理类型:炎症性、肿瘤性、 梗阻性、先天性、 损伤性 腹部包块诊断步骤 腹壁 腹块 普通外科 活检、手术 实质脏器 超声、CT、MRI 空腔脏器 内窥镜、BE、GI 腹腔 肝肿大 病因与发病机制: 1.感染: 2.中毒性、药物性肝炎: 3.瘀血: 4.瘀胆: 5.代谢异常: 6.肿瘤: 7.血液病: 8.其他:免疫损伤 诊断与鉴别 1.病史: 2.体征:程度、质地、表面、触痛、 搏动、肝区摩擦音 3.伴随症状与体征: 4.实验室检查和特殊检查:WBC、肝功、 三对半、肿瘤标记、B超、X线、肝 穿、腹腔镜等。 脾肿大 病因与发病机制: 1.感染性疾病: 病毒感染: 细菌感染: 螺旋体感染: 寄生虫感染: 立克次体感染 2.非感染性疾病:脾瘀血: 血液病: 结缔组织病: 其他: 诊断与鉴别 1.病史: 2.体征:程度、质地、表面、触痛、 搏动、肝区摩擦音 3.伴随症状与体征:贫血、黄疸、肝肿大、 皮肤表现、脾区压痛。 4.实验室检查和特殊检查:血象、肝功、 粪便检查、骨髓检查、病原体分离和免疫 学检查、B超、核素检查、脾穿刺检查等。 Case A 57-year-old female patient was admitted on Jan. 20th 2003 because of “fatigue and anorexia for 2 months, abdominal swelling and oliguria for half a month”. Two months before, the patient began to feel fatigue, decreased tolerance of physical activities and anorexia without any identifiable causes. She used to eat 100g rice every meal, but now she could only eat 50g. She also had low fever and felt better after taking anti-cold medications. Case Half a month before, the patient began to feel abdominal swelling. Her pants’ waist belt became tight for her. Urine volume decreased to 500 ml everyday and the color was dark. Then the patient went to the district hospital nearby and took the abdominal ultrasound examination. The result showed she had liver cirrhosis, splenomegaly, and large volume of ascites. The patient had acute hepatitis B 20 years ago. During the years after the acute infection, her liver function was abnormal intermittently. Case She had no habit of smoking and alcohol. She was married and had one son and one daughter. Her daughter and husband were both healthy. Her son had hepatitis B infection. Her father died of primary hepatic cancer. Her mother is still alive. Case Physical Examination: T: 37.5C, BP:16/10KPa, R:18/min, HR: 100/min. Conscious, hepatic face, mild jaundice of sclera, liver palm(+), spider angioma on left neck, no palpation of lymph nodes, lung auscultation negative, heart (-). Abdominal findings: obvious abdominal bulge (marked protuberance of the abdomen), no distention of abdominal wall veins, soft, no pain, shifting dullness(+), normal active intestinal sound, moderate edema of the lower limbs, NS(-). CLINICAL THINKING According to the patient’s symptoms, physical signs and the result of the abdominal ultrasonography, we confirmed the diagnosis of ascites. Among the causes of ascites, liver cirrhosis accounts for 80% while other causes such as cancer, heart failure, tuberculosis, renal disease and pancreatic disease account for 20%. Because the patient had the history of hepatitis B infection and the abdominal ultrasonography also suggested liver cirrhosis, the cause for this patient’s ascites was most likely secondary to liver cirrhosis. CLINICAL THINKING To ascertain the cause of ascites is very important for the diagnosis and treatment of ascites. Before we start the treatment, diagnostic paracentesis is necessary. According to the analysis of ascites, including routine tests, biochemical tests, and etiological tests, we could further verify the cause of ascites and make differential diagnosis of simple ascites of liver cirrhosis and ascites of cirrhosis with spontaneous bacterial peritonitis. CLINICAL COURSE Blood test showed WBC 2.3×109/L, RBC 3.5×1012/L,Hb95g/L, BPL45×109/L. Liver function test showed TB/CB 21/37μmol/L, A/G 32/49g/L, ALT 75U/L, AST 94U/L. Serologic tests for hepatitis B showed HBsAg(+), antiHBe(+), anti- HBc(+), others(-). A diagnostic paracentesis was performed on the day of admission and the analysis of the ascitic fluid was as follows. CLINICAL COURSE Routine tests showed the fluid was clear in appearance, an absolute RBC count of 10/μL and a WBC count of 25/μL. Biochemical tests of the fluid showed protein concentration of 5g/L,albumin concentration of 2g/L and gravity of 1.010. Culture for bacteria showed negative result. Cytology study of the fluid was also negative. CLINICAL THINKING The patient’s blood test showed that the blood counts were low. This is consistent with the diagnosis of liver cirrhosis and hypersplenism. The patient’s liver function test showed a reversed ratio of albumin to globulin, mild hyperbilinemia and elevated transaminases. This is also consistent with the decompensated stage of liver cirrhosis. Serologic tests in hepatitis B suggested that the cause of liver cirrhosis was chronic hepatitis B infection. All the laboratory tests further confirmed the diagnosis of liver cirrhosis. CLINICAL THINKING For this patient with ascites, the most valuable examination is paracentesis. Let’s go over the standard in the differential diagnosis of ascites. According to the traditional standard, ascitic fluid can be divided into exudate or transudate. CLINICAL THINKING Transudate is characterized by clear appearance, protein concentration <25g/L, gravity <1.018, cell count <100/μL and negative bacteria culture, whereas exudate is characterized by cloudy appearance, protein concentration >25g/L, gravity >1.018, cell count >500/μL and often with positive bacterial culture. CLINICAL THINKING Transudate is often caused by liver cirrhosis, heart failure and renal disease. Exudate is more often caused by tumor, tuberculosis and pancreatic disease. The transudate ascitic fluid could become exudate when spontaneous bacterial peritonitis occurs. It is obvious that the analysis of this patient’s ascitic fluid confirms its classification as transudate. CLINICAL THINKING Serum ascites albumin gradent [(SAAG) = (32-2)g/L =30g/L(>11g/L)] in this patient indicated that the ascites was due to portal hypertension. Therefore, the diagnosis of liver cirrhosis with ascites could be confirmed. Thanks for Your Attention