Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
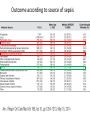
Approach to the patient with sepsis: infectious causes and antimicrobial management Morgan Hakki August 11, 2016 Infection as a cause of sepsis • ~50% of patients meeting criteria for sepsis are found to have an infectious cause – ~95% of patients with bacteremia meet criteria for sepsis, severe sepsis, or septic shock • Pneumonia and GU sources most common in persons presenting to the ER with sepsis: In hospitalized patients, think of: • • • • Line-associated (CLABSI) bacteremias Catheter-associated UTI (CAUTI) Pneumonia Gut – neutropenic hosts Microbiologic epidemiology of healthcare associated infections (HAIs) in the US 2009-2010 CLABSIs #1 source of HAIs Staph aureus single most common pathogen in HAIs Predominance of gram positives in CLABSIs Predominance of gram negatives in CAUTIs, VAP Epidemiology of Gram Negative bacteremia at OHSU E. Coli, Klebsiella Pneumoniae Pseudomonas aeruginosa Enterobacter cloacae Decreasing incidence Acinetobacter spp Serratia marcescens Proteus Mirabilis Stenotrophomonas maltiphilia Fusobacterium Klebsiella oxytoca Bacteroides fragilis Citrobacter Freundii Leptotrichia spp Capnocytophaga Sphingomonas paucimobilis Moraxella Spp Pantoea spp Enterobacter gergoviae Ralstonia mannitolitylica Morganella Morganii Citrobacter youngae Raoultella planticola Kluyvera intermedia Leclercia adecarboxylate Serratia liquefaciens Campylobacter spp Ochrobactrum anthropi Pseudomonas fluorescans Raoultella ornithinolytica Achromobacter spp Courtesy of Rob Zimmerman Proteus vulgaris Unable to be identified Why does the source of infection matter? – Determines empiric coverage based on expected pathogens – Source control is critical to successful outcome • Drain abscesses • Pull CVCs • Debride necrotizing fasciitis – Association with mortality • GI, Pulmonary: 50-55% • Urinary tract: 30% Outcome according to source of sepsis Antibiotic therapy • The administration of effective intravenous antimicrobials, ideally within the first hour and at most w/in 6 hours, should be the goal of therapy. – Each hour delay in achieving administration of effective antibiotics is associated with a measurable increase in mortality in a number of studies – Time To Administration of appropriate antimicrobial therapy one of the strongest predictors of outcome Time to antibiotic administration and outcome Which antibiotics to use? It’s important to get it right the first time! Inappropriate empiric therapy associated with worse outcome Who gets inappropriate therapy? Lots of people: up to 40% in studies; 15-30% at OHSU MRSA MRSA and VRE often not covered in empiric regimen when indicated E coli covered appropriately more VRE often than other organisms Which antibiotics to use? • Consider: – the most likely source/clinical syndrome – drug allergies – recent receipt of antibiotics • Especially important in heavily abx exposed Heme/Onc/BMT – underlying diseases – susceptibility patterns of pathogens at OHSU – documented prior colonizers or infections Which antibiotics to use? • Initial selection of antimicrobial therapy should be broad enough to cover all likely pathogens. • It is generally not an appropriate strategy to restrict antibiotic administration in the initial therapy for this patient population. • As soon as the causative pathogen has been identified and susceptibilities known, de-escalate by selecting the most appropriate antimicrobial agent that covers the pathogen, is safe and costeffective. Resistance of select pathogens in the US 2009-2010 40-50% of Staph aureus = MRSA Note relatively high rate of MDROs among certain GNs – implications for empiric therapy in the septic patient Resistance among common GNs in US, 2009-2012 Note high rates of P aeruginosa resistance to imipenem E coli very sensitive to carbapenems Will vary from institution to institution: appropriate empiric therapy requires knowledge of institution’s antibiogram OHSU Antibiograms https://o2.ohsu.edu/pharmacyservices/antibiograms.cfm A word about extended-spectrum beta-lactamase (ESBL) gram negatives • Enzymes that confer resistance to most betalactam antibiotics, including penicillins, cephalosporins, and aztreonam • Found exclusively in gram negative organisms – Klebsiella spp (K pneumoniae, K oxytoca) – E coli – Others: • Enterobacter • Proteus • Acinetobacter Rates vary widely across US Highest on East Coast Relatively low in Northwest US Management of ESBL gram negatives • The only current proven empiric therapeutic option for severe infections caused by ESBLs are carbapenems – No clear difference between imipenem and meropenem • Empiric therapy with cefepime or piperacillin/tazobactam associated with higher mortality than empiric therapy with carbapenem (Chopra et al, AAC, 2012; Tamma et al, CID, 2015) • OK to change coverage once susceptibilities known Pharmacology considerations Bacteriostatic vs bactericidal “static” = prevents growth; “cidal” = kills bacteria Some can be both: At high concentrations, static agents can be cidal Macrolides generally static but cidal vs Strep pneumoniae Linezolid cidal against Strep spp; static against Staph and ECOC Historically, cidal agents have been preferred in acutely life-threatening diseases: meningitis, endocarditis, bacteremia (daptomycin) (tigecycline) (clindamycin) (linezolid) Not all bactericidal agents are created equally! Superiority of beta-lactams over vancomycin for MSSA infections No efficacy difference cefazolin vs nafcillin for MSSA bacteremia Although cefazolin better tolerated! Pharmacology considerations Time vs concentration dependent killing: basis for prolonged/extended beta-lactam infusion concentration dependent time dependent Prolonged infusion beta-lactam antibacterial therapy • Rationale: – beta-lactam antibiotics demonstrate time-dependent killing – prolonged infusion may improve microbiologic and clinical cure by increasing the time spent over the MIC of the organism compared to intermittent dosing – Intuitively useful when pathogens demonstrate higher MICs – Can be done as 24 hour continuous infusion or extended infusion over 3-4 hours – Hey, yeah, that’s really interesting but does it work in real life? Not powered to detect survival effect Prolonged infusion of beta-lactams: • No clear answers yet – Studies limited by small size, heterogeneous patient populations, mixed microbiology, endpoints • If benefit, likely limited to – certain organisms: P aeruginosa or organisms with high MICs, or – particularly vulnerable populations (immunocompromised hosts) • No obvious toxicities noted • Currently being done routinely in ICU for piperacillin/tazobactam only – Not yet cefepime, carbapenems What about combination therapy? • Why use combination therapy: – Delay emergence of resistance: TB, HIV – Synergistic activity -> better outcome : amp+gent for enterococcal endocarditis – Improve likelihood of picking the right agent: if you have a high rate of Multi Drug Resistant Organisms What about combination therapy? • Combination therapy for suspected or known Pseudomonas aeruginosa or other multidrug-resistant Gram negative pathogens, pending susceptibility results, increases the likelihood that at least one drug is effective against that strain and positively affects outcome – Overall benefit depends on local rate of resistance • At OHSU, relatively low rates so utility of combination therapy is limited – Overall benefit may also depend on the host: neutropenic patients with overwhelming gram negative sepsis – Addition of tobramycin should be considered in neutropenic hosts with suspected or proven gram negative sepsis • Once sensitivities are known, clinical trials indicate that there is no reason to continue combination therapy for GNRs - monotherapy with appropriate antibiotic is fine (Cochrane Review 2014; Lancet Inf Dis August 2004) – Exception: aminoglycoside monotherapy generally not recommended So what’s doing in the Micro lab? A word about Verigene • Background – Brought to OHSU May 2014 – An automated rapid nucleic acid test – Run after blood culture trips + • Run on either gram positive or gram negative machine depending on gram stain • Turn-around time of ~1-2 hours Verigene – Gram negatives Detectable Organisms Acinetobacter spp. Enterobacter spp. E. Coli Klebsiella oxytoca Klebsiella pneumoniae Citrobacter spp. Proteus spp. Pseudomonas aeruginosa • Gram negatives not detected: – Stenotrophomonas – Serratia – Anaerobes • Fusobacterium • Bacteroides Verigene – Gram negative resistance markers 1. CTX-M (ESBL) 2. Carbapenemases • Due to variety of resistance mechanisms present in gram negatives, absence of molecular resistance marker in Verigene report does not necessarily predict sensitivities by traditional phenotyping so generally advisable to wait for sensitivity report before changing therapy if your patient is doing well – Presence of resistance marker should influence choice of antibacterial agent while awaiting phenotypic sensitivity report Verigene – Gram positivies • • • • • • • Not detected: Detected: – Misc enterococcus spp Listeria – Misc Strep spp Staph aureus – Micrococcus Coag Neg Staph Resistance markers: E faecalis, E faecium 1. mecA (methicillin resistance Staph) 2. vanA, vanB (vancomycin resistance Strep: Enterococcus) – Pneumoniae Limited number of resistance mechanisms in gram positives so – Pyogenes (GAS) absence of these in molecular testing is – Agalactiae, anginosus more reliable predictor of final susceptibilities compared to gram negatives GRAT question 1 • Which of the following statements pertaining to healthcare associated infections (HAIs) is true? A. The majority (>50%) of bacteremic episodes are caused by gram negative bacilli B. Coagulase negative staphylococci are the single most common cause of CLABSIs C. Klebsiella pneumoniae is the organism most commonly isolated in the setting of a CAUTI D. Candida species are a common cause of VAP GRAT question 2 • Which of the following bug/drug combinations is most appropriate before having results of formal susceptibility testing when treating a bacteremic patient? A. B. C. D. E. Staph aureus: nafcillin E coli: levofloxacin Enterococcus faecalis: ampicillin Enterobacter cloacae: piperacillin/tazobactam Enterococcus faecium: ampicillin GRAT question 3 • Which of the following is true? A. A microbiologic diagnosis will be definitively made in the vast majority (80-90%) of patients with clinical sepsis B. Skin/soft tissue infections are the most common source of sepsis in patients presenting to ERs from the community C. Urosepsis is associated with mortality rates of 50-60% D. Sepsis of GI tract/abdominal sources is associated with the highest mortality rates compared to other sources E. Delaying initiation of appropriate antibiotic therapy is not a factor in overall outcome since our supportive care measures are so good GRAT question 4 • You are taking care of a patient whose blood cultures are growing an aerobic gram negative rod that was not identified by Verigene. Which is the most likely? A. Pseudomonas aeruginosa B. E coli C. Bacteroides fragilis D. Fusobacterium E. Stenotrophomonas maltophilia GRAT 5 • Which of the following statements regarding therapy of gram negative rod bacteremia is true? A. Combination beta lactam + aminoglycoside therapy improves mortality compared to beta lactam monotherapy when treating sepsis due to infection with a beta lactam susceptible organism B. Prolonged/extended infusion of beta lactams has been conclusively demonstrated to improve survival compared to standard intermittent dosing C. Empiric therapy with either cefepime or piperacillin/tazobactam for an isolate identified as an ESBL by molecular testing is appropriate pending susceptibility testing D. Prolonged/extended infusion of beta lactams has demonstrated improved rates of microbiologic and clinical cure of infection compared to standard intermittent dosing