Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Heart failure wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Jatene procedure wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Coronary artery disease wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Electrocardiography wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Intensity
of Heart
Sounds
of Patients
following
Paul D. Stein,
F.C.C.P.;
amplitude
sured
at the
cardial
and
Myocardial
Hani
intensity
wall
chest
infarction
clinical
N. Sabbah,
in
of heart
in 25
order
sounds
were
mea-
with
acute
myo-
patients
to
determine
what
mean-
information
lthouh
physicians
tensity
have
with
usefulness
recently,
heart
sounds
the
observe
following
association
reduced
the
and
of diminished
contractile
(S2)
performance
the
heart
performance,1-3
in patients
has
been
primary
intensity
of
gradient
across
Until
second
poor
ventricular
We
now
at
the
which
valve
by the
the
after
rate
tion
reflects
impaired
ventricle.5
The
isovolumic
rate
ventricle
also affects
the
component
of the second
heart
sounds
anism,
then
are
produced
one
may
by
presume
of
intensity
sound
the
at
the
44th
College
Nov 1, 1978.
Manuscript
received
ber30.
Reprint
requests:
Dr.
Detroit
48202
Annual
October
19; revision
accepted
CHEST, 75: 6, JUNE, 1979
HospItal,
early
this
ventricle,
period
after
infarction
to relate
in mind,
it
of the intensity
wall
reflects
the
with
the
potential
guide
To
myocardial
measured
(maxi-
in dogs
background
auscultatory
cardiac
function.
following
were
shown
if observation
the
thoracic
of the
patients
sounds
been
With
as a meaningful
evaluation
of
in
period
S1 has
maximal
pressure
at
infarction,
the
and
of
to the
explore
chest
again
wall
during
in
the
of recovery.
of
Henry
by
of the
DC,
Novem2799
MATERIALS
ANt)
METHODS
If
mech-
Assembly
Washington,
Ford
the
intensity
Scientific
Physicians,
Henry
the
of the
of Chest
Stein,
this
(P2 ) .
#{176}Fromthe Departments
of Medicine
and Surgery,
Ford Hospital,
Detroit.
Supported
in part by grant R38820
from funds supplied
Henry
Ford Hospital
via a Ford Foundation
grant.
Presented
American
The
to the rate of
across
the
by the
of isovolumic
dp/dt.9
state
relates
gradient
is approximated
to determine
sounds
at
serving
clinical
heart
(Si)
also
pressure
of
a universal
that
dp/dt).
functional
relaxation
which
mal
know
deterinfarc-
relaxation
valve,
of development
of the
closure.58
sound
of the
rate
is useful
of heart
of isovolumic
isovolumic
of
the first heart
development
to maximal
pressure
In view of this, it has now been
the diminished
S2 in myocardial
the 19 patients
who showed
an increase
in A2, the
PEP/LVET
decreased
(improved)
(P < 0.02),
and
the rate of isovolumic
relaxation
increased
(P < 0.001).
Blood
pressure
did not change.
The diminished
A2, as
shown
by recently
described
mechanisms
of production
of the second
heart sound,
is due to a reduction
of left
ventricular
isovolumic
relaxation.
Similarly,
the reduced
P2 implies
that
right ventricular
isovolumic
relaxation
also was affected
by the infarction.
Variations
of Si seem
to relate to variations
of the left ventricular
contractile
state.
The results
of this study
indicate
that The intensity
of heart
sounds
at the chest
wall
in patients
with
normal
valves
and normal
transmission
of sound
is measurably
diminished
in patients
following
myocardial
infarction.
Noticeable
ausculatory
variations
of the intensity
of heart sounds
can serve
as a meaningful
guide to the
evaluation
of ventricular
performance
at the bedside.
mitral
the
determinant
rate
determined
left
the right
pulmonary
unclear.4’5
the
develops
is largely
relaxation.5’8
mined
that
with
hemodynamic
S2 is
in-
infarction
of this sign has been undetermined.
even
the cause
of the diminished
sound
that
traditionally
of heart
recognized
sounds
Grand,
lnfarction*
B.S.; and
can be derived
from observing the intensity
of the heart sounds.
During
the early
period
after infarction,
the first heart sound (Si), the aortic
component
of the second
heart sound (A2), and the pulmonary
component
of the second
heart sound (P2) each
were lower (P <0.001)
than the respective
heart sounds
of 23 normal
subjects.
Measurable
reductions
of sounds
frequently
occurred
in the absence
of a third heart sound
or rales. Prolongation
of the ratio
of the preejection
period
over the left ventricular
ejection
time (PEP/
LVET)
(P < 0.001)
and a reduced
rate of isovolumic
relaxation
(P < 0.001)
accompanied
the reduced
heart
sounds.
During
the course
of recovery,
the average
intensity
of A2 increased
in 19 of 25 patients.
Among
ingfUl
This
Evaluation
Barr, M.D.
Isaac
The
M.D.,
in the
West
The intensity
of heart sounds
was measured
repetitively
by
calibrated
phonocardiograms
in 48 subjects;
25 were patients
hospitalized
because
of an acute
myocardial
infarction,
and
23 were healthy
control
subjects.
All patients
with infarction
were studied
within
a few days after their acute episode
and
an average
of 12 weeks later (range,
1 to 35 weeks).
Control
subjects
were restudied
at an average
interval
of ten weeks
(range
1 to 32 weeks).
Heart sounds were recorded
during
quiet respiration
with
the patient
supine. The transducer
was placed at the second
left intercostal
space
and was held
in this position
by a
suction
cup. This permitted
a uniform
and repetitive
tech-
INTENSITY OF HEART SOUNDS AFTER MYOCARDIAL INFARCTION
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21043/ on 05/05/2017
679
mque
for the
application
of the transducer.
Ten consecutive
analyzed
to determine
an average
intensity
of the
heart sounds in each patient.
The frequency
response
of the
amplifier
(Electronics
for Medicine)
and microphone
(hex
Medical
Systems
Heart
Sound
Microphone
120-131)
have
been
previously
described.10
The intensity
of the heart
sounds was specified
in terms of the sound pressure
level of a
100-Hz
tone which
produced
the same peak-to-peak
voltage
measured
at the output
of the microphone-amplifier
system.
The method
of calibration
of the microphone-amplifier
system also has been described.i0
beats
The amplitude
of the heart
sounds
was measured
as the
peak-to-peak
deflection
of the acoustic
signal
and was expressed
in dynes/sq
cm. The intensity
of the heart
sounds
was calculated
by the following
equation:
intensity
of
sound = p2/pc,
where
p represents
pressure
(in dynes/sq
cm);
p represents
the density
of air (0.00120
gm/cu
cm),
and c represents
the velocity
of propagation
(34,400
cm!
sec).
The intensity
of sound was specified
in decibels
relative
to
a root mean square
sound pressure
of 0.0002
dynes/sq
cm.1’
The peak-to-peak
amplitude
of the heart sounds was measured in millivolts
and converted
to decibels
using a calibration curve based upon the peak-to-peak
voltage
produced
by
a 100-Hz
tone.
aortic
component
of the second
sound (A,) was
identified
as the first major
component
of S, and was observed
at the dicrotic
notch of the carotid pulse tracing.
The
P, was defined as the second
major component.
The
The period
of isovolumic
relaxation
in each
subject
was
determined
noninvasively
from
a simultaneously
measured
apexcardiogram
and phonocardiogram.
The apexcardiogram
was recorded
at a paper
speed
of 200 mm/sec
with
the
patient
on his left side. The sound that was recorded
during
the apexcardiogram
was used only for timing the duration
of
isovolumic
relaxation.
The period
of isovolumic
relaxation
was measured
as the time from the onset S, to the nadir
(0 point)
of the apexcardiogram.’
We also calculated
an
average
rate of isovolumic
relaxation
(in mm Hg/sec)
by
dividing
arterial
diastolic
pressure
by the period
of isovolumic
relaxation.
Systolic
time
intervals
were
measured
in all subjects
1-Clinieal
Data
Blood
pressure,
Heart
Data
rate,
Blood pressure
was measured
with a sphygmomanometer
just before
sound
was recorded.
Control
subjects
were
selected
from active
asymptomatic
working
men.
None
had
cardiac
murmurs.
All had
normal
electrocardiograms
and
hematocrit
readings
above
40 percent.
In each control
subject, the cardiothoracic
ratio measured
from chest roentgenograms
was
less than
50 percent.
At the time
of initial
measurements,
control
subjects
were matched
with patients
with infarction
in regard
to blood pressure,
heart rate, height,
weight,
hematocrit
reading,
and P-R interval
on the ECG
(Table
1). No significant
differences
were
observed
among
these
variables
(unpaired
t-test).
Patients
with
infarction
were older
(55 ± 2 years vs 30 ± 2 years)
(P <0.001).
Normal
from
mm Hg
beats
Subjects
122/78
Subjects
± 1/1
Patients
with
Infarction
118/77
± 3/2
per
minute
69±2
79±3
Height,
cm (in)
178±3(70±1)
173±3(68±1)
Weight,
kg (Ib)
75±2(165±4)
80±3(176±7)
P-Rinterval,
sec
yr
Sex
ratio,
M/F
Hematocrit
percent
tTables
ttP
0.15
±0.04
0.15 ±0.01
30±2**
Age,
<0.00
55±2*t
23/0
21/4
reading,
44 ± 1
43 ± 1
values are means
1 (unpaired
t-test).
±
SE
(unless
otherwise
stated).
female subjects were included
among the patients
with
infarction
whereas
none was included
among
the normal
subjects.
Three
patients
with infarction
had a grade 1/6 murmur;
two were
ejection
murmurs
heard
along
the left sternal
border, and one was a holosystolic
murmur
heard at the apex.
Four
Patients
with murmurs
of an intensity
of grade 2/6 or greater
were excluded.
The diagnosis
of an acute myocardial
infarction was based
upon
a typical
episode
of pain in the chest,
the development
of Q waves on the ECG, and an elevation
of
serum concentrations
of enzymes.
The locations
of the acute infarctions,
as determined
from
the ECG,
and the number
of patients
for each
were
as
follows:
inferior,
ten; inferoseptal,
three;
inferolateral,
two;
inferoposterior,
two; anteroseptal,
five; and anterior,
three.
Four of the patients
with infarction
had a third heart
sound
(S,)
at the time of the initial
measurements.
Nine patients
had rales.
(Only
one of the nine patients
with rales had an
S, gallop
rhythm).
During
initial
measurements
four
pa.
tients were receiving
therapy
with various
forms
of nitrates,
using
the methods
described
by Weissler
et ali4 and Lewis et al.15
Total electromechanical
systole
(Q-S,)
was measured
from
the onset
of the QRS complex
to the first high-frequency
vibrations
of S2. The left ventricular
ejection
time (LVET)
was measured
from
the beginning
of the upstroke
to the
trough
of the incisural
notch
on the carotid
arterial
pulse
tracing.
The left ventricular
preejection
period
(PEP)
was
derived
by
subtracting
the
LVET
from
total
electromechanical
systole. The ratio of PEP/LVET
was measured
directly
from the uncorrected
values for these two intervals.
Ten beats were analyzed.
680
Table
were
Table
2-Data
from
First
Measurement
Data
Intensity
of heart
ergs/sec/sq
Normal
Follow-Up
Measurement
sound,
cm
A,
P2
S1
Blood
pressure,
Heart
rate,
mm
beats
Hg
25±3
7±1
21±4
26±4
6±1
19±4
122/78±1/1
120/76±1/1
per
minute
PEP,
Subjects
msec
69±2
67±2
89 ± 2
87 ± 2
PEP/LVET
0.29 ±0.01
0.29
Period
of isovolumic
relaxation,
sec
0.11±0.002
0.11 ±0.002
Rate of isovolumic
relaxation,
mm
tTable
values
measurements
Hg/sec
are means
±
was 12 weeks.
STEIN, SABBAH, BARR
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21043/ on 05/05/2017
710 ± 15
SE.
Average
±0.01
724 ± 18
interval
between
CHEST, 75: 6, JUNE, 1979
ECG
ECG
-
SI
SOUND
SOUND
__h
_‘L
__-
I,:
COD
k
FIGuRE
patients
1
Iut
SEC
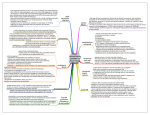
1. Heart sounds
recorded
in period
immediately
at second
left
after
infarction
intercostal
(left)
1
SEC
space and carotid
during
recovery
and
pulse
sound amplifier was same during both recordings.
Interval between
measurements
The S1, A,, and P, each showed prominent
increase
during
recovery.
two
ing
received
various
heart
sounds,
propranolol.
receiving
cardiac
14 patients
cardiac
glycosides,
glycosides,
six were receivmeasurement
of
nitrates,
six were
receiving
proprano-
and
the subsequent
were
receiving
and ten were
During
lol.
Heart
Sounds
the
the
from
During
infarction,
patients
Subjects
The
jects
intensity
of the
heart
sounds
in control
sub-
not change
significantly
(paired
t-test)
during
the 12-week
average
interval
between
measurements
(Table
2). The blood pressure,
heart rate,
PEP,
ratio
of PEP! LVET,
period
of isovolumic
relaxation,
and average
rate of isovolumic
relaxation
also did not change
significantly
during
the period
between
measurements
(Table
2).
did
Patients
with
Infarction
vs Normal
sounds
in the
comparison
(expressed
of Si, a 9dB
reduction
of P2 (Table
3). These
range of heart
sounds,
frequency
tectable
with normal
tions of the intensity
corded
in the absence
reduction
hearing.’2
of sound
of
an
of A,,
an
and
differences,
are ordinarily
Measurable
frequently
S3 gallop
48
-
U)
cm
to
11
±
2
36
-
24
-
0
w
z
0
U)
8dB
U)
a 7dB
in the
de-
UIL.
0
>-
I-.
reduc-
were
rhythm
12
U,
z
reor
I-
z
rales.
--
Prolongation
of PEP/ LVET,
volumic
relaxation
(Table
nificantly
mal
from
the acute
of A2 increased
in
C)
C)
w
U,
Subjects
constituted
reduction
course
of recovery
average
intensity
3 ± 1 ergs/sec/sq
Infarction
60
period
in decibels)
from
90
immediately
after infarcto nonnal
subjects,
showed
a
lower
amplitude
and lower
intensity
of the S1, A2,
and
P, (P < 0.001;
unpaired
t-test)
(Table
3 and
Fig 1 to 4). This
prominent
reduction
of heart
Patients
tion,
in
Recovery
Gain
of
16 weeks.
ergs/sec/sq
cm. Among
the 19 patients
who showed
an increase
of the amplitude
and intensity
of A2, the
ratio of PEP/LVET
improved
from 0.40 ± 0.01 to
0.35 ± 0.01 (P < 0.02),
the period
of isovolumic
RESULTS
Normal
during
from
tracing
(right).
was
of the PEP, an elevation
of the ratio
prolongation
of the period
of isorelaxation,
and a reduced
rate of isovolumic
accompanied
the reduced
heart
sounds
3). The blood
pressure
did not differ
sigbetween
patients
with
infarction
and nor-
subjects.
CHEST, 75: 6, JUNE, 1979
MI
NORMAL
SUBJECTS
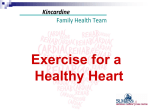
Ficuax
2. Intensity
of S1 recorded
at second
left intercostal
space
in patients
during
early
period
after
myocardial
infarction
(MI)
and in normal
subjects.
During
early
period
after infarction,
Si was lower than in normal
subjects
(P <
0.001).
INTENSITY OF HEARTSOUNDSAFTERMYOCARDIALINFARCTION
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21043/ on 05/05/2017
681
60
-
30
.
0
0
z
z
0
48
Cl)
-
24
Cl,
a
z
0
z
0
0
0
w
U)
0
Ui
C,,
a
U.
U-
0
_01
36
z
Ui0
z’OJ
.
0
S
2
a
18
00
U)
0.
0’
-
.
S
Ui
(I,
S
0
OW
I-
24
-
0
S
z
S
0
.
U-
0
S
a
>-
I-
12
Ui
I-
z
S
a
U
.
-
S
0.
S
z
-
-J
.
U)
S
12
0
S
6
>-
S
U)
z
-1-
S.
Ui
I-
S.-
z
5’
S
S.
MI
NORMAL
SUBJECTS
MI
NORMAL
SUBJECTS
3. Intensity
of A2 during
early period
after
myocardial
infarction
(MI)
and in normal
subjects.
In early period
after
infarction,
A2 was of lower intensity
than in normal
subjects
(P <0.001).
FIGuRE
±
second
0.003
period
±
from
diminished
relaxation
0.12
(P
of isovolumic
24
0.14
±
relaxation
second
0.01
and
0.001),
<
the
increased
Hg/sec
to 656 ± 30 mm Hg/sec
The P2 also increased
in these patients
ergs/sec/sq
cm
to 6 ± 3 ergs/secs/sq
mm
0.001).
±
0.2
(P
<0.05).
did
not
The
change
patients
blood
showed
intensity
of A,.
volumic
relaxation
pressure
of
these
during
significantly
a reduction
Among
or
no
sound
(P
<
from
change
the rate
in four
and
1
cm
of the
of iso-
DIscussIoN
of A, that
variations
study
are
investigations
produced
ample
readily
explained
relating
to
by the semilunar
evidence
to indicate
of
vibrations
the
closed
valves.7’18”7
These
vibrations
pressure
within
the blood
the
wall
changes
682
of the
in
pressure
chest,
were
on
the
basis
the cause
valves.767
that
the
and
detected
and,
consequently,
closure
across
leaflets;’7
and,
pressure
is produced
that
implies
audible
to
of the
can
be
rate
paired
isovolumic
be
lower
in
STEIN, SABBAH, ‘IARR
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21043/ on 05/05/2017
S2 is the
difference
in pressure
slowly
than in normal
the
we observed
that
the
of
intense
blood.7”7
of
rate
A2 in the
of isovolumic
in the early
rate
was
lower
study
shows
expected
to
of isovolumic
the
changes
lower
driving
closed
the
a less
within
The
rate
develops
across
the
after infarction,
isoTherefore,
following
consequently,
explains
study.
the pressure
gradient
valve.
Conversely,
this
of A,
reduced
vibration
more
slowly
developing
a slower
deflection
of
acoustic
infarction
produce
intensity
valvular
relaxation
factor
of the
of the aortic
valve,
the
the valve develops
more
sound
is now
of
characteristics
the
in this
as an acoustic
hemodynamic
at which
a pressure
gradient
valve after closure.5’7
In patients
volumic
relaxation
is impaired.5
several
by
primary
the
This mechanism
fluctuations
transmitted
as
determines
patients
pulmonary
vibrations
that
by a microphone
The
in this
S2 is produced
produce
which
are
are
of
of the
There
aortic
where
that
observed
signal.
subjects.5
This
force
results
in
increased
in two.
The
or transduced
pressure
528
patients
period.
Six
six,
these
decreased
this
to
average
from
4. Intensity
of P2 following
myocardial
infarction
(MI)
and in normal
subjects.
Intensity
of P2 in period
immediately
after infarction
was lower than in normal
subjects
(P <0.001).
FIGURE
period
after
development
across
that
of
the aortic
a reduction
be accompanied
by a
relaxatipn.
Since
im-
relaxation
has
been
patients
with
poor
found
ventricular
to
CHEST, 75: 6, JUNE, 1979
Table
3-Data
from
of heart
cm
Patients
with
Infarction
of heart
ergs/sec/sq
12±11*
6±1*1
10±1*1
21±4*1
intensity
of heart
valves,
dB
93±11*
85±1*1
81+11*
85±11*
122/78±1/1
118/77±3/2
88±1*1
pressure,
Heart
rate,
mmHg
beats
69 ± 2
89±2f
msec
PEP/LVET
Period
of isovolumic
relaxation,
sec
1Tables
values
<0.001
**
are
for
tP <0.05
Hg/sec
means
normal
subjects
with
vs patients
variations
with
changes
in the
ratio
of PEP/LVET
with
average
changes
in the intensity
this
association.
variations
of the
The
the
A,.8”6
gradient
ventricle
The
The
rate
between
is the
study,
that
the
affects
rate
the
isovolumic
relaxation
during
the course
It is now
recognized
as well
we
through
with
prominent
were
excluded.
patient
None
contractile
factors.”
variations
of
the
In
intensity
patients
obof the
we
of
the
period
to
pressure
CHEST, 75: 6, JUNE, 1979
2/6
had
infarction
and
with
have
shown
ventricular
observations,
another
the
fluid
intensity
(blood
since
patients
or
louder)
that
one
regurgitation.
cardiac
murmurs.
was
found
that
the
reduce
semilunar
valves
distend
would
of heart
of patients
would
to be the
diminish
of
sounds.’#{176} A more
with
the
viscosity
high
velocity
hematocrit
with
as they
which
vibrate
sounds.’#{176}”7 In
this
the
and
there-
study,
none
of the patients
or normal
subjects
was anemic;
the
hematocrit
readings
of both
groups
were
comparable.
Even
though
there
is strong
evidence
to suggest
that blood
pressure
is not the primary
hemodynamic
determinant
of the
otherwise
P,,
determined
readings)
The
ventricular
of the
suggest
aortic
S 1,28
mitral
subjects
recently
affects
viscous
infarction
several
right
P,
of pa-
and
nevertheless,
had
normal
with
have
blood
vari-
in pigs
of
infarction
of the
We
normal
blood
did
not
S,,s.6
of the
affect
the
sions,
with
and
been
observed
at
changes
generally
than
the
average
were
of
autopsy
were
age
exclude
infarction
subjects.
of sounds
among
Both
older
the
than
control
commissural
bases
of
valves
of elderly
subjects,
observed
in patients
of the
group
with
adhehave
such
older
infarction.29
INTENSITY OF HEART SOUNDS AFTER MYOCARDIAL INFARCTION
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21043/ on 05/05/2017
to
normal
groups
and
weight.
Patients
with
effusion
were
excluded.
calcification,
thickening
with
normal
matched
infarction.
infarction
Although
to
hypertensive.
transmission
also
with
in height
or pericardial
taken
were
patients
from
the chest
wall’
were
subjects
and patients
Patients
who
significantly
that
was
care
subjects
pressure
differ
Factors
of the right
venof recovery
from
that obstructive
of these
selection
(grade
In
factors
same.
performance
view
as many
stenosisZL2O
murmurs
(at
Since the P-R interval
is also thought
to relate to the
intensity
of S,,2 it was compared
in normal
subjects
subjects.
and inferoseptal
alterations
of
Such
sound
of sound.’
appropriate
aortic
rate
the
sounds.
of the
transmission
It is possible,
with
Studies
anteroseptal
significant
heart
to control
the
both
disease
were
similar
emphysema
ventricular
as the
attempted
Since
coronary
disease
can cause prominent
right ventricular
dysfunction.’8’#{176}
Abnormal
stiffening
of
the
right
ventricle
has been
observed
in such patients.’9
of right
intensity
98±3t
and
right
determinant
of right
intensity
of
actual
of
P2 that
of the
artery
intensity
intensity
P2 is analogous
pulmonary
hemodynamic
the
to the
to the
across
the
relaxation
of the
S, in
affects
in the early
of development
the
primary
of P,.8 Recognizing
isovolumic
relaxation
we infer
that
tricle
improved
the infarction.
cause
a diminished
mitral
concordant
of the
observed
suggest
that
isovolumic
right
ventricle
was also impaired
infarction.
this
fore
intensity
with
sug-
of a pro-
of A2 and
imply
average
served
after
valve),
infarction.
of A, indirectly
performance.
This
) .
intensity
infarction.
of
The
contractile
patients
dt
association
the
545±261*
ations
A, support
the
and
vs
dp/
observed
to
ventricular
affect
± SE.
subjects
for normal
performance,5
719±15*1
(maximal
the
to relate
of left
regurgitation27
0.14 ±0.004*1
0.11 ±0.002*1
shown
study
is
of S,
The
79 ± 3
Rate
of isovolumic
relaxation,
mm
relate
as possible
0.40±0.021*
0.29 ±0.01*1
been
of
infarction.
affect
factors
tients.
per minute
has
Clearly,
numerous
factors,
in addition
of development
of the pressure
gradients
4±11*
94±71*
observed
in this
Even
the mechanism
further
exploration.”4
of PEP/LVET
after
impairment
of development
for
ratio
functional
was
pressure
a basis
patients
1+0.3*1
7±11*
Si that
understood.
rate
isovolumic
5+11*
of
a subject
for
of Si in dogs
longed
P2
S,
detection
maximal
the
sound,
25±3*1
Blood
ventricle.
right
gests
A,
sound,
A2
P,
S1
for
the
remains
intensity
cm
Relative
method
The reduced
incompletely
sound,
29+2*1
15±11*
26±21*
Intensity
PEP,
Subjects
Normal
Subjects
Data
Amplitude
dynes/sq
A2
P,
S,
All
683
The
increase
recovery
of intensity
in many
initial
of the
difference
infarction
alone.
that
patients
observed
and
normal
Obviously,
one
can
heart
of A, that
affect
subjects
of heart
Regarding
that
we
the
absolute
We
measured
signal
method
sity
to
We
at
transmission
sounds
heart
the
level
of
the
intensity
of
varia-
following
myo-
of the
sounds,
chest
sonic
the
wall
energy
of the
the
shown
wall
consistent
of heart
at this
do
not
imply
the
valve.
the
intensity
affect
variations
contractile
of
as at the
study
apex.
shows
following
occur
with
heart
the
in the
a third
in
the
sounds
can serve
functional
as a clinical
state
guide
to the
are
other
HN:
Accentuation
an
sounds
a
factors
and
audible
properly
evaluation
of heart sounds in
J Physiol Heart
Am
Princeton,
NJ, D Van
Nostrand
Co, 1957, pp 9, 15
Yost WA, Nielsen
DW:
Fundamentals
of Hearing.
New
York, Holt, Rinehart
and Winston,
1977, pp 19, 136-137
D’Angelo
R, Shah N, Rubler
S: Diastolic
time intervals
in
ischemic
and hypertensive
heart disease:
A comparison
of
isovolumic
relaxation
time
and rapid
filling
time
with
systolic time intervals.
Chest 68:58-81,
1975
Weissler
AM, Harris
WS, Schoenfeld
CD: Bedside
technics for the evaluation
of ventricular
function
in man. Am
J Cardiol
23:577-583,
1969
Lewis
RP, Rittgers
SE, Forester
WF,
et al: A critical
review
of the systolic
time intervals.
Circulation
58:146158, 1977
Sabbah
HN, Stein
PD: Investigation
of the theory
and
mechanism
of the origin of the second
heart sound.
Circ
Res 39:874-882,
1976
Sabbah
HN, Stein PD: Relation
of the second
sound
to
diastolic
vibration
of the closed aortic valve. Am J Physiol
Heart Circ Physiol
3: H696-H700,
1978
18 Ferlinz
J, Gorlin
B, Cohn
PF, et al: Right
ventricular
performance
in patients
with
coronary
artery
disease.
reflect
relaxation
of the
of the heart.
ACKNOWLEDGMENT:
We
thank
Donald
Ph.D.,
and
Robert
Turner,
Ph.D.,
for their
calibration
of the heart sounds.
W. Nielsen,
assistance
in
REFERENCES
1 Price WH,
Brown
AE: Alterations
in intensity
of heart
sounds
after myocardial
infarction.
Br Heart
J 30:835839, 1968
2 Fowler
NO:
Cardiac
Diagnosis
of Heart
Disease.
New
York, Macmillan
Publishing
Co, mc, 1982, pp 32, 33, 40
3 Friedberg
CK:
Disease
of the Heart
(3rd
ed).
Philadelphia,
WB Saunders
Co, 1986, p 807
4 Stein PD, Sabbah
HN: Origin
of the second
heart sound:
Clinical
relevance
of new
observations.
Am J Cardiol
41:108-110,
1978
5 Stein PD, Sabbah
HN, K.haja F, et al: Exploration
of the
cause of the low intensity
aortic component
of the second
sound
in nonhypotensive
patients
with poor ventricular
performance.
Circulation
57:590-593,
1978
6 Kusukawa
R, Bruce
DW,
Sakamoto
T, et al: Hemodynamic
determinants
of the amplitude
of the second
heart sound.
J Appl Physiol
21:938-946,
1968
7 Blick EF, Sabbah
HN, Stein PD: One-dimensional
model
of diastolic
semilunar
valve vibrations
productive
of heart
684
Sabbah
17
rales
or
Reduced
transmission
of heart
15
16
intensity
Reduction
Consequently,
intensity
to be
infarction
of
isovolumic
performance.
of the
the
wall.
absence
14
necessarily
absence
of
heart
sound.
or their
ventricular
reduction
chest
over
a
inten-
intercostal
not
myocardial
at
13
The
23 normal
left
that
12
pressure
chest.
of intensity
although
sound
of
second
location,
reduced
of sounds
can
gallop
rhythm
PD,
An effect of blood
viscosity.
Circ Physiol 235:H664-H669,
1978
11 Olson HF: Acoustical
Engineering.
am-
at
in the
measurements
this
sounds
measurably
at the
the
same intensity
In conclusion,
10 Stein
sounds
acoustic
of
to be consistent
measured
found
age
factors
auscultatory
of quantitation
of
reached
of Si was
that
due
who
showed
no significant
change
of several
weeks.
The amplitude
and
space.
the
it
was
subjects
period
method
intensity
measured
as
not
sounds.
J Biomechanics
12:223-227,
1979
8 Stein PD, Sabbah
HN, Anbe
DT, et al: Hemodynamic
and anatomic
factors
which
participate
in relative
differences of the amplitude
of the aortic
and pulmonary
components
of the second heart sound. Am J Cardiol
42:539-544,
1978
9 Sakainoto
T, Kusukawa
B, MacCanon
DM, et al: Hemodynamic
determinants
of the amplitude
of the first heart
sound. Circ Res 16:45-57,
1965
anemia:
the
and
the
with
all of the
and
tions of the intensity
cardial
infarction.
plitude
was
intensity
interpreting
that
patients
evaluate
when
during
indicates
between
must
the
sounds
occurred
Circulation
52:608-615,
1975
19 Wells
DE, Befeler
B: Dysfunction
of the right ventricle
in coronary
artery disease.
Chest 66:230-235,
1974
20 Al-Sadir
J, Falicov
R, Zahavi
I, et al: Right
ventricular
dysfunction
in acute
inferior
myocardial
infarction
(abstract).
Circulation
47 (suppl
4) :59, 1973
21 Brooks
H, Holland
R, Al-Sadir
J: Right ventricular
performance
during
ischemia:
An anatomic
and hemodynamic
analysis.
Am J Physiol
Heart
Circ Physiol
2:H505H513,
1977
22 Rushrner
RF: Cardiovascular
Dynamics
(3rd ed). Philadelphia,
WB Saunders
Co, 1970, p 305
23 van Bogaert
A: New concept
on the mechanism
of the
first heart sound.
Am J Cardiol
18:253-262,
1966
24 Craig
E: On the genesis
of heart
sounds:
Contributions
made
by echocardiographic
studies.
Circulation
53:207209, 1976
25 Sabbah
HN, Khaja
F, Anbe DT, et al: Determinants
of
the amplitude
of the aortic component
of the second
heart
sound in aortic stenosis.
Am J Cardiol 41:830-835,
1978
26 Luisada
AA:
The
second
heart
sound
in normal
and
abnormal
conditions.
Am J Cardiol
28:150-161,
1971
27 Sabbah
HN, Khaja F, Anbe DT, et al: The aortic closure
sound in pure aortic insuciency.
Circulation
58:859-862,
1977
28
29
Leatham
A: The first and second
heart
sounds.
In Hurst
JW, Logue
RB, Schlant
RC, et al (eds):
The Heart,
Arteries
and Veins
(4th
ed),
New
York,
McGraw-Hill
Book Co, 1978, pp 237-244
Pomerance
A: Aging
changes
in human
heart valves.
Br
Heart J 29:222-231,
1987
STEIN, SABBAH, BARR
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21043/ on 05/05/2017
CHEST, 75: 6, JUNE, 1979