Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
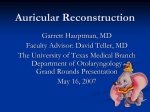
CME Upper Extremity Microsurgery William C. Pederson, M.D. San Antonio, Texas Learning Objectives: After studying this article, the participant should be able to: 1. Understand the indications for free flap coverage of the upper extremity. 2. Know the advantages and disadvantages of the flaps discussed. 3. Have a basic understanding of the anatomy of the flaps discussed. 4. Have a variety of options for free tissue transfer. The application of microsurgical tissue transfer to reconstruction of the upper extremity allows repair of significant bone and soft-tissue defects. Through the years the approach has changed from one of simply getting the wound covered to primary reconstruction to preserve or regain function. A wide variety of free flaps offers the potential to reconstruct nearly any defect of the arm and hand. Vascularized bone transfer can be utilized to repair large bony defects, while innervated free muscle transfer can replace missing muscle function. The total array of flaps and their indications is beyond the scope of a single discussion, but this article focuses on a few flaps that have found application for coverage and functional restoration in the hand and upper extremity. (Plast. Reconstr. Surg. 107: 1524, 2001.) will discuss options for the reconstruction of the upper extremity with free tissue transfers.5,6 APPROACH The topic of upper extremity microsurgery is a wide one, and for the purposes of this discussion, it will be divided into two areas: coverage and functional reconstruction. Although many situations will be encountered in which softtissue coverage is the only requirement, it should not be forgotten that coverage and functional reconstruction can be accomplished in one step with the appropriate application of microsurgical tissue transfer. In assessing a wound of the upper extremity, the surgeon should first decide on the ultimate goal of the reconstruction. This will be predicated on many factors, not the least being the patient’s age, occupation, other injuries, and future plans. The surgeon should have in mind a plan in terms of how the initial procedure fits with what else may be necessary in the future. Although soft-tissue coverage may be the first priority in a patient with an avulsion injury to the hand, the type of flap chosen not only should allow later surgery but should be performed in a way that will maximize later efforts. When a patient initially presents with a wound of the upper extremity, the surgeon must carefully assess the wound and make a number of important decisions. The assessment of the injury should take into account the status of the wound (clean or dirty), the presence or absence of fractures (and/or bony defects), and the status of neurovascular struc- Since its inception, microsurgery has found wide application in reconstructing the upper extremity. Digital replantation, which was first performed in 1968,1 probably represents the pinnacle of reconstruction in the hand, because it allows exact replacement of the missing part. The replacement of missing parts in kind was extrapolated in 1969, when Cobbett2 reported the first great toe transfer to replace a missing thumb. Although the first successful free flap reported in 19733 was to the lower limb, the technique of free tissue transfer rapidly became incorporated into reconstructive surgery of the hand and arm. Through the study of vascular anatomy of potential donor sites, the plastic surgical community has given itself a wide variety of available tissues for reconstructive purposes.4 Almost any composite defect of the upper limb can now be reconstructed with a free tissue transfer. This article From the Hand Center of San Antonio and the Departments of Surgery and Orthopaedic Surgery, the University of Texas Health Science Center at San Antonio. Received for publication April 20, 2000; revised August 25, 2000. 1524 Vol. 107, No. 6 / 1525 UPPER EXTREMITY MICROSURGERY tures (distal vascular supply and nerve function). All of these considerations are important in choosing the proper approach to reconstruction. Clean wounds with defects in structures other than soft-tissue coverage should be considered for primary reconstruction. Untidy wounds will usually require debridement and, although they may require free flap soft-tissue reconstruction, repair of other structures may best be left until a closed wound is obtained. PLANNING Regardless of the type of flap chosen, preoperative planning is essential for success. The primary issue in microvascular tissue transfer is vascular access for vessel anastomosis. Although the upper extremity has a rich vascular supply, trauma or tumor extirpation may limit the available choices for anastomosis. In most patients, the hand will maintain adequate perfusion if only one of the major arteries (radial or ulnar) is open. If the hand is viable and either one of these pulses is strong, I think that arteriography is unnecessary. If there is any question regarding the status of hand perfusion, an arteriogram should be performed, especially if free flap transfer is contemplated. In choosing where to perform vascular anastomoses, a site out of the zone of injury should be chosen. If one is not sure, the vessels should be explored and followed proximally until there is no blood staining in the vascular sheath. For coverage of the hand, anastomosis is usually performed to either the radial or ulnar arteries. For the radial side of the hand and dorsum, the radial artery in the snuffbox may be used for end-to-end or end-to-side anastomosis. If both the radial and ulnar arteries are patent, an end-to-end anastomosis at this level should not compromise circulation to the hand. In most instances, however, it is probably safer to perform an end-to-side anastomosis. For coverage of the forearm, anastomosis can be performed to either of these vessels or to the brachial artery in the antecubital fossa. If there is significant trauma to the forearm, a proximal end-to-side anastomosis to the brachial artery is preferable. In the upper arm, most anastomoses will be to the brachial system. Venous anastomosis is usually best done to one of the superficial veins of the forearm, because the deep venous system is small and anastomosis may be difficult. The surgeon must be sure that there is no proximal injury to the chosen vein to avoid outflow obstruction and thrombosis. For most free flaps, a two-team approach is the most expeditious. The recipient site can be debrided and vessels made ready for anastomosis while the flap is dissected. This may not be feasible in some settings, especially if the chosen flap is to come from the injured arm (i.e., the lateral arm flap). If there is inadequate surgical help for this approach, the wound is debrided and measured, and then an appropriate flap is harvested. Once the flap has been harvested, it is left attached by its pedicle for perfusion while the vessels are dissected on the recipient limb. When the recipient vessels are ready, the pedicle is divided and the flap is transferred. COVERAGE The approach to wounds of the upper extremity should follow the usual parameters of soft-tissue reconstruction. Many wounds can be covered with a split-thickness skin graft or with regional flaps, particularly in the hand. The ultimate morbidity of any local or regional flap must be considered, however, especially in relation to later hand function. Because the hand is highly visible, the cosmetic aspect of certain local and regional flaps must be considered as well. Although certain wounds may be adequately covered with a flap from the same extremity, one should consider what offers the best coverage in terms of the overall reconstruction.7 This will often lead to the use of a free flap for many hand wounds. The following discussion will cover the considerations regarding which flaps may be used for soft-tissue reconstruction in the hand and arm. The wound must be considered both in terms of its tidiness and size. The first step before flap coverage is always conversion of a grossly untidy wound to a clean one. Debridement should not be compromised to avoid making the wound larger, because almost any wound in the upper extremity can be covered with free tissue transfer. This concept was promoted by Godina, who coined the term “necrectomy”8 to describe the removal of all nonviable and contaminated tissue. In this approach, intact neurovascular structures are left in place and large bony fragments may be cleaned and replaced in their anatomic position if adequate coverage can be obtained. Once the wound has been debrided, flap selection should be considered. Dirty wounds are 1526 usually best covered with muscle, because muscle manages infection better than skin only.8,9 Vascularized fascia also has advantages in terms of potential contamination,10 and it may be considered in some untidy wounds. The selection of flap coverage for a clean wound allows the use of composite tissue in many cases. Particularly in the case of tumor extirpation, the reconstructive surgeon may have the option of reconstructing a complex defect with a single flap. Although many smaller wounds in the upper extremity are amenable to local or regional flaps (i.e., the pedicled groin flap), this discussion will center on the use of free flaps for wound management. Muscle Flaps for Coverage The selection of which muscle to transfer is based largely on the experience of the surgeon, but the “workhorses” in large wounds of the upper extremity are the latissimus dorsi and rectus abdominis muscles. Smaller defects can be covered with either a portion of one of these muscles or a smaller muscle flap, such as the serratus anterior or gracilis muscle. Latissimus dorsi. The latissimus dorsi muscle is a large muscle of the back and shoulder, and its vascular supply for free transfer is based on the subscapular-thoracodorsal system.11,12 The pedicle is lengthy (8 to 11 cm) and has a relatively large diameter proximally (up to 6 mm). This is the largest single muscle available for transfer, and its area of coverage can be expanded by including a portion of the serratus anterior muscle through its branch off the thoracodorsal artery.13 It can be used as an innervated muscle because of the single thoracodorsal nerve,14 but the latissimus is generally used to cover large, degloving-type wounds. Its advantages are that it has a totally reliable vascular supply and is very large. Its primary disadvantage is that the patient must be turned in the lateral decubitus position for muscle harvest. If the contralateral muscle is taken, the patient can be turned on the side, and the injured arm can be prepared simultaneously with muscle harvest (assuming that appropriate surgical assistance is available). It can be taken as a myocutaneous flap, but for most indications in the upper extremity, only the muscle is taken; it is then covered with a split-thickness skin graft. The donor site is easily closed, but seroma formation is a common sequelae of this donor site. The functional morbidity from the loss of muscle is minimal in most patients, but its use should be avoided PLASTIC AND RECONSTRUCTIVE SURGERY, May 2001 in patients who must adduct the arm strongly (crutch-walkers and paraplegics). Rectus abdominis. The rectus abdominis is a muscle widely used in microsurgery, primarily as part of the TRAM (transverse rectus abdominis musculocutaneous) flap for breast reconstruction. This muscle is on the anterior abdominal wall and runs from the medial lower ribs to the pubis. It lies in a sheath composed anteriorly of continuations of the external and internal oblique muscle layers. The posterior sheath is a continuation of the transversus abdominis, but in the lower abdomen, it is quite thin (below the linea semicircularis). This is a fairly large muscle, and it has a reliable vascular pedicle based on the deep inferior epigastric system. The pedicle is fairly long (5 to 7 cm), and its diameter is fairly large (2.5 to 3 mm). The rectus abdominis muscle will cover most defects of the hand and forearm,15,16 and it will cover large defects of the forearm if most of the muscle is harvested and it is placed “barber pole” fashion around the arm.17 The advantages of this muscle are that it has a reliable vascular pedicle and may be taken with the patient supine. The disadvantage of this muscle is that a hernia can result from its harvest if fascia is taken (for a myocutaneous flap) or if the anterior sheath is weak. For coverage of the upper extremity, this muscle is usually harvested without a skin paddle and covered with a split-thickness skin graft. Serratus anterior. This muscle is very useful for covering smaller hand defects.13,18 It consists of nine slips of muscle that connect from the ribs at the anterior axillary line to the tip of the scapula. The lower slips are vascularized by a branch coming off the thoracodorsal artery, and the upper slips are vascularized by a branch of the lateral thoracic artery. The lower three slips may be taken individually or together as a free muscle flap based on the thoracodorsal pedicle. This dissection is tedious because branches of the long thoracic nerve may be intertwined with the vessels, and damage to the nerve supplying the remaining slips of muscle can lead to winging the scapula.19 The branch to the serratus is usually taken with the proximal thoracodorsal vessels, both to lengthen the pedicle and because of the larger diameter of the proximal vessel. This can give a very lengthy pedicle (15 to 17 cm) with a large diameter (3 to 6 mm). The primary advantage of this muscle is its small size and lengthy vascular pedicle. The disadvantages of this muscle are the potential Vol. 107, No. 6 / UPPER EXTREMITY MICROSURGERY for long thoracic nerve injury and the decubitus position necessary for harvest. This flap can be used to cover the dorsal or palmar hand and first webspace. It has the potential for innervation with a branch of the long thoracic nerve, but this application would be limited in the upper extremity. Although there are certainly other muscles available for use in the upper extremity, these three will afford coverage for almost any wound. The gracilis muscle will be discussed below in the section on functional reconstruction. Fascia and Fasciocutaneous Flaps In the case of clean traumatic wounds or tumor excision, a cutaneous free flap may offer the best option for reconstruction. These flaps usually offer a better cosmetic result than a muscle covered with a skin graft, and they are probably better in terms of performing later surgery through or under the flap. This is particularly true in the case of later tendon surgery, where the fascia contained in these flaps may offer a better gliding surface for tendons. In a hand with multiple digital amputations, a cutaneous flap is better in terms of providing coverage for later toe transfer as well. There are any number of fascial/ fasciocutaneous flaps available, but the primary flaps are the radial forearm, lateral arm, scapular, and temporoparietal fascial free flaps. Although the groin flap is used in some centers as a free flap and has some definite advantages (primarily donor-site cosmetics), the variability and limited length/size of its vascular pedicle make it a second level choice for free transfer in most centers. Radial forearm free flap. This flap offers almost ideal characteristics for hand reconstruction.20 Its primary application is as a pedicled flap based on reversed flow through the distal radial artery and venae comitantes.21 Nonetheless, it may be used as a free flap in certain instances, and it affords excellent hand coverage. This flap can be raised anywhere along the course of the radial artery, and a skin island from very small to quite large may be taken. The radial artery provides a large caliber vessel for anastomosis, and it may be used for revascularization of the distal limb if necessary as a “flowthrough” free flap. The venous drainage is through the dual concomitant veins of the radial artery, but larger flaps can be drained using cutaneous veins. There has been some controversy regarding the primary venous drainage of these flaps, but the venae comitantes offer reliable drainage, even in the absence of super- 1527 ficial veins. This flap may be innervated by anastomosis of the lateral antebrachial cutaneous nerve, part of which is invariably in the flap. The quality of sensation in such reinnervated flaps is not great, but it may be useful. If the patient has a palmaris longus tendon, it may be taken in the flap as well, and this provides an excellent option for tendon reconstruction, especially on the dorsal hand. Because the tendon is taken with its surrounding tissue, it has excellent gliding when transferred as part of the flap. A portion of the volar radius may be harvested with the flap as well, and this is particularly useful in the reconstruction of missing segments of metacarpal.22,23 The radial artery can be taken with the fascia only; this provides a thin flap that is particularly useful in reconstructing the palm. The advantages of using this flap as a free flap are its thinness, its reliability (based on the radial artery), and the multitude of other tissues that may be harvested with it. The main disadvantage of this flap is the resulting donor site, which must usually be covered with a skin graft. The donor site is usually aesthetically unpleasant, but it causes few functional problems. Another relative contraindication to this flap is the loss of the radial artery, but studies have shown that significant problems are unusual. Cold sensitivity is seen, but this may be related to other factors. Although the radial forearm flap is an excellent free flap, it can usually be used as a distally pedicled island flap for hand reconstruction. If this flap is not available for some reason as a pedicled flap, I usually select a skin flap from another area and do not take a radial forearm flap from the contralateral uninjured arm. Lateral arm free flap. This cutaneous flap from the lateral distal upper arm is based on the radial collateral artery, a branch of the profundus brachii.24 This vessel runs with the radial nerve in the spiral groove and comes to lie in the intermuscular septum between the brachialis and lateral head of the triceps. It gives arterial supply to the skin overlying the septum and to the underlying humerus. Distal to the intermuscular septum, the posterior radial collateral artery has a rich system of anastomoses with vessels in the proximal lateral forearm, which will allow extension of the flap onto the proximal forearm. The pedicle for this flap is relatively short (5 to 7 cm), and the proximal artery has a small diameter (1.5 to 2 mm) when compared with the flaps previously discussed. The length of the pedicle is limited by the fact that it exits the spiral groove with the radial nerve, and dam- 1528 age to this nerve must be avoided in dissection. The skin paddle can be based directly over the intermuscular septum for a smaller flap or extended distally for a larger one. Donor sites up to 7 cm in width can be closed primarily, but larger ones will require a skin graft.25 When closed primarily, the donor site can be very cosmetic, but in some patients, the scar will widen significantly. The lateral cutaneous nerve of the arm is in the flap, and thus the skin can be innervated if necessary.26 A portion of the lateral humerus can be taken with the flap for bony reconstruction, based on its vascular supply from the overlying pedicle.27 The lateral arm flap is purported to be a “thin” flap, but because of the tissue in the intermuscular septum, it is a bit bulky when placed on a flat recipient site (i.e., the back of the hand). This problem can be avoided by using the fascia only, which also decreases donor-site problems.25,28 The primary advantages of this flap are that it can be taken from the ipsilateral arm (of injury),29 it avoids the sacrifice of a major vessel, and the donor site can often be closed primarily. The primary disadvantages of the lateral arm flap are its somewhat limited size and the short and smalldiameter pedicle. It is very useful in covering small defects of the hand and works very well in the first webspace. In thin patients, it can be used to cover a degloving injury of the thumb, with the added benefit of reinnervation by the cutaneous nerve (Fig. 1). Scapular flap. The scapular and parascapular flaps offer a versatile large skin flap to cover defects in the upper extremity (Fig. 2).30 The vascular supply is based on the circumflex scapular vessels, which branch from the subscapular system.31 The pedicle for this flap is long (4 to 6 cm) because the subscapular vessels can be taken if necessary, and this provides vessels of large diameter at the takeoff from the axillary artery. The vessels lie in the fascia with branches to the overlying skin. There are two primary branches, thus giving rise to the “transverse” scapular flap, which is sited transversely across the back, and the “parascapular” flap, which is sited obliquely down the back. Based on this vascular supply, a very large skin flap can be designed that will cover most defects of the forearm and/or arm.32 Although a number of cutaneous nerves enter the skin, there is not a dominant nerve to this area, and thus this flap has poor potential for in- PLASTIC AND RECONSTRUCTIVE SURGERY, May 2001 nervation. Branches from the primary pedicle feed the lateral surface of the scapula, and a portion of this bone can be taken to repair bony defects. This bone is quite flat, however, and its primary indication is in the reconstruction of smaller defects in the hand. Donor sites in the 8-cm range can usually be closed primarily, but this is usually limited to the parascapular design of the flap. The primary advantages of this flap are the length and diameter of its pedicle, along with its potential large size. The primary disadvantage of this flap is the need for turning the patient to harvest it. The scapular flap is an excellent choice to cover large wounds of the forearm, and it can be used in place of a pedicled groin flap for hand coverage. It can be combined with the latissimus dorsi and serratus anterior muscle flaps on a single pedicle to provide a huge amount of tissue and to cover different surfaces of the hand and arm (Fig. 3).33,34 Temporoparietal fascia flap. The temporoparietal fascia offers a flap of specialized tissue that has great utility in hand reconstruction.35 This flap is supplied by the superficial temporal artery and vein, and it has a pedicle in the 2- to 3-cm range that is about 1.5 to 2.5 mm in diameter.36 The temporal fascia lies on the temporal region of the skull, beginning on the zygoma and running superiorly. There is a superficial and deep layer, and both may be taken with this flap. The use of both layers of fascia has been promoted for use in wrapping adherent tendons on the dorsum of the hand after tenolysis in a scarred bed. The deep fascia can also provide tissue for reconstructing small tendons on the dorsal hand as well. A flap of moderate dimensions may be taken (in the range of 8 to 10 cm). The potential for harvesting vascularized bone with this flap exists, but the thin, outer table bone available has few (or no) indications in the hand. Although the donor scar is one of the best in terms of cosmesis, the problem of alopecia exists because the superficial fascia must be dissected from just beneath the hair follicles of the scalp. The primary advantages of this flap are its potential to provide a gliding surface and its good donor site (one of the best in terms of cosmesis). The primary disadvantage of this flap is that it is very thin and must be covered with a skin graft. Temporoparietal fascia offers very nice coverage for defects of the fingers and hand, but the size of the flap is limited.37 Vol. 107, No. 6 / 1529 UPPER EXTREMITY MICROSURGERY FIG. 1. (Above, left) Degloving injury to the thumb in a 23-year-old man. (Above, right) A piece of cloth is used for a template for a lateral arm flap. (Center, left) The flap is marked on the lateral upper arm. (Center, right) The flap is placed. Note that the “seam” was placed dorsally, with anastomosis of the lateral cutaneous nerve of the arm to the ulnar digital nerve of the thumb. (Below, left) Results at 8 months. Protective sensation had returned. (Below, right) Flexion at 8 months. This tissue does seem to improve the gliding ability of tendons, particularly on the dorsum. When covered with a split-thickness skin graft, the temporoparietal fascia flap offers the thinnest coverage available (excluding other fascial flaps). It is probably not the best choice when later surgery through the flap is contemplated, however. FUNCTIONAL RECONSTRUCTION Composite tissue transfer offers the ability to reconstruct functional deficits with flaps containing skin, bone, joint, and reinnervated muscle. Detailed discussion of each of these areas is beyond the scope of this article, but a brief outline of procedures to deal with signif- 1530 FIG. 2. (Above) The hand of a baby with dorsal wrist contracture after a burn. (Below) The hand after scar excision, wrist release, and scapular flap. FIG. 3. Multiple flaps are available on single pedicle. Here a portion of serratus anterior, latissimus dorsi, and a scapular cutaneous flap have been harvested on a single subscapular pedicle. icant bone loss, muscle necrosis, and digital loss will be covered. Free Fibula Most bony defects in the upper extremity can be managed with standard bone grafts; however, long defects (⬎ 6 cm) and those PLASTIC AND RECONSTRUCTIVE SURGERY, May 2001 associated with recurrent failure to heal may be candidates for microvascular bone transfer.38 Although there are several flaps available that can include a portion of vascularized bone (iliac crest, lateral arm, radial forearm, dorsalis pedis), the fibula osseocutaneous flap offers the best piece of bone for reconstructing significant defects of the long bones of the upper extremity.39,40 Smaller defects, such as those in the hand, can be managed by one of the previously discussed flaps, with inclusion of a segment of bone. Larger defects of the radius, ulna, or humerus will usually require a piece of bone such as the fibula.41 The vascular supply of the free fibula is based on the peroneal vessels of the leg. These vessels run along the deep surface of the fibula from just below the tibioperoneal trunk to the level of the ankle. Although the peroneal vessels provide a nutrient artery to the medullary canal of the fibula, they also provide a rich periosteal blood supply to the cortical surface. The proximal portion of the fibula can be taken to reconstruct the radiocarpal joint, but this segment of bone gets its primary blood supply from a branch of the anterior tibial artery,42 which must be taken to assure viability of this segment. A portion of the skin overlying the fibula can be taken with the bone, and thus compound defects can be managed with this flap (Figs. 4 and 5). The perforators to the skin run around the posterior aspect of the bone, and thus it is best to include a cuff of muscle along the posterior surface of the bone if a skin paddle is to be included. If a skin paddle is taken, most donor sites will require a skin graft on the overlying muscles. The primary advantage of this donor site is the large amount of bone that can be taken. In adults, a total of up to 24 to 26 cm of bone may be harvested. The fibular head should be left in place at the knee level, and 6 cm of the distal fibula should remain to avoid problems with the ankle. In children, a screw should be placed across the fibular-tibial joint to avoid proximal migration of the fibula. The disadvantages of this donor site are few: the pedicle is relatively short (2 to 4 cm) and there is some morbidity from harvesting, but these do not usually present functional problems. Innervated Gracilis Transfer In some instances, there is a need to replace damaged or excised muscle in the forearm or upper arm. Although many losses can be adequately reconstructed with standard tendon Vol. 107, No. 6 / 1531 UPPER EXTREMITY MICROSURGERY FIG. 4. (Above, left) Humeral nonunion in a patient who had undergone seven prior procedures to attempt union. (Above, right) Intraoperative x-ray. Note that the fibula is held in place with only two screws, while the plate spans the defect at the site of resection of nonunion. (Below) Arm after vascularized fibular transfer to nonunion. Hemostat points to plate over fibula. transfers, patients with significant loss of muscle substance (such as those with Volkmann’s ischemic contracture) may benefit from reconstruction of function with a microvascular muscle transfer (Fig. 6).43 The muscles available for this include the gracilis, latissimus dorsi, and rectus femoris. This latissimus dorsi can be used in the forearm as a free functional transfer,44 but it is not ideal. The rectus femoris has been used for this in the past, but again it is not the optimal muscle. The gracilis muscle, however, is nearly ideal for reconstruction of the muscles of the forearm. It has adequate excursion to provide finger flexion or extension, it is of the appropriate size (both length and width), and it has an excellent neurovascular pedicle. The gracilis is a muscle in the medial thigh that runs from the pubis to the medial tibia. It has a primary vascular pedicle (a branch of the profundus femoris) and enters the muscle at its undersurface about 6 to 12 cm below its origin. The pedicle is rather short (5 to 6 cm) and of relatively small diameter (1 to 2 mm). There are usually two or three secondary pedicles that enter the muscle distally, but the muscle is well-perfused by its primary pedicle alone after microvascular transfer. The gracilis is powered by a single nerve, the anterior 1532 FIG. 5. Results from the patient shown in Figure 4 at 2 years postoperatively. Note incorporation and hypertrophy of the fibula. branch of the obturator nerve, which enters the muscle at the level of the vascular pedicle proximally. The distal third of the muscle is tendinous, and this tendon is ideal for attachment to the distal flexors or extensors of the digits. The primary advantage of this muscle as an innervated free transfer is that its size and excursion closely match those of the muscles of the forearm. The primary disadvantage of this muscle for free transfers is its relatively short and small pedicle. The primary indication for innervated muscle transfer to the forearm is loss of muscle mass, as in Volkmann’s ischemic contracture or traumatic avulsion of the muscles. The prerequisites for successful innervated muscle transfer include adequate passive excursion of the distal joints, intact sensation in the hand, available neurovascular structures for anastomosis, adequate distal soft-tissue for coverage of the tendon repairs, and lack of a simpler solution for the problem.43 In certain instances, some of these requirements can be modified if the others are present. In general, however, this procedure should be reserved for those patients with a severe problem that is not amenable to more standard solutions. Toe Transfer Microvascular toe transfer represents one of the pinnacles of reconstructive surgery. The PLASTIC AND RECONSTRUCTIVE SURGERY, May 2001 ability to replace in kind a missing digit with a mobile, sensate toe offers the best type of reconstruction available. Although this is a complex microsurgical procedure that should not be undertaken without experience,45 it remains the benchmark for thumb and most digital reconstructions. There are a number of variations of toe transfer, and almost any tissue needed for digital reconstruction can be transferred. These range from pulp-only transfers to double second and third toe transfers to reconstruct the metacarpal hand. Because this is an overview, the discussion here will be limited to anatomy and a few technical points. All great and second toe transfers ideally have their vascular basis on the dorsalis pedis– first dorsal metatarsal system. This anatomy is highly variable, however, and a thorough knowledge of it is the basis for safe harvesting of these flaps. The venous drainage is based on the dorsal superficial veins of the foot, because the deep system that accompanies the arterial supply is usually very small. The flaps can be innervated by the proper plantar digital nerves to the toe(s) and by the deep peroneal nerve, which accompanies the dorsalis pedis/dorsal metatarsal vessels. Joint reconstruction. Destruction of the proximal interphalangeal or metacarpophalangeal joint in a finger remains a formidable reconstructive problem. Although arthroplasty with artificial joints continues to be an option in these patients, results are poor in young, active patients. The possibility of reconstructing a missing finger joint with a joint from a toe would seemingly obviate the problems associated with artificial joint replacement. There have been a number of reports of joint replacement in the hand with toe joints.46 –50 The metatarsophalangeal joint and proximal interphalangeal joints of the second toe are used most often to reconstruct the analogous joints in the hand. Despite early enthusiasm for this procedure, it remains problematic. Extensor lag at the transferred joint is common,49 –52 and complication rates are fairly high and include vascular failure, infection, and late joint destruction.50,52 Active range of motion for transferred metatarsophalangeal joints is in the 30-degree range, with less in transferred interphalangeal joints.50 –52 In children, transferred toe joints provide some potential for growth, but reports vary on the amount of growth obtained from the transferred epiphyses.52–54 Although this procedure Vol. 107, No. 6 / UPPER EXTREMITY MICROSURGERY 1533 FIG. 6. (Above, left) Intraoperative view of the forearm of a 12-year-old boy after a propeller injury. Note the disrupted median nerve (over background). (Above, right) Intraoperative view after innervated gracilis transfer. The skin paddle for monitoring is over the proximal muscle. (Below) Extension (left) and flexion (right) at 8 months postoperatively. certainly has advantages over implant arthroplasty and fusion, it is a complex undertaking and should be used selectively by surgeons with experience. Thumb reconstruction. Toe transfer in one of its forms offers many of the best ways to reconstruct defects of the thumb.55 For reconstruction of the pulp of the thumb alone, only the lateral pulp of the great toe is taken; this may be innervated by the lateral digital and deep peroneal nerves. This flap provides excellent reconstruction for the thumb and leaves little morbidity at the foot. For partial thumb amputations (those from the mid-proximal phalanx level), a great toe “wrap-around” flap may be used (Fig. 7). This modification takes only the distal phalanx and surrounding soft tissue, which is trimmed to approximate the circumference of the missing thumb.56,57 This technique requires the use of an intercalated bone graft segment between the proximal phalanx of the thumb and distal phalanx of the toe. Although this is arguably the most cosmetic type of thumb reconstruction, it does not recon- FIG. 7. Patient 1 year after great toe wrap-around reconstruction of the left thumb. struct missing joints. Because it leaves the proximal phalanx intact, it has the potential to impart less morbidity at the foot than whole great toe transfer. Wei et al58 advocate the “trimmed toe” technique to circumvent the lack of motion of the wrap-around flap. In this technique, the entire great toe is trimmed, including both the soft-tissue and bony structures, to give a recon- 1534 structed thumb of appropriate circumference. Their report showed a reasonable return of motion in the trimmed joints. In cases of loss of the entire thumb, the entire great toe may be transferred. It should be noted that the metatarsophalangeal joints act primarily in the extension arc. To avoid hyperextension of this joint when transferred to the hand, a dorsal oblique osteotomy is used to place the toe in the proper position on the hand. The flexor and extensor tendons are taken with a total great toe transfer, and anastomosis is ideally performed at the wrist level to decrease the incidence of tendon adhesions. The flexor tendon may be harvested through a separate incision in the non–weight-bearing surface of the arch of the foot and, if more length is needed, another incision may be made at the level of the tarsal tunnel. The extensor tendon (extensor hallucis longus) is usually taken through the dorsal incision made for dissection of the neurovascular structures. Transfer of all parts of the great toe imparts some morbidity to the foot, but the effect when evaluated with gait studies is generally minimal. Certainly, the tradeoff of a thumb for the loss of the great toe is usually well-accepted by the patient. The primary disadvantage of these techniques is their inherent complexity and, although they offer superb reconstructive options in patients with loss of all or part of the thumb, their application should probably be limited to those practitioners with experience. Digital reconstruction. The second or second and third toes may be transferred in a manner similar to that used with the great toe to reconstruct missing digits. A single toe transfer for a single missing digit is generally not indicated, and the application of this technique is generally reserved for those patients who have suffered a transmetatarsal amputation (metacarpal hand).59 Smaller portions of the second toe can be used for pulp and/or nail losses, but this type of procedure is usually less necessary in the digits than in the thumb. In the case of multiple digital loss, two fingers may be reconstructed with either a double toe (second and third combined) from one foot60 or a second toe transfer from each foot. The loss of the second toe only imparts very minimal morbidity, but the loss of two toes from one foot leaves a significant deficit.61 PLASTIC AND RECONSTRUCTIVE SURGERY, May 2001 CONCLUSIONS This has been a brief overview of microsurgical reconstruction of the upper extremity. The number of flaps available for hand and arm reconstruction is large, and only a few have been discussed here. There are a number of flaps other than those discussed that have application in the upper extremity, but I hope this overview has given the reader a number of options that offer a solution for most reconstructive problems. For further reading, one should seek out one of the many texts available on the subject.12,62,63 William C. Pederson, M.D. The Hand Center of San Antonio 9150 Huebner Road, Suite 290 San Antonio, Texas 78240 [email protected] REFERENCES 1. Komatsu, S., and Tamai, S. Successful replantation of a completely cut-off thumb. Plast. Reconstr. Surg. 42: 374, 1968. 2. Cobbett, J. R. Free digital transfer: Report of a case of transfer of a great toe to replace an amputated thumb. J. Bone Joint Surg. (Br.) 51: 677, 1969. 3. Daniel, R. K., and Taylor, G. I. Distant transfer of an island flap by microvascular anastomoses: A clinical technique. Plast. Reconstr. Surg. 52: 111, 1973. 4. Cormack, G. C., and Lamberty, B. G. Fasciocutaneous vessels in the upper arm: Application to the design of new fasciocutaneous flaps. Plast. Reconstr. Surg. 74: 244, 1984. 5. Chen, H. C., Buchman, M. T., and Wei, F. C. Free flaps for soft tissue coverage in the hand and fingers. Hand Clin. 15: 541, 1999. 6. Brown, D. M., Upton, J., and Khouri, R. K. Free flap coverage of the hand. Clin. Plast. Surg. 24: 57, 1997. 7. Upton, J., Havlik, R. J., and Khouri, R. K. Refinements in hand coverage with microvascular free flaps. Clin. Plast. Surg. 19: 841, 1992. 8. Godina, M. Wound care and timing of microvascular flap transfer to the lower leg. In A Thesis on the Management of Injuries to the Lower Extremity. Ljubljana: Presernova Druzba, 1991. Pp. 77– 84. 9. Chang, N., and Mathes, S. J. Comparison of the effect of bacterial inoculation in musculocutaneous and random-pattern flaps. Plast. Reconstr. Surg. 70: 1, 1982. 10. Calderon, W., Chang, N., and Mathes, S. J. Comparison of the effect of bacterial inoculation in musculocutaneous and fasciocutaneous flaps. Plast. Reconstr. Surg. 77: 785, 1986. 11. Bailey, B. N., and Godfrey, A. M. Latissimus dorsi muscle free flaps. Br. J. Plast. Surg. 35: 47, 1982. 12. Jones, N. F., and Lister, G. D. Free skin and composite flaps. In D. P. Green, R. N. Hotchkiss, and W. C. Pederson (Eds.), Operative Hand Surgery, 4th Ed. Philadelphia: Churchill Livingstone, 1999. 13. Whitney, T. M., Buncke, H. J., Alpert, B. S., Buncke, G. M., and Lineaweaver, W. C. The serratus anterior free-muscle flap: Experience with 100 consecutive cases. Plast. Reconstr. Surg. 86: 481, 1990. Vol. 107, No. 6 / UPPER EXTREMITY MICROSURGERY 14. Favero, K. J., Wood, M. B., and Meland, N. B. Transfer of innervated latissimus dorsi free musculocutaneous flap for the restoration of finger flexion. J. Hand Surg. (Am.) 18: 535, 1993. 15. Horch, R. E., and Stark, G. B. The rectus abdominis free flap as an emergency procedure in extensive upper extremity soft-tissue defects. Plast. Reconstr. Surg. 103: 1421, 1999. 16. Rao, V. K., and Baertsch, A. Microvascular reconstruction of the upper extremity with the rectus abdominis muscle. Microsurgery 15: 746, 1994. 17. Press, B. H., Chiu, D. T., and Cunningham, B. L. The rectus abdominis muscle in difficult problems of hand soft tissue reconstruction. Br. J. Plast. Surg. 43: 419, 1990. 18. Gordon, L., Levinsohn, D. G., Finkemeier, C., Angeles, A., and Deutch, H. The serratus anterior free-muscle transplant for reconstruction of the injured hand: An analysis of the donor and recipient sites. Plast. Reconstr. Surg. 92: 97, 1993. 19. Derby, L. D., Bartlett, S. P., and Low, D. W. Serratus anterior free-tissue transfer: Harvest-related morbidity in 34 consecutive cases and a review of the literature. J. Reconstr. Microsurg. 13: 397, 1997. 20. Braun, F. M., Hoang, P., Merle, M., Van Genechten, F., and Foucher, G. Technique and indications of the forearm flap in hand surgery: A report of thirty-three cases. Ann. Chir. Main 4: 85, 1985. 21. Soutar, D. S., and Tanner, N. S. B. The radial forearm flap in the management of soft tissue injuries of the hand. Br. J. Plast. Surg. 37: 18, 1984. 22. Yajima, H., Tamai, S., Yamauchi, T., and Mizumoto, S. Osteocutaneous radial forearm flap for hand reconstruction. J. Hand Surg. (Am.) 24: 594, 1999. 23. Foucher, G., Van Genechten, F., Merle, M., and Michon, J. A compound radial artery forearm flap in hand surgery: An original modification of the Chinese forearm flap. Br. J. Plast. Surg. 37: 139, 1984. 24. Katsaros, J., Schusterman, M., Beppu, M., Banis, J. C., Jr., and Acland, R. D. The lateral upper arm flap: Anatomy and clinical applications. Ann. Plast. Surg. 12: 489, 1984. 25. Chen, H. C., and el-Gammal, T. A. The lateral arm fascial free flap for resurfacing of the hand and fingers. Plast. Reconstr. Surg. 99: 454, 1997. 26. Harpf, C., Papp, C., Ninkovic, M., Anderl, H., and Hussl, H. The lateral arm flap: Review of 72 cases and technical refinements. J. Reconstr. Microsurg. 14: 39, 1998. 27. Arnez, Z. M., Kersnic, M., Smith, R. W., and Godina, M. Free lateral arm osteocutaneous neurosensory flap for thumb reconstruction. J. Hand Surg. (Br.) 16: 395, 1991. 28. Yousif, N. J., Warren, R., Matloub, H. S., and Sanger, J. R. The lateral arm fascial free flap: Its anatomy and use in reconstruction. Plast. Reconstr. Surg. 86: 1138, 1990. 29. Scheker, L. R., Kleinert, H. E., and Hanel, D. P. Lateral arm composite tissue transfer to ipsilateral hand defects. J. Hand Surg. (Am.) 12: 665, 1987. 30. Burns, J. T., and Schlafly, B. Use of the parascapular flap in hand reconstruction. J. Hand Surg. (Am.) 11: 872, 1986. 31. Barwick, W. J., Goodkind, D. J., and Serafin, D. The free scapular flap. Plast. Reconstr. Surg. 69: 779, 1982. 32. Thoma, A., and Heddle, S. The extended free scapular flap. Br. J. Plast. Surg. 43: 709, 1990. 1535 33. Germann, G., Bickert, B., Steinau, H. U., Wagner, H., and Sauerbier, M. Versatility and reliability of combined flaps of the subscapular system. Plast. Reconstr. Surg. 103: 1386, 1999. 34. Evans, G. R., and Luethke, R. W. A latissimus/scapula combined myo-osseous free flap based on the subscapular artery used for elbow reconstruction. Ann. Plast. Surg. 30: 175, 1993. 35. Hing, D. N., Buncke, H. J., and Alpert, B. S. Use of the temporoparietal free fascial flap. Plast. Reconstr. Surg. 81: 534, 1988. 36. Abul-Hassan, H. S., von Drasek Ascher, G., and Acland, R. D. Surgical anatomy and blood supply of the fascial layers of the temporal region. Plast. Reconstr. Surg. 77: 17, 1986. 37. Upton, J., Rogers, C., Durham-Smith, G., and Swartz, W. M. Clinical applications of free temporoparietal flaps in hand reconstruction. J. Hand Surg. (Am.) 11: 475, 1986. 38. Weiland, A. J., Kleinert, H. E., Kutz, J. E., and Daniel, R. K. Free vascularized bone grafts in surgery of the upper extremity. J. Hand Surg. (Am.) 4: 129, 1979. 39. Yajima, H., Tamai, S., Ono, H., Kizaki, K., and Yamauchi, T. Free vascularized fibula grafts in surgery of the upper limb. J. Reconstr. Microsurg. 15: 515, 1999. 40. Ihara, K., Doi, K., Yamamoto, M., and Kawai, S. Free vascularized fibular grafts for large bone defects in the extremities after tumor excision. J. Reconstr. Microsurg. 14: 371, 1998. 41. Gerwin, M., and Weiland, A. J. Vascularized bone grafts to the upper extremity: Indications and technique. Hand Clin. 8: 509, 1992. 42. Tang, C. H. Reconstruction of the bones and joints of the upper extremity by vascularized free fibular graft: Report of 46 cases. J. Reconstr. Microsurg. 8: 285, 1992. 43. Manktelow, R. T., and Anastakis, D. J. Functioning free muscle transfers. In D. P. Green, R. N. Hotchkiss, and W. C. Pederson (Eds.), Operative Hand Surgery, 4th Ed. Philadelphia: Churchill Livingstone, 1999. 44. Park, C., and Shin, K. S. Functioning free latissimus dorsi muscle transplantation: Anterogradely positioned usage in reconstruction of extensive forearm defect. Ann. Plast Surg. 27: 87, 1991. 45. Lister, G. D., Kaisman, M., and Tsai, T. M. Reconstruction of the hand with free microneurovascular toe-tohand transfer: Experience with 54 toe transfers. Plast. Reconstr. Surg. 71: 372, 1983. 46. O’Brien, B., Gould, J. S., Morrison, W. A., Russell, R. C., MacLeod, A. M., and Pribaz, J. J. Free vascularized small joint transfer to the hand. J. Hand Surg. (Am.) 9: 634, 1984. 47. Foucher, G., Sammut, D., and Citron, N. Free vascularized toe-joint transfer in hand reconstruction: A series of 25 patients. J. Reconstr. Microsurg. 6: 201, 1990. 48. Tsai, T. M., and Lim, B. H. Free vascularized transfer of the metatarsophalangeal and proximal interphalangeal joints of the second toe for reconstruction of the metacarpophalangeal joints of the thumb and index finger using a single vascular pedicle. Plast. Reconstr. Surg. 98: 1080, 1996. 49. Chen, S. H., Wei, F. C., and Chen, H. C. Vascularized toe joint transplantation. Hand Clin. 15: 613, 1999. 50. Imamura, K., Nagatani, Y., and Hirano, E. Vascularized toe-to-finger joint transplantation: 11 patients followed for 4 years. Acta Orthop. Scand. 63: 457, 1992. 51. Chen, S. H., Wei, F. C., Chen, H. C., Hentz, V. R., Chuang, 1536 52. 53. 54. 55. 56. 57. D. C., and Yeh, M. C. Vascularized toe joint transfer to the hand. Plast. Reconstr. Surg. 98: 1275, 1996. Ellis, P. R., Hanna, D., and Tsai, T. M. Vascularized single toe joint transfer to the hand. J. Hand Surg. (Am.) 16: 160, 1991. Ishida, O., and Tsai, T. M. Free vascularized whole joint transfer in children. Microsurgery 12: 196, 1991. Singer, D. I., O’Brien, B. M., McLeod, A. M., Morrison, W. A., and Angel, M. F. Long-term follow-up of free vascularized joint transfers to the hand in children. J. Hand Surg. (Am.) 13: 776, 1988. Lister, G. The choice of procedure following thumb amputation. Clin. Orthop. 195: 45, 1985. Morrison, W. A., O’Brien, B. M., and MacLeod, A. M. Thumb reconstruction with a free neurovascular wrap-around flap from the big toe. J. Hand Surg. (Am.) 5: 575, 1980. Doi, K. Microsurgical thumb reconstruction: Report of six cases with a wrap-around free flap from the big toe and an iliac bone graft. Ann. Acad. Med. Singap.11: 225, 1982. PLASTIC AND RECONSTRUCTIVE SURGERY, May 2001 58. Wei, F. C., Chen, H. C., Chuang, C. C., and Chen, S. H. Microsurgical thumb reconstruction with toe transfer: Selection of various techniques. Plast. Reconstr. Surg. 93: 345, 1994. 59. Wei, F. C., el-Gammal, T. A., Lin, C. H., Chuang, C. C., Chen, H. C., and Chen, S. H. Metacarpal hand: Classification and guidelines for microsurgical reconstruction with toe transfers. Plast. Reconstr. Surg. 99: 122, 1997. 60. Wei, F. C., Chen, H. C., Chuang, C. C., and Noordhoff, M. S. Reconstruction of the hand, amputated at the metacarpophalangeal level, by means of combined second and third toes from each foot: A case report. J. Hand Surg. (Am.) 11: 340, 1986. 61. Barca, F., Santi, A., Tartoni, P. L., and Landi, A. Gait analysis of the donor foot in microsurgical reconstruction of the thumb. Foot Ankle Int. 16: 201, 1995. 62. Foucher, G. Reconstructive Surgery in Hand Mutilation. St. Louis: Mosby, 1997. 63. Serafin, D. Atlas of Microsurgical Composite Tissue Transplantation. Philadelphia: Saunders, 1996. Self-Assessment Examination Upper Extremity Microsurgery by William C. Pederson, M.D. 1. THE LARGEST SINGLE MUSCLE AVAILABLE FOR MICROSURGICAL TRANSFER IS THE: A) Rectus abdominis B) Pectoralis major C) Gluteus maximus D) Latissimus dorsi E) Trapezius 2. HARVEST OF THE SERRATUS ANTERIOR MUSCLE CARRIES THE RISK OF DAMAGE TO: A) The thoracodorsal nerve B) The pleura C) The long thoracic nerve D) The medial pectoral nerve E) The axillary artery 3. THE MOST COMMON DONOR-SITE COMPLICATION OF TEMPOROPARIETAL FASCIA HARVEST IS: A) Facial nerve injury B) Temporal wasting C) Temporomandibular joint malfunction D) Alopecia E) Necrosis of the scalp 4. A DEFINITE INDICATION FOR INNERVATED GRACILIS TRANSFER TO THE FOREARM WOULD BE: A) Volkmann’s ischemic contracture B) Electrical burn to the forearm C) High median nerve injury D) Degloving injury to the forearm E) Radial nerve paralysis 5. THE TYPE OF GREAT TOE TRANSFER OFFERING THE BEST POTENTIAL FOR MOTION WOULD BE: A) Great toe wrap-around B) Whole great toe transfer C) Trimmed great toe transfer D) Great toe pulp transfer E) Great toe interphalangeal joint transfer 6. THE TERM “NECRECTOMY” AS APPLIED TO WOUND DEBRIDEMENT IMPLIES THAT: A) Only the margins of the wounds are excised B) All tissues that may have been damaged, including nerves and vessels, are excised C) All contaminated or nonviable tissue is excised with the exception of major neurovascular structures D) All deep structures are left intact, regardless of contamination, because coverage with a free flap will take care of any residual necrotic tissue or contamination E) Only obviously necrotic tissue is excised To complete the examination for CME credit, turn to page 1635 for instructions and the response form.