Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
History of invasive and interventional cardiology wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Electrocardiography wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Heart failure wikipedia , lookup
Aortic stenosis wikipedia , lookup
Coronary artery disease wikipedia , lookup
Cardiac surgery wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Myocardial infarction wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Atrial septal defect wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
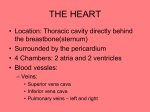
Chest X-ray signs of cardiac disease A. Swartbooi Diagnostic Radiology, UFS 2 March 2012 Congenital Heart Disease Numerous clinically important imaging signs in congenital cardiovascular disease. It is important that Radiologists must be able to recognize these signs and must understand their causes in order to provide accurate diagnoses of abnormalities affecting the heart and vessels of the thorax. Congenital Heart Disease Transposition of the Great Arteries – Most common cyanotic congenital heart lesion – 5%–7% of congenital cardiac malformations – isolated in 90% – Transposition of the great arteries is produced by a ventriculoarterial – – – – discordance in which the aorta arises from the morphologic right ventricle and the pulmonary artery arises from the morphologic left ventricle Pulmonary artery is situated to the right of its normal location Results in the apparent narrowing of the superior mediastinum on radiographs Patent ASD, VSD, Foramen ovale, systemic collaterals to sustain life Atrial border is abnormally convex, and the left atrium commonly is enlarged because of increased pulmonary blood flow. TGA – EGG ON STRING SIGN Congenital Heart Disease Total Anomalous Pulmonary Venous Return – Occurs when the pulmonary veins fail to drain into the left atrium and instead form an aberrant connection with some other cardiovascular structure – 2% of cardiac malformations – Four types of TAPVR may be defined Type I (55%) – – – – The anomalous pulmonary veins terminate at the supracardiac level. Typically, four anomalous pulmonary veins converge behind the left atrium and form a common vein, known as the vertical vein, this passes anterior to the left pulmonary artery and the left main bronchus to join the innominate vein Less commonly, drainage to the left brachiocephalic vein, right superior vena cava, or azygos v Classic snowman sign Type II (30%) – – Involves a pulmonary venous connection at the cardiac level. Pulmonary veins join either the coronary sinus or the right atrium. Congenital Heart Disease Type III (13%) – – – Involves a connection at the infracardiac or infradiaphragmatic level Pulmonary veins join behind the left atrium to form a common vertical descending vein, which courses anterior to the esophagus and passes through the diaphragm at the esophageal hiatus Vertical vein usually joins the portal venous system but occasionally connects directly to the ductus venosus, the hepatic veins, or the inferior vena cava. Type IV (2%) – Involves anomalous venous connections at two or more levels. – In the most common pattern, the vertical vein drains into the left innominate vein, and the anomalous vein or veins from the right lung drain into either the right atrium or the coronary sinus – Generally associated with other major cardiac lesions. TAPVR I – SNOWMAN SIGN Congenital Heart Disease Partial Anomalous Pulmonary Venous Return – – – – – – Anomalous pulmonary vein drains any or all of the lobes of the right lung Vein curves outward along the right cardiac border, usually from the middle of the lung to the cardiophrenic angle, and usually empties into the inferior vena cava but also may drain into the portal vein, hepatic vein, or right atrium Size of the vein generally increases as it descends. Characteristic appearance of the vein has led to its comparison to a scimitar Flow through the scimitar vein produces a left-to-right shunt that is usually hemodynamically insignificant. Part of Scimitar syndrome when associated with: Hypoplasia of the right lung with dextroposition of the heart, Hypoplasia of the right pulmonary artery, and Anomalous arterial supply of the right lower lobe from the abdominal aorta PAPVR – SCIMITAR SIGN Congenital Heart Disease Endocardial Cushion Defects – Interruption of the normal development of the endocardial tissues during gestation which normally forms the lower portion of the atrial septum, the upper portion of the interventricular septum, and the septal leaflets of the mitral valve and the tricuspid valve – 4% of all cases of congenital heart disease – Gooseneck-shaped deformity Caused by a deficiency of both the conus and sinus portions of the interventricular septum, with narrowing of the left ventricular outflow tract. Characteristic shape by concavity of the interventricular septum below the mitral valve, along with the elongation and narrowing of the left ventricular outflow tract Endocardial cushion defect GOOSENECK SIGN Congenital Heart Disease Tetralogy of Fallot – 10%–11% of cases of congenital heart disease – As a result of single defect, an anterior malalignment of the conal septum – Components: Ventricular septal defect Infundibular pulmonary stenosis Overriding aorta Right ventricular hypertrophy. – Heart has the shape of a wooden shoe or boot – Blood flow to the lungs is usually reduced Tetralogy of Fallot – BOOT SHAPED SIGN Congenital Heart Disease Aortic Coarctation – 5%–10% of congenital cardiac lesions – Produced by a deformity of the aortic media and intima, which causes a – – – – prominent posterior infolding of the aortic lumen Occurs at or near the junction of the aortic arch and the descending thoracic aorta Infolding cause eccentric narrowing of the lumen at the level where the ductus or ligamentum arteriosus inserts anteromedially Resultant luminal narrowing in turn obstructs the flow of blood from the left ventricle Classic radiologic signs Figure-of-three sign Reverse figure-of-three sign Rib notching on CXR pathognomonic Aortic Coarctation – Figure of Three, and Reverse Figure of Three Congenital Heart Disease Ebstein Anomaly – 0.5%–0.7% of cases of congenital heart disease. – Characterized by the downward displacement of the septal leaflets and posterior leaflets of the tricuspid valve into the inflow portion of the right ventricle. – Results in the formation of a common right ventriculoatrial chamber and causes tricuspid regurgitation. – Insufficiency of the tricuspid valve leads to dilatation of the right ventricular outflow tract and all proximal right heart structures, – Most consistent imaging feature is right atrial enlargement; Ebstein Anomaly – Box Shaped Heart Useful Approach Clinical A. – Cyanotic vs Acyanotic Thoracic Musculoskeletal Structures 1. – prior operations, rib or sternal deformities or sternal wire sutures Pulmonary vascularity 2. – ⇧ pulmonary arterial circulation versus pulmonary venous hypertension Overall Heart Size 3. – Assessing CT index Useful Approach Specific Chamber Enlargement 4. – Right retrocardiac double density Splayed carina, horiz L bronchus Posterior displacement of the left upper lobe bronchus Enlarged atrial appendage – RA – Great arteries – Ascending aorta, LA 5. Lateral bulging and elongation of the right heart border LV & RV PA View Lat ⇨ – Aortic knob, – Main pulmonary arterial segment Acquired Heart Disease In the evaluation of acquired heart disease a systematic approach is directed toward discerning the pertinent findings from the radiograph and, for each finding, narrowing the diagnostic considerations Cardiac size and chamber enlargement can be inferred by evaluation of the chest radiograph. The normal heart will occupy slightly less than 50% of the transverse dimension of the thorax. Anatomy Anatomy Acquired Heart Disease Small Heart RADIOGRAPHIC FEATURES OF AORTIC STENOSIS Enlargement of the ascending aorta due to poststenotic dilatation Mild or no cardiomegaly in compensated stage Substantial cardiomegaly occurs only after myocardial failure has ensued No pulmonary venous hypertension or pulmonary edema is seen during most of the course of this disease Calcification of aortic valve may be discernible on radiograph but is more readily shown on CT RADIOGRAPHIC FEATURES OF ARTERIAL HYPERTENSION Enlargement of the thoracic aorta— ascending, arch, and descending aorta Mild or no cardiomegaly until the onset of myocardial failure No pulmonary edema or pulmonary venous hypertension until the occurrence of diastolic dysfunction due to severe left ventricular hypertrophy or myocardial failure RADIOGRAPHIC FEATURES OF MITRAL STENOSES Pulmonary venous hypertension or edema is present Pulmonary edema may be observed intermittently Mild cardiomegaly is seen in isolated mitral stenoses Enlargement of the left atrium is characteristic Enlargement of the left atrial appendage is frequent and suggests a rheumatic etiology Right ventricular enlargement indicates some degree of pulmonary arterial hypertension or associated tricuspid regurgitation. RADIOGRAPHIC FEATURES OF MITRAL STENOSES Enlargement of the pulmonary arterial segment is indicative of associated pulmonary arterial hypertension Right ventricular enlargement in the absence of prominence of the main pulmonary artery suggests associated tricuspid regurgitation. The right atrium is also enlarged with tricuspid regurgitation The ascending aorta and aortic arch are usually inconspicuous in isolated mitral stenosis. Even slight enlargement of the thoracic aorta raises the question of associated aortic valve disease RADIOGRAPHIC FEATURES OF HYPERTROPHIC CARDIOMYOPATHY Normal in most patients Mild cardiomegaly and pulmonary venous hypertension in a minority of patients Left atrial enlargement can be caused by associated mitral insufficiency or reduced left ventricular compliance In the obstructive form (subaortic stenosis), ascending aortic enlargement is infrequent Left ventricular enlargement may occur in end-stage disease RADIOGRAPHIC FEATURES OF RESTRICTIVE CARDIOMYOPATHY Pulmonary venous hypertension is typical Pulmonary edema may occur intermittently Normal heart size or mild cardiomegaly in most patients Left atrial enlargement Left atrial appendage is typically not enlarged Moderate to severe cardiomegaly can ensue in end-stage disease RADIOGRAPHIC FEATURES OF ACUTE MYOCARDIAL INFARCTION Normal chest x-ray in about 50% of first acute infarctions Normal heart size with pulmonary venous hypertension or pulmonary edema in about 50% of first acute infarctions Cardiomegaly is usually indicative of acute infarction in a patient with history of previous infarctions Cardiomegaly may be indicative of ischemic cardiomyopathy RADIOGRAPHIC FEATURES OF ACUTE MYOCARDIAL INFARCTION Signs of complication of acute myocardial infarction Intractable pulmonary edema may occur with papillary muscle rupture (mitral regurgitation) or ventricular septal rupture (left to right shunt). Enlarged cardiac silhouette may be caused by pericardial effusion. Abnormal cardiac contour may be a sign of true (bulge of the anterolateral or apical regions) or false (bulge of the posterior or diaphragmatic regions) aneurysms RADIOGRAPHIC FEATURES OF CONSTRICTIVE PERICARDITIS Pulmonary venous hypertension Normal heart size or mild cardiomegaly Left atrial enlargement may be discernible Flattened cardiac contours are pathognomonic but infrequently observed Calcification of the cardiac margin, especially the atrioventricular and interventricular grooves Acquired Heart Disease Large Heart RADIOGRAPHIC FEATURES OF AORTIC REGURGITATION Absence of pulmonary venous hypertension or pulmonary edema until late in the course of this lesion Moderate to severe cardiomegaly Left ventricular enlargement Enlargement of ascending aorta and aortic arch RADIOGRAPHIC FEATURES OF MITRAL REGURGITATION Variable degree of pulmonary venous hypertensive or pulmonary edema (less severe than with mitral stenosis) Moderate to severe cardiomegaly Left ventricular enlargement Left atrial enlargement Enlargement of left atrial appendage RADIOGRAPHIC FEATURES OF TRICUSPID REGURGITATION No pulmonary venous hypertension or pulmonary edema (isolated tricuspid regurgitation) Pulmonary venous hypertension or edema indicates associated mitral valve disease Moderate to severe cardiomegaly Right ventricular enlargement Right atrial enlargement RADIOGRAPHIC FEATURES OF CONGESTIVE (DILATED) CARDIOMYOPATHY Pulmonary venous hypertension or pulmonary edema may be but is not invariably present Moderate to severe cardiomegaly Left ventricular enlargement Left atrial enlargement is infrequently evident but can be caused by mitral regurgitation caused by left ventricular enlargement Congestive Heart Failure RADIOGRAPHIC FEATURES OF PERICARDIAL EFFUSION No pulmonary venous hypertension or pulmonary edema Moderate to severe enlargement of cardiac silhouette Associated pleural effusion is not uncommon Specific features, such as “fat pad” and/or “variable density” signs, are infrequently evident ENLARGEMENT OF MAIN PULMONARY ARTERY Etiology – – – – – – – – Pulmonary arterial hypertension Excess pulmonary blood flow (left to right shunts, chronic high output states) Valvular pulmonic stenosis Pulmonary regurgitation Congenital absent pulmonary valve (aneurysmal pulmonary artery) Absence of left pericardium Aneurysm of pulmonary artery Idiopathic dilatation of pulmonary artery Cardiac Calcification Ascending aortic calcification – – Mitral annular calcification – – – Dense C-shaped calcification in the region of the mitral valve. It may be a causative factor of mitral regurgitation. It is frequently observed in apparently normal elderly patients. Aortic annular calcification – – Most frequently observed on the right anterolateral margin of the ascending aorta in elderly individuals, especially in the presence of aortic valve disease. In the past, it was considered to be a characteristic of syphilitic aortitis. A circular calcification in the region of the aortic valve. Extension of this calcification into the region of the conducting system can produce complete heart failure. Valvular calcification (aortic and mitral). – Calcification of the aortic valve of sufficient density and extent to be visualized on the radiograph is nearly always associated with hemodynamically important aortic stenosis (gradient more than 50 mm Hg). Cardiac Calcification Coronary arterial calcification – – Left ventricular mural calcification – Most frequently located in the anterolateral or apical regions of the left ventricle and marks the site of a transmural MI or aneurysm. Pericardial calcification – – Coronary arterial calcification is frequently observed by fluoroscopy or CT. It must be both dense and extensive to be recognized on the thoracic radiograph. Indicative of constrictive pericarditis. Located usually in the interventricular or atrioventricular grooves of the heart. Unusual sites – – – – Intracardiac tumor (left atrial myxoma), Pericardial tumor (dermoid), or Healed granulomas (myocardial tuberculoma). An extremely rare process of the left ventricle, Loeffler's eosinophilic fibroplasia, can cause calcification of the left ventricular wall. Cardiac Calcification Reference Thoracic Imaging: Pulmonary and Cardiovascular Radiology, 1st Edition; Webb, Richard W.; Higgins, Charles B. page 655-702. Grainger & Allison's Diagnostic Radiology, 5th ed; page 450-526 Classic Imaging Signs of Congenital Cardiovascular Abnormalities, RadioGraphics 2007; 27:1323–1334 http://radiologymasterclass.co.uk/tutorials/chest/chest_path ology/chest_pathology_page8.html(last accessed 22/02/12) Acquired Heart Disease Approach Cardiac Valvular Lesions Signpost Signpost If no signposts are present, then the diagnosis is unlikely to be a valvular lesion. The absence of signposts should direct attention to a disease directly afflicting the myocardium or pericardium, such as acute MI, hypertrophic cardiomyopathy, restrictive cardiomyopathy, and constrictive pericardial disease. However, even these latter diseases sometimes induce left atrial enlargement, as stated above. Cardiac Size ENLARGEMENT OF THE MIDDLE SEGMENT OF LEFT HEART BORDER Etiology – – – – – – – – – – – Dilated left atrial appendage (rheumatic mitral valve disease) Partial absence of left pericardium Enlargement of right ventricular outlet region such as occurs with left-to-right shunts Asymmetric form of hypertrophic cardiomyopathy (minority of cases) Levo transposition of the great arteries Juxtaposition of atrial appendages (rare anomaly usually associated with tricuspid atresia) Left ventricular aneurysm Cardiac tumor Aneurysm or pseudoaneurysm of left circumflex coronary artery Pericardial cyst or tumor Mediastinal tumor EVAGINATION OF LEFT LOWER HEART BORDER Etiology – – – – – – Ventricular aneurysm Ventricular tumor Pericardial cyst, diverticulum or tumor Left ventricular diverticulum Mediastinal or lung tumor Pericardial fat pad ENLARGEMENT OF RIGHT HEART AND BORDER Etiology – – – – – – – – Right atrial enlargement Pericardial fat pad Eventration or hernia of diaphragm Pericardial cyst or diverticulum Pericardial tumor Cardiac tumor Diaphragmatic tumor Mediastinal tumor