Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Surround optical-fiber immunoassay wikipedia , lookup
Fatty acid metabolism wikipedia , lookup
Community fingerprinting wikipedia , lookup
Genetic code wikipedia , lookup
Matrix-assisted laser desorption/ionization wikipedia , lookup
Biosynthesis wikipedia , lookup
Metalloprotein wikipedia , lookup
Amino acid synthesis wikipedia , lookup
Biochemistry wikipedia , lookup
Mass spectrometry wikipedia , lookup
CLIN. CHEM. 39/1, 66-71 (1993)
Rapid Diagnosis of Phenylketonuria by Quantitative Analysis for Phenylalanine and
Tyrosine in Neonatal Blood Spots by Tandem Mass Spectrometry
H. Chace,’ David S. Mlllington,’
Hofman3
Donald
Naoto Terada,2 Stephen G. Kahier,’ Charles
A new method for quantifying specific amino acids in
small volumes of plasma and whole blood has been
developed. Based on isotope-dilution tandem mass spectrometry, the method takes only a few minutes to perform
and requires minimal sample preparation. The accurate
assay of both phenylalanine and tyrosine in dried blood
spots used for neonatal screening for phenylketonuria in
North Carolina successfully differentiated infants who had
been classified as normal, affected, and falsely positiveby
current fluorometric
methods. Because the mass-spectro-
metric method also recognizes other aminoacidemias
simultaneously and is capable of automation, it represents a useful development toward a broad-spectrum
neonatal screening method.
R. Roe,’
and Lindsay
F.
referred to as liquid secondary ionization (LSI)-is
suitable for the rapid assay of specific components
in complex biological samples (5). The basis for this type of
analysis is the production of mostly intact molecular
species from a complex mixture by use of a “soft”
ionization
technique, after which molecular
fragments
are identified from specific components induced by collisions with neutral gas molecules. The use of two mass
analyzers
separated
by a region in which the collisionally induced fragmentation
takes place allows highly
selective and specific analysis for compounds of various
structural
classes. Time-consuming
chromatographic
separations are not needed because separation
and analysis take place simultaneously
and entirely within the
-
mass spectrometer.
AddItIonal Keyphrases: heritable disorders
metabolism
.
amino acids
tyrosinemia
Screening
neonates
for phenylketonuria
(PKU), an
inborn error of metabolism
resulting from phenylalanine hydroxylase
deficiency (McKusick 261600), is beneficial because it provides for early diagnosis and treatment (1, 2). The collecting of specimens as blood spets
on filter paper and the subsequent
quantitative
analysis
for phenylalanine
(Phe) is used in neonatal screening
laboratories worldwide
(3). Most of the analytical methods, including the fluorometric
assay currently used in
the North Carolina
State Screening Laboratory (4),
generate a relatively high rate of false-positive
results
(typically about 0.1% of those screened), which require
follow-up analysis for amino acids. In North Carolina
during 1991, >100 samples were followed up for initial
screening
results of above-normal
Phe concentrations,
of which only 2 were subsequently
confirmed as positive
for PKU. Typically, five or six cases are detected annually, but the false-positive
rate is still high. These
false-positive
results are generally assumed to be due to
initially high Phe concentrations
that later decrease to
within the normal range.
Tandem
mass spectrometry
(MS/MS)
coupled
with
fast atom
bombardment
ionization-more
of LSIMS/MS
to the quantitative
analysis
for Phe and
tyrosine (Tyr) in plasma and neonatal blood spots for the
rapid diagnosis of PKU and related disorders of metabolism of aromatic amino acids.
Materials and Methods
Materials
Solvents were high-purity grade (Burdick and Jackson, Muskegon, MI). The esterifying
agent, 3 moltL HC1
in n-butanol,
was obtained from Regis (Morton Grove,
IL). [2H5]L-Phenylalanine
(98 atom%), [2H41L-tyrosine
(98 atom%), and [2H3-methyl]L-leucine (99 atom%) were
obtained from MSD Isotopes (Montreal, Canada). The
unlabeled
Phe and Tyr and amino acid standard
kits
were from Aldrich (Milwaukee,
WI) and Sigma (St.
Louis, MO). Stock solutions of the analytical standards
were prepared in 0.1 mol/L HC1 and stored at 4#{176}C.
Filter paper for the preparation of blood spots was from
Schleicher and Schuell (Keene, NH; cat. no. 903).
accurately
1Department of Pediatrics, Division of Genetics and Metabolism, Duke University Medical Center, Box 3028, Durham, NC
27710.
‘Department
of Pediatrics, Kyoto Prefectural University of
Medicine, Kawaramachi Hirokoji Kamikyo-ku, Kyoto 605, Japan.
3State of North Carolina Department of Environment, Health,
and Natural Resources, Division of Laboratory Services, 306 N.
Wilmington St., Raleigh, NC 27601.
4Nonstandard abbreviations: PKU, phenylketonuria;
MS/MS,
tandem mass spectroscopy; and LSI, liquid secondary ionization.
Received April 20, 1992; accepted August 19, 1992.
66 CLINICALCHEMISTRY,Vol. 39, No. 1, 1993
In this laboratory,
we have developed
and applied
LSIMSIMS
for the detection
of abnormal
urine and
plasma metabolites
in patients with inborn errors of
metabolism
(6, 7) and have described
a general
LSIMSfMS method to analyze for amino acids in blood
and plasma (8). Here we report the specific application
Samples
Newborn screening cards containing blood spots collected on the third day postpartum were made available
by the State of North Carolina Division of Laboratory
Services. Among the samples were 10 from infants with
normal concentrations of Phe, 8 from infants with increased concentrations of Phe and subsequently confirmed as positive for PKU, and 5 from infants with
initially increased concentrations
of Phe that were normal on follow-up and shown not to have PKU.
In addition, we examined
45 cards from the New
England Regional Newborn Screening Program, of
which
30 were
normal
control
subjects
and 15 were
patient control subjects (other than PKU). The original
screening cards and plasma samples from later hospital
admissions
were also available from one patient with
the oculocutaneous
type of tyrosinemia,
caused by tyro-
sine transaminase
deficiency (tyrosinemia type I, McKusick 276600), and from another with fumarylacetoacetate
hydrolase
deficiency (tyrosinemia
type II,
McKusick 276700).
The first 206 samples from a pilot study involving the
analysis of fresh neonatal samples from North Carolina
by MSIMS were also included as a set of normal controls.
Preparation
Dried
of Samples
blood spots on filter paper were prepared
by
punching out a 6.35-mm (0.25-in.)-diameter circle into a
1-niL vial with a standard paper punch. This corresponds to --11 L of whole blood (9). About 2 nmol each
of [2H3]leucine, [2H5]phenylalanine,
and [2H4]tyrosine
in 0.5 mL of methanol were added to the vial. The
contents were vortex-mixed and allowed to stand for 30
mm at room temperature.
The supernate was transferred to a 1-mL conical vial, evaporated to dryness
under nitrogen, and incubated with 50 1L of 3 mol/L
HC1 in n-butanol at 65#{176}C
for 20 mm in a capped 1-niL
glass vial. The solvent was evaporated under nitrogen,
and the derivatized sample was reconstituted
in 50 pL
of an equivolume mixture of methanol and glycerol.
To assay plasma samples, we added -5 nmol each of
the isotopically labeled internal standards-[2H3]Leu,
[2H5]Phe, and [2H4]Tyr-in
methanol (800 L) to a
100-j.L aliquot of plasma. After vortex-mixing,
we
transferred
the supernate to a 5-niL vial, evaporated the
solvent,
and reconstituted
the residue
in methanol
(2
X
100 ML), transferring
this to a 1-mL vial. The same
procedure
for derivatization and preparation was followed as described above.
The recoveries of Phe and Tyr from blood spots were
determined by standard
addition at three different concentrations (25, 200, and 400 pmol/L), then experimentally measuring the added amounts and quantifying the
results from the standard curves after subtracting the
endogenous
signals.
In these experiments,
we accurately pipetted 12 L of the fortified blood samples onto
the paper and used the entire spots for the analysis.
Mass Spectrometry
We used a VG Quattro
triple-quadrupele
tandem
mass spectrometer with a Lab-base data system (Fisons
Instruments,
Danvers, MA). This computer-controlled
instrument incorporates a cesium ion gun operated at
10 keV, a conventional LSIMS insertion probe, and two
off-axis detectors.
One detector was placed in an intermediate position after the first quadrupele
(Q1) but
before the collision region (also the second quadrupole,
Q2);the other was positioned after the third quadrupole
(Q3). Tuning was optimized by using a solution containing one of the analytical
standards,
2 mmol/L,
deriva-
tized as the butyl ester and dissolved in the LSIMS
matrix. The settings for the ion source were optimized
first, to achieve maximum intensity of the EM + H] ion
at the intermediate
detector, with unit mass resolution
in the first quadrupole.
During the monitoring
of the protonated molecular
ion at the final detector, argon was introduced into the
intermediate
collision cell until the intensity of the
signal decreased by 50%. At this point, the daughter ion
corresponding to EM + H 1021 was brought into focus
and the collision energy was optimized to provide maximum sensitivity. The optimum value for all the amino
acids studied was about 30 eV. The second analyzer (Q3)
was also set to unit mass resolution and all lens voltages
in the instrument
were optimized systematically
to
provide maximum intensity at unit mass resolution for
the daughter ion. These tuning settings were saved and
recalled automatically
by the computer when this type
of analysis was to be performed. In general, the resolution settings and lens voltages were not altered unless
maintenance
in the analyzer region of the instrument
was required. Source tuning and collision gas pressure
were optimized when necessary,
usually once daily,
with use of a tuning solution containing the isotopically
labeled standards for Phe and Tyr at 2 mmol/L each.
Samples were analyzed with the static LSIMS probe
without
further tuning of the instrument.
A blank
solution containing only internal standards
was analyzed occasionally
to ensure the absence of carryover
between samples.
All MSIMS spectra (product and neutral loss scans)
were acquired in the continuum mode, in which every
data point was stored. Sixty consecutive
scans of 1 a
each were accumulated
into a single raw spectrum,
which was then automatically
processed
by five-point
smoothing, baseline subtraction, and centroid calculation to produce the final stored mass spectrum. The
result of this was a mass spectrum with much better
signal-to-noise
ratio and reproducibility
of ion ratios
than the average of 60 mass spectra recorded with use of
the standard real-time centroid calculation algorithm.
To produce the scan for “neutral loss of 102 Da,” we
scanned Q1from mlz 125 to 300 while simultaneously
scanning Q3from m/z 23 to 198. The result was a
spectrum of product ions, mostly corresponding
to EM +
H
102]. For convenience,
the mass scale was
adjusted to show the precursor (EM+ H]) ion masses on
the recorded mass spectra as used later for Figures 3
and 4. The mass spectra shown there and in Figure 1 are
the accumulated raw spectra after smoothing and baseline subtraction (as described above).
For quantitative
analysis for Phe and Tyr, we determined the abundance ratios of the ions corresponding
to
Phe and E2H5]Phe (mlz 222:227) and Tyr and [2HJPyr
(mlz 238:242). These values were obtained directly from
the absolute ion abundances stored afcer processing the
raw mass spectra as described above. The concentrations of Phe and Tyr were then calculated
by reference
to the appropriate standard
curves. These calibration
curves were derived by standard addition of Phe and Tyr
-
-
CLINICAL CHEMISTRY,
Vol.39, No. 1, 1993 67
Phenylalanine
lXI
(-102/
(-102/
136
I
I
Tyrosin.
57
57
100
150
100
200
2H5-Phenylalanine
100
<
150
200
2H4-Tyroslne
242
1.1021
1-102/
57
57
100
150
140
100
(
150
200
1*
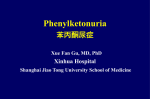
FIg. 1. Product ion mass spectra from the collision-induced dissociation of [M + H] ions of Phe, Tyr, and their stable isotope-labeled
in the tandem mass spectrometer
The most abundant fragment in eachcase corresponds to the lossof 102 Da
to aliquots of a control plasma having fixed concentrations of the internal standards. The ion abundance
ratios (mlz 222:227 and mlz 238:242), corrected for
natural isotopic abundance, were plotted against the
added concentrations of Phe and Tyr, respectively.
Results
Analysis for Amino Acids by MS/MS
As reported previously (8), the butyl ester derivatives
excellent sensitivity and specificity for the
detection of amino acids in blood or plasma by MS/MS.
The fragmentation
of the protonated molecular ions (EM
+ HIl
of the Phe and Tyr butyl esters and of their
isotopically labeled analogs under collision-induced
disprovided
sociation in the tandem mass spectrometer
is shown in
Figure
1. A common loss of the elements
of butyl
formate (102 Da) was observed according to the product
ions at m/z 120 and 136 for Phe and Tyr and at m/z 125
analogs
The aromatic amino acids, Phe and Tyr, have unique
molecular masses and were detected with good sensitivity and selectivity
in blood at physiologically
normal
ranges of concentration.
This is clearly illustrated
in
Figure
3A, which shows the amino acid profile by
MS/MS from a typical sample of normal human plasma.
Signals for several amino acids were clearly discernible.
Signals corresponding
to the isotope-labeled
internal
standards,
[2H3]Leu, E2H5JPhe, and E2HJI’yr, were detected at m/z 191, 227, and 242, respectively.
The
spectrum was essentially
free of interfering
signals
derived from other endogenous compounds in plasma.
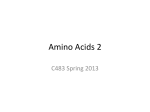
The profile in Figure
3B was from the methanol
extract of a 12-L blood spot from an original neonatal
screening
card corresponding
to one of the control subjects. The profile of amino acids was essentially
the
same as that of the normal plasma
(Figure 3A), and
R
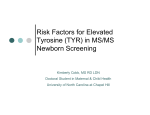
and 140 for [2H5]Phe and E2H4]Tyr, respectively. This
process, shown schematically for Phe and Tyr in Figure
2, involves
the transfer of a proton to generate a resonance-stabilized
carbonium ion, which is apparently
specific to a-amino acids. The loss of 102 Da was not
observed with either fatty acid or acylcarnitine
butyl
esters (data not shown). Other minor fragments were
also observed in the product ion spectra, including a
common ion at m/z 57 derived from the butyl group
(Figure 1).
0
Phe:
Tyr.
A-H
A-OH
CH2
H3i-CH-COOC4H8
A neutral-loss
scan of 102 Da in the MS/MS mode,
whereby
both mass analyzers
are scanned simultaneously with a constant mass difference of 102 Da, generated a spectrum
showing the molecular ions of the
CID
amino acids (as their butyl esters) present in a mixture
(8). The sensitivity for each amino acid varied widely,
H2it-CH-CH2--
HCOOC4H8
A
and some signals were composites
of more than one
amino acid that either shared the same molecular mass
(such as leucine, isoleucine,
and hydroxyproline)
or a
Fig.2. Schematic representation of the specific fragmentationthat
characterizes the amino acid butyl ester derivatives
Loss of the elementsof butyl formate(102 Da) fromthe protonated molecule
occurs under collision-induced dissociation and results in the formation of a
common fragment ion (such as glutamine
resonance-stabilized
68
CLINICALCHEMISTRY,Vol.39, No. 1, 1993
and lysine).
carbonium ion
100
Assay Accuracy
A
I
L
100
nv
B
)
n;1z
Fig.3. MS/MS aminoacid profilesof normalhumanplasma(A) and
a blood spot froma normalneonatalscreeningcard(B) obtained by
applying the ‘neutral loss of 102 Da” scan to the denvatized
methanol extracts
The signals detectedcorrespond to the fragments resulting from the loss of
102 Da from the [M + H1 ion of each amino acid, but for convenience the
mass scale has been adjusted to represent the precursor (protonated molecular) ionmasses.Giyclne (Gly, m/z 132), alanine + sarcoslne (Ala + Sar, m/z
146), senne (Ser, m/z 162), proline + asparagine (Pro + Asn, mhz172), valine
(Val,mhz174),threonine(Thr, mhz 176), glutamine + lysine (Glu + Lys, m/z
186), leucine + isoleucine + hydroxyproline (Leu + lie + Hypro, m/z 188),
methionine (Met, m/z 206), phenylalanlne (Phe, mhz 222), tyroslne (Tyr, mhz
238), aspartic acid (Asp, mhz 246), glutamic acid (Glu, m/z 260), and
tiyptophan(Trp, m/z261)
there was no evidence of interference
from signals not
derived from the amino acids and their added internal
and Precision
The accuracy of this method was previously determined by comparing the individual values for Phe and
Tyr in selected plasma
samples
with those obtained
by a
standard
method involving ion-exchange chromatography (8).
The analytical recoveries of added Phe and Tyr from
blood were determined in triplicate at concentrations of
25, 200, and 400 moI/L.
The respective mean (SD)
values obtained were 98 (7)% and 101 (8)% at 25 tmol/L;
98 (6)% and 93 (6)% at 200 MmoJJL; and 100 (5)% and
102 (6)% at 400 molJL.
The methods of calibration
and analysis
on which
isotope-dilution
MS is based are independent
of the
recovery of analytes from the biological matrix (10,11).
In principle, MS/MS greatly reduces the chance of chemical interference
because of its high molecular specificity, which greatly exceeds that of conventional ultraviolet absorbance
detectors. This is exemplified
by the
lack of interfering signals in the mass spectral profiles
not derived from amino acids (Figure 3, A and B).
Precision of the assay was calculated by replicate
analysis
of the same blood sample by the complete
analytical
procedure for blood spots described in Mate-
Table 1. QuantitatIve Analysis
s-
Cenc by MS/MS, ganottL
Sample
Ph.
Tyr
38 (<242)b
192 (<242)
211
2
45 (<242)
51
4
5
6
38 (<242)
42 (<242)
62 (<242)
48
78
Assay Calibrationand Limitsof Detection
3
51(242)
4
5
224(557)
149 (279)
Phe and Tyr (Table 1).
48
3
standards.
0.99).
The signal-to-noise
ratios for endogenous
signals for
Phe and Tyr in typical blood samples were 50:1 and
20:1, respectively.
The estimated
detection limits-the
signals projected to give a signal-to-noise
ratio of 3:1correspond to concentrations
of 3 and 10 pmoIJL, respectively, well below the physiologically
normal ranges for
Ph.yr
Control group 1a
Controlgroup2”
1
2
We used standard isotope-dilution
assay techniques
(10, 11) to derive calibration curves for the analytes of
interest in human plasma, i.e., standard addition of the
Phe and Tyr over the calibration range of interest with
fixed amounts of the internal standards.
The ratios of
signals corresponding to the analytes and their internal
standards
were plotted as a function of concentration.
The curve for added Phe showed excellent linearity over
the concentration range 2-80 mol/L (r2 = 0.99). For
Tyr, the range of linearity was 10-400 Mmol/L (r2 =
for Phe and Tyr In Blood
150(448)
83(260)
PKU positives
1
2
3
4
5
6
7
0.88
0.80
0.53
70
0.89
93
157
109
1.6
0.53
0.47
220
1.0
75
2.0
166(297)
51
3.3
490 (624)
64
77
61
53
7.7
2.5
67
67
70
307
283
21.6
3.0
8.5
195(242)
237(370)
512(430)
1454(1545)
254 (273)
598 (576)
8
Tyrosinernia 1d
0.80
0.91
37 (n.a.)
3.9
9.7
0.12
Tyrosinemia 1l
142 (n.a.)
0.45
a Selected from 55 normal samples (as assessed by the State Laboratory).
b Results of fluorometric assay used by the State Screening Laboratory
tsted in parentheses.
C False PKUpositives
(as assessedbythe State Laboratory).
dTyne
transaminasedeficiency.
Fumaiylacetoacetate
n.a., not applicable.
hydrolase deficiency.
CLINICALCHEMISTRY,Vol.39, No. 1,
1993
69
These values, representing the within-assay variation, were 6.2% for Phe, 8.4% for Tyr, and
6.6% for the Phe/Tyr ratio (n = 10). The CVs for Phe,
Tyr, and Phe/Tyr ratio determined for the same sample
on different occasions within 1 month, representing the
interassay variation, were 8.8%, 9.7%, and 11.5%, respectively
(n = 8). The absolute concentrations of Phe
and Tyr in this sample were 115 and 85 mo1/L, respectively.
rials and Methods.
100
A
cJ
100
00
Analysisof Original Neonatal Screening Cards
we used 206 fresh samples, from the
State Screening
Laboratory, analyzed
of collection. The samples had already
been analyzed by the State Laboratory
and were considered normal. In this control group, the mean ± SD (and
range) for Phe and Tyr were 55 ± 17 (12-172) mol/L
and 77 ± 30 (29-236) molIL, respectively; the PhelTyr
ratio in each sample was 0.78 ± 0.28(0.21-1.74).
These
Phe and Tyr concentrations compare well with values
from the literature
for neonates:
38-137
and 55-147
junol/L (12). Premature
infants can have Phe and Tyr
valuesof
213 and 420 moIIL, respectively (12).
Figure 4 shows MS/MS analysis of unused blood spots
from a second group of older samples (stored 2 years)
from the State of North Carolina Screening Laboratory
that had been categorized
as either normal (control
group 1), confirmed PKU, or falsely positive (control
group 2). Representative
results from each category,
showing the signals for Phe, Tyr, and their respective
internal standards
are presented in Figure 4A-C. For
comparison, the profile of a patient with tyrosinemia
caused by tyrosine transaminase
deficiency is presented
in Figure 4D. For each profile, both Phe and Tyr were
readily quantified from the ion abundances and the
standard curves. Results are summarized
in Table 1,
including results for 6 of the 55 control samples from
group 1. The mean ± SD concentrations
of Phe and Tyr
in all 55 controls were 85 ± 31 mol/L (range 30-192
tmol/L)
and 135 ± 66 prnol/L (range 46-368 mol/L),
respectively.
For the true PKU positives, the abovenormal Phe values measured by the State Laboratory
with a fluorometric assay were in good agreement with
those determined
by isotope-dilution MS, whereas the
fluorometric
Phe values for the false positives (control
group 2) were more than twice as high as those measured by mass spectrometry
(Table 1).
The Phe/Tyr ratio was calculated
for each sample
(Table 1). For control group 1, the mean ± SD Phe/Tyr
ratio was 0.71 ± 0.22 (range 0.2-1.4, n = 55)-very
similar to that obtained from the analysis of the 206
fresh control samples previously described. For all cases
of PKU, the mean ratio was 7.8 ± 6.5 (range 2.6-22, n =
8); for the false positives in control group 2, it was 1.1 ±
0.67 (range 0.4-2.0, n = 5).
Amino acids were also analyzed from the original
PKU cards that corresponded to two cases of tyrosinemia, retrieved from the State Screening
Laboratory
after a positive diagnosis of tyrosine transarninase deficiency in one case and fuinarylacetoacetate
hydrolase
B
For controls,
North Carolina
within 2 weeks
70 CLINICAL CHEMISTRY, Vol. 39, No. 1, 1993
C
I
C
04
100
D
240
nVz
Fig. 4. Detection of the aromaticamino acids PheandTyr,with their
respective internal standards ([2H5]Phe and [2HJryr), by MS/MSof
extracts from selected neonatalblood spots: (A) normal;(B) classical PKU; (C) falsely positiveby fluorometricassay and normal by
MSMS; (D) tyrosinemladue to tyrosinetransaminase deficiency
The Internal standards enableaccuratequantificationof Phe and Tyr
deficiency in the other, The neonatal tyrosine concentrations were 307 and 283 mol/L,
respectively (controls: 135 ± 66 pmoJ/L, n = 55).
DIscussIon
MS/MS can be a
in neonatal
blood
samples. A larger sampling will be needed to accurately
determine the sensitivity and specificity of the assay.
Samples
are prepared
in batches of 60 by a simple
solvent extraction and derivatization
procedure
that
takes -2.5 h. The total instrument time required for the
These
reliable
results
method
demonstrate
for detecting
that
PKU
analysis of each sample is -2-3 mm. The advantages of
MS/MS over alternative methods of analysis are its high
specificity
and accuracy of quantification through use of
the isotope-dilution
technique, plus its speed and amenability to automation. The lack of chemical interference from other components in the sample matrix is
striking
in view of the simplicity of the method of
sample preparation.
Most of the samples identified as false positives by the
fluorometric
suggesting
assay
that
the
for Phe were normal
fluorometric
assay
by MS/MS,
is subject
to
chemical interference that leads to overestimation
of
the Phe concentration in at least some cases. The MS
data also indicate that the Phe/Tyr ratio is an excellent
discriminant
for PKU-affected and normal cases. We
expect the number of false positives obtained by using
this ratio to be very low. In addition to PKIJ, the new
method might be expected to detect at least some forms
of tyrosinemia in neonates, as indicated by the results
for the two cases presented
here.
Other disorders
of
amino acid metabolism such as the glycinemias, methioninemias,
and maple syrup urine disease should
also be detectable by the same test. When combined
with the acylcarnitine profile test for disorders of fatty
acid and branched-chain amino acid catabolism currently performed
on the same samples in this laboratory, at least 15 metabolic disorders are potentially
detectable from the same blood spot with a single
analysis (13).
The suitability
of a tandem quadrupole mass spectrometer
in the clinical laboratory can be judged by our
experience, in which such an instrument
has been used
routinely in a clinical diagnostic setting for >2 years to
assay acylcarnitines in urine and plasma. During this
time, >5000 patients’ results were obtained. The equipment is compact in size and controlled
by programmed
computer instructions.
It is actually easier and less
troublesome to operate than a gas-chromatographic MS
system, and in our hands downtime has been restricted
to scheduled ion-source cleaning (4 h every 2 weeks) and
maintenance (2 days every 6 months), with breakdowns
accounting for <5 days per year. The instrument
is
operated daily by B.S.-degreed technicians
under the
remote supervision of an experienced mass spectroscopist.
The current sample load of -200 samples per week is
easily handled by manual methods of sample analysis.
Automation of the MS analysis and data processing is
currently under development and will ultimately facilitate large-scale neonatal screening of 400 samples
per day by this method. The capacity for high throughput and accurate, multiple testing combined with miiiimal labor and reagent costs can offset the high capital
cost of the equipment.
We thankS. HAilmanforhis expert technical assistance. Financial support was from NICHD Division of the National Institutes of
Health (Bethesda, MD; grant no. HD-24908) and the State of
North Carolina, Division of Maternal and Child Health, Department of Environmental Health and Natural Resources (Raleigh,
NC; grant no. C-05070). We also thank Harvey Levy of the New
England Regional Newborn Screening Program (Jamaica Plain,
MA) for a set of 45 original Guthrie cards.
References
1. Kirkman kIN, Carroll CL, Moore EG, Matheson MS. Fifteenyear experience with screening for phenylketonuria
with an automated fluorometric method. Am J Hum Genet 1982;34:743-52.
2. Snyderman SE. Newborn metabolic screening: follow-up and
treatment results. In: Carter TP, Wiley AM, eds. Genetic disease:
screening and management. New York: Alan R Lisa, 1986:195.209.
3. Guthrie R. Newborn screening past, present and future. In:
Carter TP, Wiley AM, eds., Genetic disease: screening and management. New York: Alan R Lisa, 1986:319-39.
4. Hoffman GL, Laeasig RH, Hassemer DJ, Makowski ER. Dual
channel continuous-flow
system for determination
of phenylalanine and galactose: application to newborn screening. Clin Chem
1984;30:287-90.
5. McLaffertyFW. Tandem mass spectrometry. Science 1981;214:
280-7.
6. Millington DS, Norwood DL, Kodo N, Roe CR, Inoue F. Application of fast atom bombardment with tandem mass spectrometry
and liquid chromatography/mass
spectrometry
to the analysis of
acylcarnitines in human urine, blood, and tissue. Anal Biochem
1989;180:331-9.
7. Millington DS, Kodo N, Norwood DL, Roe CR. Tandem mass
spectrometry: a new method for acylcarrntine profiling with potential for neonatal screening for inborn errors of metabolism. J Inher
Metab Dis 1990;13:321-4.
8. Millington DS, Kodo N, Terada N, Roe D, Chace DH. The
analysis of diagnostic markers of genetic disorders in human blood
and urine using tandem mass spectrometry with liquid secondary
ion mass spectrometry. hit J Mass Spectrom Ion Processes 1991;
111:211-28.
9. National Committee for Clinical Laboratory
Standards. Blood
collection on filter paper for neonatal programs: approved standard. NCCLS Publication LA4-A. Villanova, PA: NCCJ.S, 1988.
10. Falkner F. Comments on some common aspects of quantitative mass spectrometry. Biomed Mass Spectrom 1981;8:43-6.
11. Markey SF. Quantitative
mass spectrometry. Biomed Mass
Spectrom 1981;8:426-.30.
12. Shapira E, Blitzer MG, Miller JB, Affrick DK. Biochemical
genetics: a laboratory manual. New York: Oxford University
Press, 1989.
13. Millington DS, Terada N, Chace DH, Chen Y-T, Ding J-H,
Kodo N, Roe CR. The role of tandem mass apectrometry in the
diagnosis of fatty acid oxidation disorders. In: Coates PM, Tanaka
K, eds. New developments in fatty acid oxidation. New York:
Wiley-Lisa, 1991:339-54.
CLINICAL CHEMISTRY, Vol.39, No. 1, 1993
71