Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
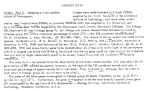
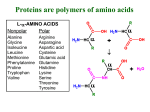
Risk Factors for Elevated Tyrosine (TYR) in MS/MS Newborn Screening Kimberly Cobb, MS RD LDN Doctoral Student in Maternal & Child Health University of North Carolina at Chapel Hill North Carolina Newborn Screening ¢ NC uses tandem mass spectrometry (MS/MS) to screen for >30 disorders ¢ Abnormal TYR considered >300µM (until August 2002) Transient Neonatal Tyrosinemia ¢ Hypertyrosinemia that peaks prior to 14 days and usually resolves by one month ¢ Likely due to decreased activity of 4hydroxyphenylpyruvic acid dioxygenase (4HPPD) ¢ Proposed risk factors: l l l l Prematurity Excessive protein intake Deficient vitamin C intake Combination of above (1) phenylalanine hydroxylase (tetrahydrobiopterin), (2) tyrosine aminotransferase (TAT) (pyridoxine), (3) 4-hydroxyphenylpyruvic acid dioxygenase (4HPPD) (ascorbate, oxygen), (7) & (8) the responsible enzymes have not been identified From The Metabolic & Molecular Bases of Inherited Disease 8 th ed Transient Neonatal Tyrosinemia ¢ Controversy over whether it is benign Lethargy and reduced motor activity in neonates l Corneal opacities l Intellect deficits in later childhood l ¢ No recent studies Changes in feeding practices l Changes in screening technology l Study Aims ¢ Determine risk factors for transient neonatal tyrosinemia. Gender l Race / ethnicity l Type of feeding l Birth weight (prematurity) l Multiple births l Age a specimen collection l Other abnormal NBS labs l Methods ¢ Study Population l ¢ Cases l ¢ All infants screened by MS/MS in North Carolina from August 1, 2001 to July 31, 2002 Infants with abnormal TYR (=300µM) Controls Infants with normal TYR (<300µM) l Matched by laboratory batch of cases l Methods ¢ Descriptive, laboratory and follow-up data was abstracted from the Newborn Screening Database at the NC State Laboratory of Public Health ¢ Logistic regression analysis was used to determine the odds of having abnormal TYR on a initial screen Results Table 1. Summary Statistics Sample Size Gender Male Female Race White Black Ethnicity Non-Hispanic Hispanic Ave Age Tyr Level >500 µmol/L 300-500 µmol/L Tyrosine Cases 482 Controls 861 48% 52% 52% 47% 48% 29% 53% 32% 55% 22% 48 hrs 64% 12% 45 hrs 11% 89% 0% 0% Results Table 2. Summary of Findings Variable Odds Ratio Ethnicity Hispanic 2.21 Birth Weight Low Birth Weight 1.74 Very Low Birth Weight 1.59 Extremely Low Birth Weight 3.49 Feeding Breastfeeding 2.73 Standard Error p-value 95% CI 0.58 0.003 (1.32, 3.71) 0.28 0.45 1.16 0.001 0.101 0.000 (1.26, 2.38) (0.91, 2.75) (1.92, 6.68) 0.48 0.000 (1.94, 3.84) Adjusted for gender, age, transfusion, other abnormal labs, multiple births and death Results ¢ Significant variables Ethnicity l Type of Feeding l Birth Weight l Results ¢ Non-significant variables Gender l Race l Age at screen l Transfusion l Multiple births l Infant Death l Other abnormal labs (T4 / TSH) l Results ¢ Repeat screen requested for all infants with abnormal tyrosine ¢ 5% of repeat samples had TYR >300µM 1 infant with TYR II l Several with liver disease l Others resolved by time of confirmatory testing l Conclusions ¢ Breastfed infants may be catabolic in neonatal period l ¢ TYR elevations due to endogenous sources of protein Birth Weight May be proxy for prematurity l Need gestational age l ¢ Unclear significance of Hispanic ethnicity Changes in TYR Screening ¢ Cut off values for abnormal TYR changed to >500µM in August 2002 l Number of abnormal TYR fell by 75% l No known false negatives Limitations / Future Studies ¢ Type of Feeding l ¢ Relies on self-report Gestational Age / Prematurity Unavailable from NBS records l Linkage to Birth Certificate Data l ¢ Long-term effects of elevated TYR Do they exist? l At what level and duration do they occur? l Implications for dietary treatment l Acknowledgements This study has been made possible through the support of: ¢ Dianne Frazier, PhD MPH RD, Associate Professor of Pediatrics, UNC-CH Department of Pediatrics Division of Genetics and Metabolism ¢ NC State Laboratory of Public Health with special thanks to l Shu Chaing, PhD, Director of Newborn Screening Program l Susan Weavil, MS, Director of Tandem Mass Spectrometry Laboratory