Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
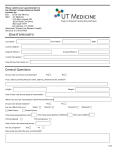
PAST MEDICAL/FAMILY/SOCIAL HISTORY MEDICAL CONDITIONS [ ] Diabetes [ ]Cancer [ ]Asthmas [ ]Chronic Lung Disease [ ]high blood pressure [ ]Tuberculosis [ ] OTHER ____________ PREVIOUS SURGERIES [ ]Heart [ ]Tonsils [ ]Appendix [ ]Gall Bladder [ ]Hysterectomy [ ] OTHER _______________________ FAMILY HISTORY: Any chronic or hereditary illness? Please list all prescription, medications, herbs, vitamins, and over the counter medications ALLERGIES (LIST): MARITAL STATUS _____________ OCCUPATION _________________ LEVEL OF EDUCATION: # OF YEARS COMPLETED _______________ ALCOHOL USE? [ ] NO [ ] YES DRUG USE? [ ] NO [ ] YES SMOKE CIGARETTES? [ ] NO [ ] YES pack(s) per day=_____________ IMMUNIZATIONS: Tetanus booster in last 5 years? [ ] NO [ ] YES Last flu shot ___________________ Date of last pneumovax________________ REVIEW OF SYSTEMS PLEASE CHECK QUESTIONS: [√] No Problem [√] Problems you are having now [√]Other & explain below GENERAL/CONSTITUTIONAL [ ] no problem [ ] fever/chills [ ]poor appetite [ ]tired [ ]other EYES [ ] no problem [ ] discharge [ ]blurred vision [ ]other EARS [ ] no problem [ ]pain [ ]decreased hearing [ ]itching [ ]other NOSE [ ] no problem [ ]pain [ ]drainage hearing [ ]congestion [ ]other THROAT [ ] no problem [ ]pain [ ]hurts to swallow [ ]swelling [ ]other HEART & BLOOD VESSELS [ ] no problem [ ]chest pain [ ]bad circulation [ ]varicose vein [ ]other RESPIRATORY [ ] no problem [ ]cough [ ]difficulty breathing [ ]wheezing [ ]other ESOPHAGUS [ ] no problem [ ]painful swelling [ ]difficulty swallowing [ ]other STOMACH [ ] no problem [ ]heartburn [ ]nausea [ ]vomiting [ ]other INTESTINES, COLON [ ] no problem [ ]pain [ ]constipation [ ]diarrhea [ ]bleeding [ ]other PELVIC [ ] no problem [ ]problems with period [ ]vaginal discharge [ ]sex pain [ ]other URINATION [ ] no problem [ ]painful [ ]blood [ ]frequent [ ]other [ ] hard to get started [ ]loose it with cough or sneeze [ ]weak stream MUSCLES & BONES [ ] no problem [ ]arthritis [ ]neck pain [ ]arm problem [ ]leg problem [ ] other NEUROLOGIC [ ] no problem [ ]headache [ ]weak [ ]memory loss [ ]numb [ ]other SKIN [ ] no problem [ ]rash [ ]color change [ ]abnormal sweating [ ]other BREASTS [ ] no problem [ ]pain [ ]lumps [ ]other PSYCHIATRIC [ ] no problem [ ]depression [ ]anxiety [ ]hallucinations [ ]anger [ ]other ENDOCRINE [ ] no problem [ ]abnormal thirst [ ]cold all the time[ ]hot all of the time [ ]other [ ] abnormal weight loss/gain [ ]abnormal hair loss or gain BLOOD [ ] no problem [ ]anemia [ ]easy bruising [ ]other LYMPH NODES [ ] no problem [ ]painful [ ]swollen [ ]other ALLERGIC, IMMUNOLOGIC [ ] no problem [ ]hives [ ]food allergy [ ]hay fever [ ]other [ ]low resistance to infection EXPLAIN OTHER [ ] Boxes checked and list any other problems you are having NAME:____________________________________________ DATE OF BIRTH________________________ DATE:_____________________________________________ REVIEWED BY:_________________________