Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
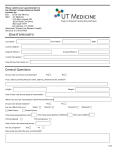
PATIENT MEDICAL HISTORY Date____________ Name ________________________________________ DOB _____________ Age__________ GENERAL MEDICAL INFORMATION Date of last physical exam _____________________ Reason for today’s visit (Chief Complaint)“________________________________” Duration _________________ Location ___________________ Symptoms __________________ Medications____________________________ Allergies to Medications N Y __________________ Reaction? ___________________________ Bad reaction to local anesthesia? NY Reaction? ___________________________ Pregnant, planning a pregnancy or nursing a child? N Y Do you take oral contraceptives? N Y __________ PAST MEDICAL HISTORY None, I am Healthy Do you have artificial joints? Asthma/ Hay fever Do you have a heart murmur? High Blood Pressure Do you have a pacemaker? Heart Attack Do you take antibiotics before a dental procedure? Diabetes HIV/AIDs Hepatitis Skin Cancer: Melanoma, Squamous Cell Carcinoma, Basal Cell Carcinoma Bleeding disorder Surgeries __________________________________________________ No No No No YES YES YES YES MEDICATIONS __________________________ ___________________________ __________________________ _____________________________ __________________________ _____________________________ Aspirin No Coumadin No Plavix No Heparin No Other Blood Thinner YES YES YES YES No YES FAMILY HISTORY Healthy Y/N Health Conditions? If deceased, specify cause & age? Healthy Y/N Father Brothers Mother Sisters Spouse Children SOCIAL HISTORY Occupation _________________ Do you smoke? N Y Health Conditions? If deceased, specify cause & age? Do you drink? N Y Drugs? N Y REVIEW OF SYSTEMS Fever or Chills Ears/Nose/Throat/Mouth Lungs Kidneys Headaches/seizures Endocrine/ hormonal Normal Normal Normal Normal Normal Normal Abnormal Abnormal Abnormal Abnormal Abnormal Abnormal ___________________ ___________________ ___________________ ___________________ ___________________ ___________________ Patient: ________________ Date_______________ Eyes Heart Stomach/bowel Arthritis/muscles/joints Psychological disorder Allergic/ Immunologic Normal Normal Normal Normal Normal Normal Abnormal Abnormal Abnormal Abnormal Abnormal Abnormal _________________ _________________ _________________ _________________ _________________ _________________ Provider__________________ Date_____________