Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
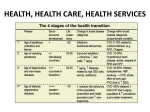
GMT 3: Disease burdens and the risk of new pandemics GMT Description Summary Health is essential for human development. Globally, health standards have improved in recent decades, largely in step with increasing life-spans. However, the risk of exposure to new, emerging and re-emerging diseases, to accidents and new pandemics, is expected to grow with increasing mobility of people and goods, climate change and poverty. Vulnerable Europeans could be severely affected. The exact nature and extent of risks and potential impacts within and outside Europe will depend on a number of factors, such as: the nature and extent of economic growth; government responses to emerging threats; technological advances in health care and disease management; and the inherent ‘wild-card’ nature of potential pandemics. Trend description Overall the World Health Organization (WHO) predicts a decrease in the global burden of communicable diseases to 2020 and 2030 as vaccinations continue and new vaccines are developed (WHO, 2009a). However, the disease burden in developed and developing countries differs markedly, and is also unevenly distributed across populations, varying with gender, social and economic status (Wilkinson and Pickett, 2006). Malnutrition and infectious diseases are dominant in the developing world, while obesity and many non-infectious diseases (cardiovascular and neuro-degenerative diseases, diabetes, respiratory diseases, cancer and mental health) predominate in the developed world (WHO, 2006). At the same time health conditions and outcomes vary significantly between the rich and the poor within countries and regions, and even at the micro-scale between different socio-economic groups living in the same country, particularly in cities (especially in emerging economies). Poverty is increasing rapidly in urban areas and hundreds of millions of people live in poverty in the urban slums of lowand middle-income countries, and their numbers are predicted to increase in coming years (UNFPA 2007). This issue is explored in more detail in GMT2: Living in an urban world. Even though sometimes significant regional, national and sub-national variation exists in the disease burden, the general pattern observed is that as countries develop, infectious diseases become a less significant part of overall ill health and are replaced by non-infectious diseases (Figure 1) often associated with lifestyle, consumption and ageing, and driven by increasing obesity and inactivity (WHO, 2009a). This trend towards an increasing prevalence of non-infectious diseases in developing countries is explored in more detail below, see rise of obesity and non-infectious diseases in developing countries, below. Figure 1: Evolution in human health risks as economies develop (source: WHO, 2004) The ageing of populations may have a mutually reinforcing link with developments in health technology: as populations age, so the demand for novel health technologies is likely to increase, while these technologies can simultaneously facilitate the population living longer. Irrespective of the advances in medical science an older population in Europe, and elsewhere, is expected to mean higher rates of certain diseases, e.g. Alzheimers, Parkinsons, heart disease, cancers and arthritis (UN, 2002). Changes in working, living and travel habits, as well as climate change, alter the disease burden both between and within countries (Arguin et al., 2009). Migration inside and between countries is likewise increasing (Figure 2) which increases opportunities for the spread of new, emerging and reemerging diseases and also increases the risk of new pandemics. These factors may have both direct and indirect impacts in Europe, and are explored in more detail below, see rise of infectious diseases in developed countries, and, increased potential for global pandemics. Important uncertainties exist, including: the growth of resistance to antibiotics and other drugs; the failure to address many tropical diseases (Frew et al., 2009); and how effective efforts to manage migration and control disease may be, partly because of uncertainties in trends and future policies but also because the links between income levels and global pandemics are complex and poorly understood. Further uncertainty exists around the status of the global economy. In an optimistic scenario, improvements in access to health care, drinking water and sanitation will continue, further improving health in what are now the poorest countries of the world. This in turn depends on the absence of widespread conflict. However, in the context of these uncertainties, technology can play an important role in supporting improvements in health status and in spatial monitoring of health patterns, allowing mapping and analyses of geographic patterns of disease trends that were previously overlooked (Bodenhiemer, 2005). Nonetheless, it is likely that global disparities will persist in national capacities to manage some transmissible infectious diseases (WHO, 2009b). Although this GMT3: Disease burdens and the risk of new pandemics is not expected to have direct impacts on Europe’s environment, changing patterns of disease burden globally and potential new pandemics may increase the consumption of novel and existing pharmaceuticals, which could result in an increase in the presence of pharmaceuticals in waste- and drinking-water (Roswell et. al 2003). However, global changes in disease burdens are relevant for European policymaking, particularly by prompting investment in preparedness for increased immigration and the associated risks of emerging diseases and pandemics (Arguin et al., 2009): it is worth investing in prevention globally and at the place of origin of potential migrants to Europe. In addition, environmental changes worldwide are becoming an important a driver of human health (Gilland, 2002). Figure 2: Movements of people: migration and tourism Figure 3: Malaria by 2050 (Source: Rogers and Randolph, 2000; Ahlenius, 2005 Risk of rise of infectious diseases in developed countries Rising global mobility driven by economic factors, environmental change or tourism, provides opportunities for diseases to spread rapidly between regions, countries and populations and may result in the introduction (or re-introduction) of infectious diseases to areas where they had been eradicated, including Europe. Ageing populations and climate change may also increase risks and vulnerability. A convergence of certain factors may lead to the risk of a rise of infectious diseases in developed countries, including in Europe, over coming decades. Migration inside countries in particular in the developing world (usually from rural to urban areas) increases the risk of infectious disease, violence and drug dependence, particularly where the migration leads to chaotic slum development, associated with poverty, overcrowding and poor public services. Densely populated urban areas, may pose an even bigger risk of environmental hazards, crime and disease, especially if they are not well managed (WHO, 2008a). Current population movement dynamics rapidly and effectively link regions of marked health disparity, and these linkages can be associated with risk for importation of drug-resistant infectious diseases, vaccine-preventable diseases, multidrug-resistant Tuberculosis (TB), novel influenza viruses, and dengue virus serotypes. For example, TB has re-emerged to become more common in some developed countries where it had historically been reduced to extreme lows. This increase in the incidence of TB has been linked to migrants from areas of high health inequality. Thus, this increased risk in the developing world, especially associated with rapid and poorly managed urbanisation, when combined with increased global movement of people and goods (see Figure 2), can impact directly on the risk of infectious diseases in Europe. The effectiveness of interventions such as airport screening, travel restrictions and other community mitigation measures remains uncertain (Arguin et al. 2009). The link between migration and the incidence of infectious diseases in migrant populations may become increasingly significant as Europe is projected to require increasing numbers of migrants over coming years due to population decline (and to support an ageing population). At the same time the ageing European population is more vulnerable to both communicable and noncommunicable diseases and to health effects related to climate change (for example heat waves and flooding). For Europe, this increased vulnerability may impose significant costs on health systems, which can compete with costs on environmental protection. Rise of obesity and non-infectious diseases in developing countries Historically malnutrition and infectious diseases are dominant in developing countries, while obesity and many non-infectious diseases are predominant in developed countries. However changing lifestyles and patterns of consumption are driving an increase in obesity and noninfectious diseases in developing countries. In the context of often significant regional, national and sub-national variation in the disease burden, the general pattern is that as countries develop, infectious diseases become a less significant part of overall ill health, replaced by non-infectious diseases (Figure 1) often associated with lifestyle, consumption and ageing, and driven by increasing obesity and inactivity (WHO, 2009a). This is also illustrated in Figure 4 which visualises the ‘risk transition’ where, over time, major risks to health shift from ‘traditional’ risks such as inadequate nutrition, unsafe water and sanitation to ‘modern’ risks such as overweight and obesity. Figure 4: the risk transition (WHO, 2009a) Changes to working, living and travel practices contribute to a changing global disease burden, both between and within countries. As income levels rise and access to more ‘western’ lifestyles and consumption patterns increases, there is a tendency for the amount of calories consumed to increase compared to the amount of calories expended. This is due to a range of factors, but principally is related to the decrease in the levels of physical activity associated with working practices. This in turn significantly reduces the amount of energy expended per day, and is a key contributory factor in the increase in the levels of obesity, and other diseases associated with inactivity, in more developed countries, and among certain socio-economic groups in developing countries. Furthermore, the disease burden associated with smoking is decreasing in developed countries, and increasing in developing countries (WHO 2009a). The rate of smoking is likely to increase to 2030 in developing countries, but could decrease over the longer term due to the effect of government policies. Thus, while development, and the trappings of wealth it can bring, does lead to tangible health benefits, this can be seen as a ‘double edged sword’. Easy access to high protein / high calorie foods, sedentary lifestyles, and the emergence of status competition, can lead to physical and mental health problems: obesity, stress and the erosion of community and traditional values and support networks. The WHO estimates that in 2005 more than 1 billion people worldwide were classed as overweight and more than 300 million were obese, and have predicted that the rates will increase in almost all countries, with 2.3 billion people overweight and 700 million obese by 2015 (WHO, 2006). This issue, which was once considered a problem only in high-income countries, is expected to dramatically increase in low- and middle-income countries, particularly in urban settings. A rise in the medical procedures associated with obesity, such as liposuction and stomach-reduction surgery, may reduce the number of obese people. However this is unlikely to be significant in the context of the levels of obesity predicted for certain countries. Non-infectious diseases such as obesity, heart disease and cancer are expensive to treat, and increasing prevalence of these diseases may result in more expensive public health systems. This may pose a challenge to how healthcare is provided in Europe. Increased potential for global pandemics Increased global mobility of people and goods, including migration within and between countries for economic or environmental reasons and as a result of conflicts, provides opportunities for the spread of diseases and increases the risk of global pandemics. We live in an increasingly globalised and mobile world. People and goods are on the move, within and between countries and global regions for tourism, trade, and migration. Such movement may hasten the spread of pandemics. A pandemic is an epidemic spread over a wide geographical area and affecting many people. While a pandemic may not threaten the survival of humanity, it challenges the prosperity and stability of political institutions and human society. An increasingly globalised economy, changes to working, living and travel habits, as well as migration caused by environmental and economic changes as well as major conflicts are all contributing to a more mobile world. This in turn provides opportunities for the spread of new, emerging and reemerging diseases and the potential for an increased risk of global pandemics. The risk of exposure can be exacerbated through environmental factors causing migrations, through forced migration, disease and conflicts (Figure 2). As shown in Figure 2 and Figure 5, climate change may result in environmental changes and pressures leading to migration, in particular from regions of low and medium development to areas of higher development. The risk of global pandemics is highly uncertain, however preparedness and appropriate planning are important issues for Europe as the repercussions could threaten Europe’s security and create a more unstable world. These threats underline the need for a more holistic view of policy approaches, in particular for addressing global problems. A combination of actions for example tackling: sanitation; health care; economic development; and climate change adaptation are needed to address problems of the poor in the world’s megacities1. Figure 5: Environmental factors and conflicts that may cause migration 1 Definitions of what constitutes a megacity differ, however the UN and WHO refer to megacities as those with 10 million or more inhabitants. See: http://www.unhabitat.org/pmss/listItemDetails.aspx?publicationID=2101 and http://www.who.or.jp/publications/20082010/Megacities_Report_Dec09.pdf. Drivers of: Disease burdens and the risk of pandemics Disease burdens and the risk of new pandemics Social Increased migration and personal mobility, including forced migration (e.g. due to environmental change and/or conflict) are key drivers in changes to the pattern of disease burdens, as well as being a key risk factor for potential global pandemics. Rapid urbanisation in developing countries, especially combined with poor planning and governance, is a driver for an increased risk of infectious diseases (see also economic and political drivers below), which, combined with increased migration / mobility, poses a risk to increase the burden of infectious diseases in developed countries, including in Europe. Changes in attitudes and practices related to consumption, lifestyle and dietary habits, combined with increased availability of cheap, high-calorie foods, are key drivers of increased non-infectious diseases in developing countries, in particular obesity and associated disorders. Existing and increasing social and economic inequality in developing (and developed) countries may drive increased exposure and vulnerability to health risks in certain groups. Technological Improved access to sanitation and clean water, as well as vaccination programmes, in developing countries are key drivers for a reduced burden of infectious diseases. Changes to and improvements in health technologies is a key driver for longer life expectancy, and associated non-infectious medical conditions. Technology (e.g. in the workplace and in personal mobility) is a driver for reducing levels of physical activity, for example due to physical effort being ‘engineered out’ of urban areas, which in turn can lead to increased overweight and obesity (more calories consumed than used). Economic Divergence in economic growth, wealth and poverty distribution within and between countries and regions are key drivers of changing patterns of disease burden. Improved living standards and access to health care (for some) in emerging economies is a driver for an increased burden of non-infectious diseases. As noted under Social drivers, divergent economic conditions and prospects is a key driver of migration, which is a factor in increasing the risk of the spread of infectious diseases, and also of global pandemics. Economic development may contribute to changes in access to technology / personal mobility, driving reduced physical activity in work and leisure time, thus driving a tendency for increased prevalence of obesity and overweight, especially when combined with reduced relative cost of food (often weighted towards high-calorie / low nutrient foods). Economic inequality may also be an important driver for mental health issues, such as stress and depression in developing countries. Environmental Environmental degradation and divergent exposure to environmental hazards between rich and poor are drivers of changing disease burdens. Climate change is a significant driver, for example leading to changes in disease vectors, and being a critical catalyst to large scale migration. The growth of resistance to antibiotics and other drugs, and the failure to address many tropical diseases are also drivers of changing patterns of disease burden. Political Governance and policy can play a key role in health and the patterns of disease burden. For example the implementation of high standards of health care, universal vaccination and disease prevention programmes can have a significant impact on the prevalence of certain diseases, while failure to implement such programmes successfully can equally undermine such results. Poor governance of rapidly expanding urban areas, particularly in developing countries may act as a key driver for increased incidences of infectious diseases, and also an increased risk of them spreading (through increased mobility / migration) to developed countries – including Europe. Equally, well managed urbanisation can minimise these risks. The ability (or otherwise) of border security systems to prevent the spread of disease is an important driver (or buffer) in the potential spread of infectious disease, and may play a role in global pandemics. Healthcare policies that put the cost of healthcare onto individuals are likely to be a driver of increasing healthcare costs and thus increasing health inequalities. Interlinkages to other GMTs GMT3: Disease burdens and the risk of new pandemics is closely linked with the other two social global megatrends, GMT1: Increasing global divergence in population trends, and GMT2: Living in an urban world. As indicated in the trend description above, increased migration and the potential social and health implications caused by poorly managed and rapid urbanisation (particularly in developing countries) can exacerbate the potential for the emergence (or re-emergence) of infectious diseases, as well as potentially leading to the rise and spread of new global pandemics. Ageing populations, particularly in the developed world, including Europe, is a factor in the increased prevalence of the non-infectious disease burden. Other interlinkages include with GMT4: Accelerating technological change: racing into the unknown, and GMT5: Continued economic growth. Technology is increasingly important in health care and the control of disease (e.g. the use of nanotechnologies), but also has the potential to change lifestyles and lead to, for example, an increase in the incidence of non-infectious diseases. Income levels and relative inequality are a key factor in disease burdens, with the general trend observed that as levels of economic wealth increase in a population, the relative burden of disease shifts from infectious to non-infectious. Interlinkages also exist between GMT3: Disease burdens and the risk of new pandemics and environmental megatrends and in particular GMT9: Increasingly severe consequences of climate change. Climate change is a key driver of migration within and between countries, and is also directly impacting on disease vectors as well as the geographic range and seasonality of certain infectious diseases. A link is also seen with GMT10: Increasing environmental pollution load. The degradation of ecosystems will impact directly on health, for example through reduced water quality (and availability) and food production, and also will impact indirectly by impacting on livelihoods, especially in developing countries, which may act as a driver of migration and urbanisation. GMT3: Disease burdens and the risk of new pandemics has interlinkages with: Social • GMT1: Increasing global divergence in population trends • GMT2: Living in an urban world Technological • GMT4: Accelerating technological change: racing into the unknown Economic • GMT5: Continued economic growth? Environmental • GMT9: Increasingly severe consequences of climate change • GMT10: Increasing environmental pollution load References Ahlenius, H. 2005, 'Climate change and malaria, scenario for 2050', UNEP/GRID- Arendal Maps and Graphics Library (http://maps.grida.no/go/graphic/climate-change-and-malaria-scenario-for-2050). Arguin, P., Marano, N., and Freedman, O., 2009, ‘Globally mobile populations and the spread of emerging pathogens’, Emerging Infectious Diseases 15(11) 1713 – 1720. Bodenhiemer, T., 2005, 'High and rising health care costs, part 2: technologic innovation' Annals of Internal Medicine, (142) 11 932–11 937 (http://www.annals.org/content/142/11/932.abstract) accessed 14 August 2012. DRC, 2007, Global migrant origin database, Development Research Centre on Migration, Globalisation and Poverty (http://www.migrationdrc.org/research/typesofmigration/global_migrant_origin_database.html) accessed 14 August 2012. Frew, S., Liu, V., Singer, P., 2009, 'A business plan to help the "global south" in its fight against neglected diseases', Health Affairs 28(6) 1 760–1 773. Gilland, B., 2002, 'World population and food supply: Can food production keep pace with population growth in the next half-century?', Food Policy (27) 47–63. IISS, 2010, Armed conflict database (http://www.iiss.org/publications/armed-conflict-database) accessed 15 August 2012. NIC, 2008, Global Trends 2025— A transformed world, US National Intelligence Council, Washington D.C. (http://www.dni.gov/files/documents/Global Trends_2025 Report.pdf) accessed 14 August 2012. Rogers, D.J. and Randolph, S., 2000, 'The global spread of malaria in a future, warmer world', Science, 8 September 2000, (289–5 485) 1 763–1 766. Rowsell VF, Pang DS, Tsafou F, Voulvoulis N, Removal of steroid estrogens from wastewater using granular activated carbon: comparison between virgin and reactivated carbon, Water Environ Res, 2009, Vol: 81, Pages: 394-400, ISSN: 1061-4303 UNDP, 2010, Human development report 2010, United Nations Development Programme (http://hdr.undp.org/en/media/HDR_2010_EN_Table1.pdf) accessed 15 August 2012. UNFPA, 2007, State of the World Population 2007: Unleashing the potential of urban growth United Nations (UN), 2002, World Population Ageing: 1950-2050 (http://www.un.org/esa/population/publications/worldageing19502050/) accessed 14 August 2012. UNWTO, 2008, Tourism Highlights 2008, United Nations World Tourism Organization, Madrid, Spain. WBGU, 2007, World in transition — climate change as security risk, German Advisory Council on Global Change, Earthscan, London. WHO, 2004, Projections of mortality and burden of disease, 2004–2030, World Health Organization (http://www.who.int/healthinfo/global_burden_disease/projections/en/index.html) accessed 14 August 2012. WHO, 2006, Obesity and overweight, Factsheet No 311, World Health Organization (http://www.who.int/mediacentre/factsheets/fs311/en/) accessed 14 August 2012. WHO, 2008a, Our cities, our health, our future: acting on social determinants for health equity in urban settings— Report to the WHO Commission on Social Determinants of Health from the knowledge network on urban settings, World Health Organization, Kobe. WHO, 2008b, World health report 2008 — primary health care: now more than ever, World Health Organization, Geneva. WHO, 2009a, Global health risks: mortality and burden of disease attributable to selected risks, World Health Organization, Geneva. WHO, 2009b, The European health report 2009: health and health systems, World Health Organization, Geneva Wilkinson, R. and Pickett, K., 2006, 'Health inequality and UK presidency of the EU', The Lancet (367). Links to other analysis http://www.eea.europa.eu/soer/europe-and-the-world/megatrends http://www.eea.europa.eu/soer/europe-and-the-world/megatrends/disease-burdens-and-the-risk Versioning 1st Draft, Owen White 20 August 2012. 2nd Draft, Owen White 31 August 2012.