Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
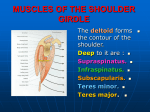
What is the Rotator Cuff Understanding the Shoulder: Injuries and Rehab Concepts Presented by Jennifer Hoffarth, MPT • • • • Supraspinatus Infraspinatus Teres Minor Subscapularis • Biceps not technically part of the RTCbut often implicated and significant cause of anterior shoulder pain Bony Anatomy Humeral head Glenoid fossa Sternoclavicular joint Scapulothoracic joint-scapula lies flush against thoracic spine/ribs • Acromioclavicular joint • • • • 1 Glenohumeral Joint • Where the largest range of motion (ROM) is generated from • Humeral head is large in comparison to glenoid (ice cream cone theory) • Labrum helps stabilize the joint and keep humeral head seated in joint Acromioclavicular Joint • Allows scapula to glide forward/backward and rotate • The AC joint is often a part of shoulder pain – Implicated with ROM over 80-90 degrees Sternoclavicular Joint • Where the sternum and clavicle join • A small disc also is present at this joint • The clavicle needs to elevate and spin posteriorly during normal flexion/elevation of the arm • Motion at this joint needs to be assessed 2 Scapulothoracic Joint • Scapula rides along the thoracic spine • Muscles in this area provide the stability at this joint (trapezius, rhomboids, serratus anterior, levator, etc.) • Weakness of these muscles (proximal weakness) will effect strength at shoulder on down Subacromial Joint • Provided by the acromialclavicular joint and by the ligaments (superior aspect of joint • Inferiorly by the humeral head • Normal subacromial space(714mm) Cervical & Thoracic Spine • Also need to assess these areas • Posture of thoracic spine affects position of the scapula and the position of the humeral head – Humeral head forward – Posture needs to be addressed as part of treatment- especially with the exercises • Thoracic extension is necessary for full elevation of the shoulder as well. – Need to assess for this especially in our older patients. – Movement of thoracic spine all the way to T6 necessary for normal movement of shoulder 3 What Other Muscles Impact the RTC/Shoulder • • • • • • • • Deltoid Pec major and minor Latisimuss dorsi Trapezius Rhomboid major and minor Serratus anterior Levator Teres major Other Areas of Concern • The capsule-helps stabilize the humeral head • Bursa of the shoulder • The labrum Our job is to figure out what is exactly causing the problem! 4 Three Phases of Shoulder Elevation • Phase I—0-60 degrees- increases supraspinatus activity- which compresses humeral head and the subscapularis works to depress the humeral head • Phase II—(motion 60-140 degrees) considered the critical phase-need full ER for this portion – Scapula begins to rotate – Important to have scapular stabilization during this phase Scapulohumeral Rhythm • Phase III—( motion from 140-180 degrees) the soft tissue impacts this portion of motion – Will see if they have “tight” shoulder will “move as one”, usually extends through the thoracic spine to make up for this tightness 2:1 motion 120 degrees comes from humeral head 60 degrees at the scapula 5 What Affects Scapulohumeral Rhythm • Soft tissue flexibility • Poor posture • Proximal or distal muscle weakness • It is not just the movement of the shoulder it is the quality of the movement. It is important to watch them actively elevate or abduct the arm. Look at scapular position with the arms in various positions. Look for winging of the scapula during these movements. Why Does the Shoulder Hurt • The shoulder is the most “moveable” joint in the body. • It is this flexibility/motion that sets the shoulder up for significant problems. • When do we not use our arms? • Poor blood supply to tissues of the shoulder. • Sleeping position often is aggravating to the pain • Our activities throughout our lifetime often catch up with us later in life. • Time spent performing static activities, such as computer work. 6 Examination of the Shoulder • Subjective – – – – What activities cause the pain Where does it hurt When did it start (from injury or over time) When does it hurt • • • • Rest With activity Time of day Does it effect your sleep • How does it hurt – Diffuse – Sharp – Popping – Burning pain – Catching sensation Objective Assessment • Does the patient have a previous history of injury to this shoulder. • Occupation—what does the patient do for a living or what activities does he/she do at home or what sports/leisure activities • Pain level—at rest and with activity • Any neck pain along with the shoulder pain? • AROM-quality and quantity – At what point in motion do they start to experience pain • PROM• Strength Assessment • Scapulohumeral Rhythm – Position of scapula ( 3 positions) • Palpation 7 – Posture--is there anterior translation of the humeral head? – Swelling • Observation – Do they hold the arm at the side – Do they cradle the arm – Do they use it to take there shirt off – Do they have a hard time reaching behind their back – Muscular atrophy – Bony anatomy Palpation • Peripheral Joint Scan—assess briefly the cervical and thoracic spine – Pain in shoulder referred to C4 and C5 dermatomes • C4-look closely at SC/AC joints • C5-common to have pain throughout this dermatome with shoulder pain the more the severe pain may radiate further into the C5 dermatome • • • • AC joint SC joint Spine of the Scapula Greater/Lesser tubercle – Lesser tubercle with ER – Greater tubercle with IR – Coracoid process 8 • Subscapularis Tendon – Arm resting at side, slide lateral off the coracoid and before the bicipital groove—close relation to the biceps tendon • Supraspinatus Tendon – noted in slight extension, max IR and slight abduction • Infraspinatus Tendon – Shoulder flexion to 80 degrees – Slight adduction and ER – Identify spine of scapula and resist ER to know that you are there Special Tests • Distraction/Pull Test – Resisted abduction with arm at side, if painful-• Repeated with distraction force • If worse with distraction-tendonitis • If better with distraction-bursitis Belly Press Test • Hand against lower abdomen – Have patient hold hand to this area as you try to pull them away – If painful implicates the superior fibers the subscapularis 9 Lift Off Sign • Have patient hold there hand against the small of their back or at the sacrum, have them lift just slightly away – If positive implicates the inferior fibers of the subscapularis • Speeds Test • O’Briens Test – Positive if pain greater in IR than with ER and resistance – Deep pain indicates SLAP lesion, superior pain indicates AC joint pathology • Yergasons – Indicates bicipital tendonitis or tear of transverse ligament • AC Shear – Indicates involvement of the AC joint, either arthritic changes or ligament involvement • Hawkins Kennedy – Impingement of supraspinatus • Neer Impingement – Impingement of supraspintus or LHB • Coracoid Impingement – Indicates LHB or subscapularis with medial pain, lateral pain indicates supraspinatus • Sulcus at 0 degrees/90 degrees – Laxity at 0 degrees indicates superior glenohumeral ligament Laxity at 90 degrees indicates inferior glenohumeral complex • Crossover Impingement – – – – Anterior pain—subscapularis or LHB Lateral pain supraspinatus Superior pain AC joint Posterior pain infraspinatus, post. capsule, teres 10 Resistive Tests (learned from IAOM) • ERLS – Have patient hold position as you first let go at wrist then at the elbow • Part one indicates the infraspinatus • Part two indicates the supraspinatus • Positive sign is when there is a drop greater than 5 degrees, • Pain with resisted abduction/ER – supraspinatus • Pain with resisted ER only – Infraspinatus • Pain with resisted IR only – Subscapularis • Pain with resisted Add/ER – Teres minor • Pain with resisted Add/IR – Lat, pec major, teres major Diagonoses We See • Impingement – Acromion types I, II and III – GHJ instability – Scapulothoracic instability/weakness – Shortening of posterior capsule-slides humeral head forward, painful anterior structures • Bursitis – Bursa is densely innervated compared to the other structures – Bursa can be compartmentalized— therefore injections not always helpful 11 • RTC tears – Can be traumatic or occur over times • Small tears vs. large tears • Tendonitis • Selective hypomobilities-restrictions in only one or two directions • Ligamentous Instability – Can lead to nerve damage • Frozen Shoulders/Adhesive Capsulitis – Limitation of ER greater than abduction and IR – Idiopathic usually, typically between 40 and 60 years old, 70% female – More often dominant arm – Not uncommon to one shoulder and later the other – Can take up to 2 years to improve – Freezing, frozen and thawing stages – Can lead to bony lesions – Bankart lesions – Muscle tears – The laxity can lead to impingement as well • Long thoracic—serratus • Suprascapular nerve (supra and infraspinatus) 12 • Tendonitis – Any of the tendons can become inflamed following injury or unknown cause • It is important to differentiate what is causing the pain to allow you to guide your treatment plan. Usually it is more than one structure that is causing the pain. Good assessment will help you better guide your treatment and rehab plans. Treatment Options • Modalities – US – phonophoresis – Iontophoresis – CP – Estim – Use of therapuetic pool • • • • • • • Passive stretching AAROM/AROM Manual techniques to gain ROM Joint mobilization STM Cross Friction massage Self stretching 13 Cross Friction/Self stretch Techniques • Supraspinatus – Transverse friction-arm held slightly behind the back – Self stretch—arm flexed to slightly above/below 90 degrees • Subscapularis – Transverse Friction-supine head of bed or head elevated- inferior to superior – Self stretch • At doorway • With broomstick, arm abducted to 90 degrees, maximal ER with assistance of broomstick or dowel • Infraspinatus – Transverse Friction-on stomach, propped on elbows, one thumb on top of each other, inferior to superior – Self stretch-as noted for supraspinatus-just need to vary position slightly • Biceps – Transverse friction-similar to subscapularis position—make sure thumb is in bicipital groove, passive slight ER, release and repeat – Self stretch—standing-shoulder extension, full pronation, elbow extension- 14 Exercises • Shoulder IR, ER, adduction and extension • Prone over ball or on bed: extension, horizontal abduction, rows, active scaption if tolerated, • Corner “pushout” • Seated chair pushups • Scaption/empty can if done with good form Thank You!! 15