Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Psychopharmacology wikipedia , lookup
Psychedelic therapy wikipedia , lookup
Pharmacognosy wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Neuropharmacology wikipedia , lookup
Drug design wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Prescription drug prices in the United States wikipedia , lookup
Drug discovery wikipedia , lookup
Prescription costs wikipedia , lookup
Drug interaction wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Intravenous therapy wikipedia , lookup
Theralizumab wikipedia , lookup
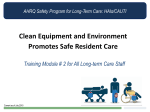
American Nephrology Nurses Association Management of Common Types of Infections in Patients Receiving Chronic Renal Replacement Therapy Sarah Tomasello, PharmD, BCPS Clinical Associate Professor Rutgers, The State University of New Jersey Clinical Specialist – Nephrology Robert Wood Johnson University Hospital New Brunswick, NJ [email protected] Outline of Presentation • Infections in patients on hemodialysis – Risk factors – Common “Bugs and Drugs” – Pharmacokinetic parameters and alterations – Administration and dosing – Monitoring therapy and altering regimen • Catheter related infections • Peritonitis Risk factors for Infection • Weakened immune function – Immunosuppressive agents, uremia • Indwelling catheters – Vascular Access • Catheter > AVG (arteriovenous graft) > AVG (arteriovenous fistula) – Presence as well as manipulation • Dialysis unit exposure – Care givers, patients • Comorbidities – Diabetes (~50%) Issues Related to Hemodialysis • Intermittent clearance – Generally three times a week • Vascular access • Type of filters – “High-Flux” • Filter re-use • Dialysis adequacy – Time on HD – Blood flow rate Common Drugs Used and Why? • Cephalosprins – Cefazolin, ceftazadime, ceftriaxone, • Quinolones – Levofloxacin, ciprofloxacin • Vancomycin • Aminoglycosides? – Gentamicin, tobramycin, amikacin • Long half-life (t ½)in ESRD patients • Can be dosed with/right after hemodialysis What about “The Vancomycin • Glycopeptide • Empiric therapy for gram+ (MRSA) • Concerns – Resistance • 1 gram every week • 1 gram followed by 500mg Q HD Vanco • “Mississippi mud” • Crystalline Degradation Product 1 (CDP1) • Higher trough for resistant organisms or hard to penetrate areaaas • Assays – high performance liquid chromatography (HPLC) – Fluorescence polarization immunoassays (FPIA) Hu et al. Ther Drug Monitor 12 562-569, 1990 Vancomycin Toxicities • • • • “Red Man’s” Syndrome Ototoxicity Nephrotoxicity Increased risk of toxicity with aminoglycoside antibiotics • Thrombocytopenia Rybak et al. Antimicrob Agents Chemother 1999;43:1549-1555 Types of Bacteria Common to dialysis patients bioweb.uwlax.edu/.../whatisbacteria.htm Properties of Dialyzable Drug* • Molecular weight –High-flux may eliminate drugs up to 5000 daltons • Vd – > 1 L/kg not readily dialyzed –Must be water soluble • Protein Binding –Highly protein bound (>96%) not as dialyzable – Watch “narrow therapeutic window” agents – Or saturated plasma proteins (toxicologic emergencies) * May be removed during dialysis Pharmacokinetic Parameters A = Absorption D = Distribution M = Metabolism E = Elimination/Excretion Alterations in Kidney Dysfunction Absorption and Bioavailability • DECREASED – Altered GI emptying (diabetes) – Altered pH (H2 antagonists, proton pump – Edema of GI tract (fluid overload) inhibitors, antacids) – Drug Interactions (antacids, iron, etc…) • INCREASED – Decreased first pass effect – Decreased metabolism by uremic toxins – Decreased enzymatic activity in kidney, liver, GI tract Volume of Distribution (Vd) • Plasma Protein Binding – Albumin is major plasma protein – Acidic drugs bind to albumin • Phenytoin, valproic acid, salicylates – Changes in albumin effect Vd • Alterations in binding sites Increased free concentrations (more effect?) vs Increased rate of clearance? (excreted more rapidly?) Volume of Distribution Plasma Protein Binding (cont.) • Alpha-1-acid glycoprotein (AAG) – Binds basic drugs – AAG up-regulated in kidney disease – “Expect” a decreased free-fraction • This has not been observed in vitro studies Causes of Hypoalbuminemia • • • • Malnutrition Nephrotic syndrome Liver disease Accumulation of competitive inhibitors – Uremic toxins – Metabolites (Normal serum albumin concentration ~4g/dL) Clinical Significance of Changes in Volume of Distribution: WATER • Increased fluid volume – Interdialytic weight gain – Effects drug “peak”concentration • Rapid fluid removal, – Redistribution (re-equilibrium) – Affects therapeutic drug monitoring (TDM) in serum Hemodialyzer • Selectively permeable membrane • Solute (drug) molecules pass through “selectively” based on MW and size • Composed of many types of fibers • Blood flows through 5000-20,000 hollow fibers • Dialysate flows on outside of fibers Hemodialysis System Hollow Fiber Dialyzer Definitions • Diffusion- passive movement of particles from high concentration to low concentration. Limited by filter. • Ultrafiltration- Removal of plasma water by a procedure • Convection- movement of particles with movement of water in which they are dissolved. Due to ultrafiltration, also limited by filter MW of Common Drugs • • • • • Digoxin: 781 Daltons Vancomycin: 1,486 Daltons Gentamicin: 149 Daltons Cefazolin: 477 Daltons Erythropoietin: 30,400 Daltons Molecular Weight High Flux Dialyzer Blood Dialysate MW cutoff < 5,000 daltons (up to 20,000?) Protein Binding albumin albumin albumin Blood = Drug Dialysate Protein Binding Normal Uremia albumin albumin albumin albumin albumin albumin albumin albumin albumin albumin albumin =Drug albumin Competitive inhibitors “uremic slime” Volume of Distribution Tissue Compartment Plasma Compartment Renal Elimination Or Dialysis Optimizing Therapy • Altering dose and dosing interval depends on efficacy and toxicity parameters – Peak effect for efficacy • aminoglycosides – Trough effect for efficacy/toxicity • digoxin, antiepileptics, aminoglycosides – Steady state for efficacy • antihypertensive agents • beta-lactam antibiotics GFR nl GFR Drug Concentration Continuous Infusion hours Steady State 24 48 72 96 120 144 kidney dysfunction Drug Concentration Accumulation at same dose and dosing interval Normal function Trough hours 24 48 72 96 120 144 Lower dose, same dosing interval Normal kidney function Decreased kidney function Drug Concentration Max effective dose Trough hours 24 48 72 96 120 144 Same dose, normal kidney function Extended interval in altered renal function Drug Concentration Max effective dose Trough Time (hrs) TIME Dependent Killing Example: Vancomycin HD TIW, MWF 80 M a x i m u m T h e r a p e u t i c C o n c e n t r a t i o n ( M T C ) 70 mcg/mL 60 50 40 30 20 10 Minimum 0 1st Dose MON tu WED Inhibitory th FRI sa Concentration su MON tu (MIC) WED th X factor FRI sa su Concentration Dependent Killing This is the dosing regimen we were trying to emulate. Matsuo et al. "Administration of Aminoglycosides to Hemodialysis Patients Immediately before Dialysis: a New Dosing Modality." Antimicrobial Agents and Chemotherapy 41.12 (1997): 2597-601. Print. Dosing Tobramycin “Pre-HD” 14 12 280mg ppst HD Drug Concentration 10 8 240 mg Pre HD 310mg post HD 6 4 310mg Pre HD 2 0 1-Sep 2-Sep 3-Sep 4-Sep 5-Sep 6-Sep 7-Sep 8-Sep 9-Sep 10-Sep 11-Sep Tobramycin Course Date Time Dose Comment 9/2 12:00 am 90 mg IVPB 1 mg/kg (4:30pm) 9/3 12:00 pm 240 mg IVPB Pre HD 9/5 5:00 am 310 mg IVPB Pre HD 9/8 12:00 pm 310 mg IVPB Post HD *9/12 11:00 am 280 mg IVPB Post HD *Dose was held on 9/10 Drug Dosing for Hemodialysis • Use recommendations from literature* – Dose for CrCl < 10-15 ml/min on HD – IV IDEALLY given TIW during/after HD – Supplemental dose post-HD if needed • Daily Dialysis – Very little literature (use professional judgment) • MONITOR – Subjective and objective efficacy and toxicity – Therapeutic drug monitoring if available (and PK calculations) *See previous slides 30-32 Drug Levels in HD (Dialyzable) Cpeak Cpre-HD K off HD Conc Next Dose ctrough Pre HD HD End HD Time Redistribution Phenomenon Koff HD Conc Pre HD HD Time End HD POINTS TO REMEMBER • MONITOR!!! – Therapeutic drug levels (if appropriate) • MUST be taken at the proper times – Subjective and objective signs of efficacy and toxicity – Watch for idiosyncratic or “expected” adverse drug events Risk factors for Infection in Peritoneal Dialysis • • • • Patient technique Provider technique Immunocompetence Cormorbid disease states Peritonitis • Incidence – 1 episode for every 12-24 patient months • Signs and Symptoms – – – – – Cloudy drainage Abdominal pain Fever Nausea/vomiting Fever > 37ºC • Diagnostic criteria – Dialysate WBC count > 100/mm3 (> 50% PMNs) – Organism on culture? Drug Regimens to Treat Peritonitis • Several review articles on drug delivery using intraperitoneal route (IP) – Watch for compatibility issues* • Use International Society of PD Guidelines for the treatment of PD related peritonitis** • Use primary literature *Intraperitoneal administration of drugs in peritoneal dialysis patients: A review of compatibility and guidance for clinical use peritoneal dialysis international 2009;29:5–15 .**International ad hoc committee on peritoneal dialysis related infections. International society for peritoneal dialysis - guidelines for the treatment of peritonitis in adults. Peritoneal dial int 2005;25:107131. Treatment of Peritonitis • • • • Give intraperitoneally (IP) if possible Empiric therapy Cover both gram positive and negative Combination first and third generation cephalosporin – Cefazolin and ceftazidime • Narrow coverage based on culture report – not always cultured • Complications – Fibrosis and scarring Peritoneal Dialysis Catheter Infections • Incidence – Once per 1-2 patient years • Organisms – staph aureus, staph epi, pseudomonas • Prophylaxis for nasal carriers of Staphylococcus aureus? – rifampin 300 mg BID x 5 days every three months – intranasal mupiricin BID x 5 days every month – exit-site mupiricin topically every day PD Dialyzability Factors Inflamed peritoneum during infection Blood flow - may affect drug transfer Dwell time Residual renal function Dialysate dextrose concentration- increase causes more ultrafiltration • Generally, high drug absorption but low drug clearance for PD • • • • • Dosing Drugs for Patients on PD • Molecular size- not as important as HD, increased permeability • PB- highly PB not removed • Vd- Increased Vd means less removed, more absorbed into the body • Water solubility- required for removal • Ionization- highly ionized neither absorbed or removed Common Agents to Treat Peritonitis • Tables from ISPD guidelines 2005 update Issues Related to IP Administration • Patient education • Compatibility • Clearance – Increased peritoneal membrane permeability during acute infection – Decreased permeability with fibrosis and sclerosis secondary to infection and inflammation Catheter-Related Bacteremia (CRB) • “Biofilm infection” • Catheter removal creates a requirement for the use of temporary catheters and risk of their associated complications – Multiple procedures, hospitalization period, increased costs – Loss of central venous entry site • Dialysis patients must continue to receive dialysis treatments, therefore, catheter removal is not a feasible option Beathard GA et. al. Infection associated with tunneled hemodialysis catheters. Sem Dial. 2008; 21(6):528-538 50 Incidence of CRB • Rate is less than uncuffed catheters – Tunneled catheters: 1.6-5.5 episodes/1000 days – Uncuffed cathers: 3.8-6.6 episodes/1000 days • Morbidity and mortality due to metastatic infections: 3.2%-50% Beathard, et al. Infection associated with tunneled hemodialysis catheters. Sem Dial. 2008; 21 (6):528-538 51 Pathogenesis • >99.9% bacteria grow as aggregated “sessile communities” attached to surfaces • Hallmark of biofilm-related infections: resistance to anti-microbials and host defenses • Develop in steps: 1. Microbial attachment to the catheter surface 2. Adhesion, growth and aggregation of cells into microcolonies 3. Maturation and dissemination of progeny cells for new colony formation Beathard, et al. Infection associated with tunneled hemodialysis catheters. Sem Dial. 2008; 21 (6):528-538 52 Risk factors • Skin and nasal colonization with staphylococcus • Catheter hub colonization • Prolonged duration of usage • Thrombosis • History of previous CRB • Frequency of catheter manipulation • Diabetes mellitus • Iron over-load • immunocompromised Beathard , et al. Infection associated with tunneled hemodialysis catheters. Sem Dial. 2008; 21 (6):528-538. 53 Prophylaxis of CRB Local antiseptic application Catheter placement Systemic prophylactic antibiotics Aspirin Exit-site infection Daily catheter site care Cleansing site Bandage covering site “Lock” solutions Beathard, et al. Infection associated with tunneled hemodialysis catheters. Sem Dial. 2008; 21 (6):528-538. 54 Diagnosis • • • • + blood culture No other apparent source of infection Symptomatic patient Isolation of the same organism from a semiquantitative culture of the catheter tip (>15 colony-forming units) National Kidney Foundation: KDOQI Clinical Practice Guidelines and Clinical Practice Recommendations for Vascular Access. Am J Kidney Dis 2006; 48: S176-322. 55 Clinical pearls s. aureus, pseudomonas or candida species Remove catheter Other gram- or coagulase- staph. organisms adjunctive antibiotic lock therapy for 3 weeks AND/OR guidewire catheter exchange Catheter locks to be used WITH systemic antimicrobial therapy instill post HD, dwell until next HD, aspirate, instill fresh lock post HD repeat TIW with HD Treat for 7-14 days Mermel, et al. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 update by the Infectious Diseases Society of America. Clin Inf Dis. 2009; 49:1-45. 56 Exit Site Infections • Redness, crusting, and/or exudate • NO systemic symptoms • Negative blood cultures 1. Apply topical antibiotics 2. If tunnel drainage - intravenous antibiotics 3. No response - remove the catheter. National Kidney Foundation: KDOQI Clinical Practice Guidelines and Clinical Practice Recommendations for Vascular Access. Am J Kidney Dis 2006; 48: S176-322. 57 Treatment CRB • Intravenous antibiotics • Remove the catheter – – • Stable, asymptomatic – – • Symptomatic >36 hours Patient is unstable. Change catheter over a guidewire Minimum of 3 weeks of systemic antibiotic therapy New permanent access – – Placed AFTER course of antibiotics AND Blood cultures, have been negative for at least 48 hours National Kidney Foundation: KDOQI Clinical Practice Guidelines and Clinical Practice Recommendations for Vascular Access. Am J Kidney Dis 2006; 48: S176-322. 58 Empiric Treatment • Cefazollin OR vancomycin plus gram-negative rod coverage (Vancomycin plus gentamicin) • Vancomycin: 20 mg/kg loading dose, then 500 mg each subsequent dialysis session • Gentamicin (or tobramycin): 1mg/kg, not to exceed 100mg after each dialysis session • Ceftazidime: 1g IV after each dialysis session “Cath lock” • Concentrated antibiotic solution with/without anticoagulant agent. Dwelled in lumen of the dialysis catheter at the end of each dialysis session until the beginning of next session • Goal: sterilize the catheter biofilm while salvaging the catheter • Antibiotic concentrations must be 100-1000 times greater to kill sessile bacteria within a biofilm Mermel LA, Allon M, Bouza E, et al. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 update by the Infectious Diseases Society of America. Clin Inf Dis. 2009; 49:1-45. 60 Antibiotic lock solutions • Success rate – 87%–100% gram-negative pathogens – 75%– 84% Staphylococcus epidermidis – 40%–55% for hemodialysis-associated CRBSI due to S. aureus • Clinical success of salvaging the catheter and eradicating CRB depends upon the bacterial pathogen involved Mermel LA, Allon M, Bouza E, et al. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 update by the Infectious Diseases Society of America. Clin Inf Dis. 2009; 49:1-45. 61 Examples of Cath-Lock Formulas 1. Gentamicin 5mg/ml and heparin 5000 U/mL 2. Cefazolin 10 mg/ml + gentamicin 5 mg/ml+ heparin 1000 U/ml kim 3. Vancomycin 25mg/mL+gentamicin sulphate 40mg/mL +heparin 5000 U/mL (al) 4. Cefotaxime (10mg/ml) and heparin 5000 U/mL 1. McIntyre CW, et al. Kidney International. 2004; 66:801-805. 2.Kim SH, et al. Kidney International 2006; 69:161-164. 3. Al-Hwiesh AK. Saudi J Kidney Dis Transplant. 2008; 19(4):593-602. 4. Saxena AK, Panhotra BR, Sundaram DS, et al. Nephrology. 2006; 11:299-305. Administration of an antibiotic lock Image derived from: Allon M. Current management of vascular access. Clin J Am Soc Nephrol. 2007; 2:786-800. 63 QUESTIONS?