Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Thesis for doctoral degree (Ph.D.)
2012
Pleiotropic Effects of HMG-CoA
Reductase Inhibitors
Thesis for doctoral degree (Ph.D.) 2012
– studies in vitro and in vivo
Pleiotropic Effects of HMG-CoA Reductase Inhibitors –studies in vitro and in vivo
Cristine Skogastierna
Cristine Skogastierna
From the Department of Laboratory Medicine, Division of Clinical
Pharmacology Karolinska Institutet, Stockholm, Sweden
PLEIOTROPIC EFFECTS OF
HMG-COA REDUCTASE
INHIBITORS
– STUDIES IN VITRO AND IN VIVO
Cristine Skogastierna
Stockholm 2012
All previously published papers were reproduced with permission from the publisher.
Published by Karolinska Institutet. Printed by US-AB
© Cristine Skogastierna, 2012
ISBN 978-91-7457-818-8
Live as you were to die tomorrow.
Learn as if you were to live forever.
- Mahatma Gandhi
ABSTRACT
Cardiovascular disease (CVD) is the prime cause of death in industrialized countries,
resulting from the progression of atherosclerotic lesions. An increased level of plasma
cholesterol, particularly within low-density lipoproteins, is a principle risk factor, but
also elevated triglycerides and low levels of high-density lipoprotein cholesterol.
Recognition of dyslipidemia as a risk factor for CVD has led to an international
consensus that anti-hyperlipidemic drug therapy is essential for the primary and
secondary prevention in risk patients. HMG-CoA reductase inhibitors, i.e. statins, are
the most common drugs used for this purpose, inhibiting the rate-limiting step in
cholesterol biosynthesis. The medical significance of HMG-CoA reductase inhibitors
have in recent years been expanded to include cholesterol-independent or "pleiotropic"
vascular effects, including improvement of vascular endothelial function, inhibition of
vascular smooth muscle cell proliferation and migration, anti-inflammatory actions,
anti-oxidative effects or stabilization of vulnerable plaques. These effects have potential
in the treatment of coronary artery disease in various settings, such as prevention of its
onset as well as its progression. The major aim of this thesis was to contribute to the
general knowledge about the pleiotropic effects of statins, particularly in relation to the
vascular endothelium and to carcinogenesis.
We found that fluvastatin at clinically relevant doses up-regulates transcription and
translation of prostacyclin synthase and endothelial nitric oxide synthase in human
vascular endothelial cells, associated with an increase in cellular production of
prostacyclin (PGI2) and nitric oxide (NO), and induces rapid dilatation in isolated
human arteries via contribution of endothelium derived factors like NO and PGI2.
These results suggest beneficial effects of fluvastatin on endothelial maintenance in
vivo and a protective role on the cardiovascular system, particularly at the level of
vascular endothelium. We also show that simvastatin induces a potentially negative
alteration of vascular endothelial cells both in vivo and in vitro. Exposure of clinically
comparable concentrations of simvastatin led to decreased production and release of
PGI2 in endothelial cells and to significantly increased urinary thromboxane A2 (TXA2)
levels in healthy volunteers, possibly resulting in a shift of the balance between PGI2
and TXA2, favoring the thromboxane pathway. Fluvastatin and simvastatin were also
shown to have different impact on vascular endothelial oxidative stress status, both in
cultivated endothelial cells and in healthy volunteers. Compared to simvastatin,
fluvastatin seems beneficial both regarding expression of anti-oxidative stress enzymes
and reactive oxygen species activity in vitro and anti-oxidative capacity in vivo. The
suggested anti-carcinogenic properties of statins in relation to expression of the redoxactive enzymes thioredoxin reductases (TrxR) were investigated in paper IV. We found
that statin treatment decreases the hepatic expression of TrxR1 in humans and rats. In
addition, the decreased TrxR1-levels were correlated with inhibited carcinogenesis in
rat liver. The effect on TrxR1 levels might explain some of the anti-carcinogenic effects
of statins.
Overall, our results add to the conjecture that the impact on production of vascular
active substances may be significantly different among the statins, and thus the
consequences of statin exposure may not be drug class related but rather compound
specific, highlighting the importance of more comparative studies where several statins
are included. These findings add novel insight in the field of pleiotropic effects of
statins and provide some insight for functional differences among statins.
LIST OF PUBLICATIONS
This thesis is based on the following publications, which will be referred to by their
Roman numerals as indicated below:
I.
II.
Skogastierna C, Luksha L, Kublickiene K, Eliasson E, Rane A, Ekström L.
Beneficial vasoactive endothelial effects of fluvastatin: focus on prostacyclin
and nitric oxide. Heart Vessels. 2011 Nov;26(6):628-36.
Skogastierna C, Björkhem-Bergman L, Bergman P, Eliasson E, Rane A,
Ekström L. Influence of simvastatin on the thromboxane and prostacyclin
pathways, in vitro and in vivo. Accepted in Journal of Cardiovascular
Pharmacology 2012.
III.
Skogastierna C, Björkhem Bergman L, Rane A, Ekström L. Anti-oxidative
effects of statins on vascular endothelium. Manuscript.
IV.
Skogastierna C*, Johansson M*, Parini P, Eriksson M, Eriksson LC,
Ekström L, Björkhem-Bergman L. Statins inhibit expression of thioredoxin
reductase 1 in rat and human liver and reduce tumour development. Biochem
Biophys Res Commun. 2012 Jan 20;417(3):1046-51.
*Equal contribution
ADDITIONAL PUBLICATIONS
Garevik N, Skogastierna C, Rane A, Ekstrom L. Single dose testosterone
increases total cholesterol levels and induces the expression of HMG CoA
Reductase. Subst Abuse Treat Prev Policy. 2012 Mar 20;7(1):12.
Bogason A, Masquelier M, Lafolie P, Skogastierna C, Paul C, Gruber A,
Vitols S. Daunorubicin metabolism in leukemic cells isolated from patients
with acute myeloid leukemia. Drug Metab Lett. 2010 Dec;4(4):228-32.
Aomori T, Yamamoto K, Oguchi-Katayama A, Kawai Y, Ishidao T, Mitani Y,
Kogo Y, Lezhava A, Fujita Y, Obayashi K, Nakamura K, Kohnke H,
Wadelius M, Ekström L, Skogastierna C, Rane A, Kurabayashi M,
Murakami M, Cizdziel PE, Hayashizaki Y, Horiuchi R. Rapid singlenucleotide polymorphism detection of cytochrome P450 (CYP2C9) and
vitamin K epoxide reductase (VKORC1) genes for the warfarin dose
adjustment by the SMart-amplification process version 2. Clin Chem. 2009
Apr;55(4):804-12.
Olsson M, Gustafsson O, Skogastierna C, Tolf A, Rietz BD, Morfin R, Rane
A, Ekström L. Regulation and expression of human CYP7B1 in prostate:
overexpression of CYP7B1 during progression of prostatic adenocarcinoma.
Prostate. 2007 Sep 15;67(13):1439-46.
CONTENTS
1
2
3
4
5
Populärvetenskaplig sammanfattning ................................................................ 1
Introduction ........................................................................................................ 3
2.1 The history of statins ................................................................................ 3
2.2 Cholesterol ................................................................................................ 5
2.2.1 Biosynthesis of cholesterol .......................................................... 5
2.2.2 Cholesterol and cardiovascular disease ....................................... 7
2.3 Pharmacology of statins ........................................................................... 8
2.3.1 Function and molecular properties .............................................. 8
2.3.2 Pharmacokinetics ....................................................................... 12
2.3.3 Clinical applications ................................................................... 12
2.4 Pleiotropic effects of statins ................................................................... 15
2.4.1 Definition.................................................................................... 15
2.4.2 Statins and the vascular endothelium ........................................ 15
2.4.3 Prostanoids ................................................................................. 20
2.4.4 Nitric Oxide ................................................................................ 24
Aims.................................................................................................................. 25
Methodological considerations ........................................................................ 26
4.1 Experimental systems ............................................................................. 26
4.1.1 Cell culture systems ................................................................... 26
4.2 Study subjects ......................................................................................... 27
4.2.1 Human ........................................................................................ 27
4.2.2 Animals ...................................................................................... 27
4.3 Experimental methods ............................................................................ 28
4.3.1 Quantitative real time PCR ........................................................ 28
4.3.2 Promoter studies ......................................................................... 28
4.3.3 Enzyme Immunoassay ............................................................... 31
4.3.4 Western Blotting ........................................................................ 33
4.3.5 Colorimetric assay – detection of NO production..................... 34
4.3.6 LC-MS/MS ................................................................................. 34
4.3.7 Myographic readings ................................................................. 35
Results and discussion...................................................................................... 36
5.1 General comments .................................................................................. 36
5.2 Paper I: Beneficial vasoactive endothelial effects of fluvastatin: ..............
focus on prostacyclin and nitric oxide ................................................... 37
5.3 Paper II: Influence of simvastatin on the thromboxane and .....................
prostacyclin pathways, in vitro and in vivo ........................................... 38
5.4 Paper III: Anti-oxidative effects of statins on vascular endothelium ... 39
5.5 Paper IV: Statins inhibit expression of thioredoxin reductase 1 in ...........
rat and human liver and reduce tumour development ........................... 40
5.6 Undisclosed and unpublished results ..................................................... 41
5.6.1 Atorvastatin and rosuvastatin vs. expression of COX, PGIS .......
and eNOS ................................................................................... 41
5.6.2 Atorvastatin and rosuvastatin vs. PTGIS promoter activity ..... 42
5.6.3
6
7
8
Atorvastatin and rosuvastatin vs. anti-oxidative stress ................
enzyme genes.............................................................................. 43
Conclusions....................................................................................................... 45
Acknowledgements .......................................................................................... 46
References......................................................................................................... 48
LIST OF ABBREVIATIONS
CYP
PGI2
TXA2
PCR
HMG-CoA
HMGR
CVD
MI
ROS
AA
TXA2
PGIS
NO
eNOS
EC
HUVEC
HAEC
PTGIS
PGE2
TXB2
EIA
NE
L-NAME
Indo
COX
TXAS
CYP
IL
TNFα
TrxR
Cat
SOD
GPx
LDL
ADR
Cytochrome P450
Prostacyclin
Thromboxane A2
Polymerase chain reaction
3-hydroxy-3-methylglutaryl-CoA
HMG-CoA reductase
Cardiovascular disease
Myocardial infarction
Reactive oxygen species
Arachidonic acid
Thromboxane A2
Prostacyclin synthase (enzyme)
Nitric oxide
Endothelial nitric oxide synthase
Endothelial cell
Human umbilical vein endothelial cell
Human aortic endothelial cell
Prostacyclin synthase (gene)
Prostaglandin E2
Thromboxane B2
Enzyme immunoassay
Norepinephrine
L-nitro-arginine methyl ester
Indomethacin
Cyclooxygenase
Thromboxane synthase
Cytochrome P450
Interleukin
Tumour necrosis factor α.
Thioredoxin reductase
Catalase
Superoxid dismutase
Glutathion peroxidase
Low density lipoprotein
Adverse drug reaction
1 POPULÄRVETENSKAPLIG SAMMANFATTNING
Kardiovaskulära sjukdomar är den främsta orsaken till för tidig död i västvärlden.
Förhöjda och/eller obalanserade nivåer av blodfetter är viktiga riskfaktorer för
utvecklandet av sjukdomar i hjärta och kärl, till exempel åderförkalkning (ateroskleros),
som leder till förtjockning och minskad rörlighet av kärlväggarna. Den vanligaste typen
av läkemedel för att behandla eller förhindra återkommande symtom är HMG-CoA
reduktas hämmare, de som vi i vardagligt tal kallar för statiner. Utvecklingen av statiner
för att minska konsekvenserna av aterosklerotiska kärlsjukdomar, främst hjärtinfarkt, är
ett av de största medicinska framstegen de senaste decennierna. Många hjärt-kärl sjuka
får positiva effekter av statiner utöver den primära effekten gällande korrektion av
lipidnivåerna. Syftet med denna avhandling var att utöka kunskapen om hur några av
de vanligaste statinerna interagerar med blodkärlens innersta celler, det vaskulära
endotelet, och dess produktion av ämnen som har betydels för kärlens funktion samt
hur statiner kan motverka cancerutveckling.
Kväveoxid och prostacyklin är viktiga substanser som vidgar kärlen och bidrar till ett
hälsosamt vaskulärt endotel. Vi visar i delarbete I att fluvastatin påverkar metabolismen
av dessa substanser positivt och att deras bildande i humana kärlendotelceller ökar. Vi
visar också att fluvastatin akut påverkar blodkärlens förmåga att vidga sig. Detta
betyder att fluvastatinbehandling kan ge visst skydd för kärlväggen både akut genom att
minska vaskulär tonus och över längre tid genom att bromsa
åderförkalkningsprocessen.
I delarbete II studerade vi hur en annan vanlig statin, simvastatin, påverkar bildning och
balans av två av de viktigaste ämnena för endotelfunktion i cirkulationen, prostacyklin
och tromboxan A2. Dessa två ämnen är funktionella antagonister, det vill säga de har
motsatt funktion och måste vara i balans. Vi fann att hos friska frivilliga
försökspersoner minskades utsöndringen av en viktig prostacyklinnedbrytningsprodukt
medan tromboxan A2-utsöndringen höjdes efter simvastatinintag. I isolerade vaskulära
endotelceller som behandlades med simvastatin, minskade produktionen av
prostacyklin med så mycket som 40 %. Resultaten indikerar att simvastatin rubbar den
viktiga jämvikten mellan tromboxan A2 och prostacyklin till fördel för tromboxan A2,
vilket kan ha negativ inverkan på den vaskulära hälsan.
Oxidativ stress och kronisk inflammation i kärlväggarna är ett kännetecken för
kardiovaskulär sjukdom. Syftet med delarbete III var att jämföra de två statiner som
studerats i delarbete I och II i relation till oxidativ stresspåverkan. Studiens resultat
visar att fluvastatin verkar vara mer fördelaktig än simvastatin, då simvastatin
hämmade genuttrycket av flera försvarsenzymer i endotelceller. Försök på friska
försökspersoner visade att de som fått fluvastatin hade bättre försvar mot oxidativ
stress. Dessa resultat tyder på att statinernas effekt kan vara ämnesspecifika och kan
påverka den oxidativa stresstatusen i vaskulärt endotel.
1
C. Skogastierna
I delarbete IV undersöktes mekanismerna bakom statiners anticarcinogena effekter i
leverceller. Thioredoxin reduktaser är proteiner som har stor betydelse för
cancerutveckling och har vistats vara förhöjda i celler med onormal tillväxt.
Statinbehandling visades minska levercellsuttrycket av thioredoxin reduktas 1 i
människa och råtta. Denna hämning kan bidra till att förklara potentiella anticancereffekter av statiner.
Sammanfattningsvis så bidrar våra resultat till ökad kunskap och förståelse kring
statiners verkan i kroppen, samt medverkar till ökad insikt om funktionella
ämnesspecifika skillnader mellan statiner.
2
2 INTRODUCTION
2.1 THE HISTORY OF STATINS
In the second half of the 19th century, the German pathologist Rudolf Virchow
discovered that artery walls of patients dying from occlusive vascular disease were
often thickened and irregular. He also observed that they also contained a fatty,
yellowish substance later identified as cholesterol [1]. This pathological condition was
termed atheroma, the Greek word for porridge [2].
In the 1950s scientists revealed a link between high blood cholesterol levels and
cardiovascular disease, known as the lipid hypothesis [3]. Treatment was limited
essentially to dietary changes (reductions in saturated fats and cholesterol), the bileacid sequestrants (cholestyramine and colestipol), nicotinic acid (niacin), the fibrates
and probucol. Unfortunately, all of these treatments have limited efficacy or
tolerability, or both. Novel and more effective ways to lower blood cholesterol levels
without modifying the diet and lifestyle of subjects suffering with elevated blood
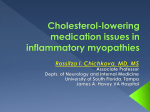
cholesterol levels became high priority [2]. HMG-CoA reductase was found to be the
rate-limiting enzyme in the cholesterol biosynthetic pathway (Figure 1) and hence
became a natural target for drug development.
Figure 1: The biosynthetic pathway of cholesterol
3
C. Skogastierna
In contrast to other late-stage intermediates there are alternative metabolic pathways
for the breakdown of hydroxymethylglutarate when HMG-CoA reductase is inhibited,
rendering no build-up of potentially toxic precursors.
In 1971, Akira Endo, a Japanese biochemist, in the search for a antimicrobial agent
discovered the natural cholesterol-lowering substance mevastatin (ML-236B) [4]
produced by the fungus Penicillium citrinum. Endo and his team believed that certain
microorganisms may produce inhibitors of the enzyme HMG-CoA reductase to defend
themselves against other organisms, as the product, mevalonate, is a precursor of many
substances required by organisms for the maintenance of their cell wall (ergosterol) or
cytoskeleton (isoprenoids) [5]. Mevastatin was however never marketed, because of its
adverse effects with tumors, muscle deterioration, and sometimes death in laboratory
dogs. By 1978, Alfred Alberts and colleagues at Merck Research Laboratories isolated
another natural product in a fermentation broth from the fungus Aspergillus terreus.
This compound was called mevinolin (MK803), later known as lovastatin and first
marketed in 1987 as Mevacor.
When lovastatin (Mevacor, Altocor, Altoprev) became available for prescription use,
physicians were able, for the first time, to easily obtain large reductions in plasma
cholesterol. Lovastatin at its maximal recommended dose of 80 mg daily produced a
mean reduction in LDL cholesterol (low density lipoprotein cholesterol, or the “bad
cholesterol”1) of 40 %, a far greater reduction than could be obtained with any of the
treatments available at the time. Equally important, the drug produced very few
adverse effects, and with once- or twice-daily dosing, was easy for patients to take.
For these reasons, lovastatin was rapidly accepted by prescribers and patients. The
second entrant, simvastatin (Zocord, Lipex), which differs from lovastatin only in that
it has an additional side chain methyl group, was initially approved for marketing in
Sweden in 1988 and subsequently worldwide. Pravastatin (Pravachol, Selektine,
Lipostat) followed in 1991, fluvastatin (Lescol) in 1994, atorvastatin (Lipitor, Torvast)
in 1997, cerivastatin in 1998, rosuvastatin (Crestor) in 2003, pitavastatin in 2003
(Livalo, Pitava). Atorvastatin became by 2003 the best-selling pharmaceutical in
history.
Some types of statins are naturally occurring, and can be found in such foods as oyster
mushrooms and red yeast rice. Lovastatin is a fermentation product, simvastatin is a
semisynthetic derivative of lovastatin and pravastatin is derived from the natural
product compactin by biotransformation2. All other HMG-CoA reductase inhibitors
1
Low-density lipoprotein, or LDL, is one of the five major groups of lipoproteins that enable transport of
multiple different fat molecules, including cholesterol, within the watery extracellular matrix and within
the water-based blood stream. Higher levels of a certain types of LDL particles have been coupled to
promotion of health problems and cardiovascular disease, and are therefore often informally termed the
bad cholesterol, as opposed to HDL particles, which are frequently referred to as good cholesterol or
healthy cholesterol particles.
2
Biotransformation is the chemical modification (or modifications) made by an organism of a chemical
compound such as (but not limited to) nutrients, amino acids, toxins and drugs in the body, rendering
polar compounds to be excreted in the urine.
4
are fully synthetic products. The structures of these drugs are shown in Figure 5. The
generic names for all HMG-CoA reductase inhibitors end with ‘statin’, and the
members of this class are today often referred to as ‘statins’, as opposed to the formal,
although rather cumbersome, class name ‘HMG-CoA reductase inhibitors’. All
inhibitors of HMG-CoA reductase produce a qualitatively similar effect on the lipid
profile [6]. The mean reduction in LDL cholesterol attainable with the maximal
recommended dose of different statins ranges from 35 to 55 %.
2.2 CHOLESTEROL
Cholesterol is a waxy steroid of fat and an essential structural component of
mammalian cell membranes, required for establishing proper membrane permeability
and fluidity through the interaction with the phospholipid fatty acid chains [7, 8].
Within the cell membrane, cholesterol also functions in intracellular transport, cell
signaling and nerve conduction. It is essential for the structure and function of
invaginated caveolae and clathrin-coated pits, including caveola-dependent and
clathrin-dependent endocytosis [9]. Within cells, cholesterol is the precursor molecule
in several biochemical pathways, for example the production of bile salts in the liver
hepatocytes, for the synthesis of vitamin D and the steroid hormones, including the
adrenal gland hormones cortisol and aldosterone, as well as the sex hormones
progesterone, estrogens and testosterone, and their derivatives.
Mammalian cells retrieve cholesterol primarily from two sources; from outside the cell
by receptor mediated endocytosis of LDL or by new synthesis from acetyl-CoA. All
cells in the body are able to produce cholesterol, but with relative production rates
varying with cell type and organ function. It is a complex 37 step process, involving
more than 30 enzymes starting with the intracellular protein enzyme HMG-CoA
reductase. Cholesterol is the principal sterol synthesized by vertebras, formed
predominantly in the liver. Other sites of higher synthesis rates include the intestines,
adrenal glands, and reproductive organs. Cholesterol is extensively recycled; upon
excretion by the liver via the bile into the digestive tract, typically about 50 % of the
excreted cholesterol is reabsorbed by the small bowel back into the bloodstream, where
it is carried around by different lipoproteins.
For a person of about 68 kg, the average de novo synthesis of cholesterol in the body is
about 1 g per day. The total body content of the same person is about 35 g, primarily
located within the membranes of all the cells of the body. Typical daily dietary intake
of additional cholesterol, in the United States, is 200 – 300 mg [10]. Small quantities
are synthesized in other cellular organisms (eukaryotes) such as plants and fungi, but it
is almost completely absent among prokaryotes, i.e. bacteria.
2.2.1 Biosynthesis of cholesterol
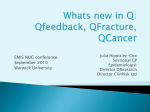
HMG-CoA reductase is a resident glycoprotein of the endoplasmic reticulum (ER) that
consists of two distinct domains; a hydrophobic N-terminal domain with eight
5
C. Skogastierna
membrane-spanning regions and a hydrophilic C-terminal domain that projects into the
cytosol, which exerts the catalytic activity [11]. The N-terminal domain of the enzyme,
which anchors the protein in membrane of the ER, contains sites for binding of
regulatory proteins (Insig) and sterol-regulated ubiquitination (Figure 2) [12-14],
sensing signals for its degradation. The enzyme activity can also be reduced by
phosphorylation by an AMP-activated protein kinase, leading to halted cholesterol
synthesis when ATP levels are low [15]. As a key enzyme in this pathway, HMG-CoA
reductase is regulated by feedback mechanisms operating at multiple levels:
transcription, translation, posttranslational modification and protein degradation.
Figure 2: The HMG-CoA Reductase enzyme with its two distinct domains; the hydrophobic Nterminal domain which anchors the protein in membrane of the ER and the hydrophilic,
catalytically active C-terminal domain that projects into the cytosol.
Biosynthesis of cholesterol is directly regulated by the cholesterol levels present
through classic end product feedback inhibition. When cells are depleted of sterols,
membrane-bound transcription factors called sterol regulatory element binding
proteins, SREBPs, together with another protein, SCAP (SREBP-cleavage-activating
protein), dissociate from the membrane to the Golgi apparatus. Two proteases, S1P and
S2P, activated by SCAP, cleave SREBP to a water soluble N-terminal domain that
subsequently is translocated to the nucleus. The activated SREBP bind to specific sterol
regulatory element DNA sequences, thus upregulating the synthesis of proteins
involved in sterol biosynthesis, including the LDL receptor and HMG-CoA reductase
(Figure 3). In sterol-overloaded cells, SREBP is inactive and transcription of these
genes falls, synthesis of additional sterols is reduced and sterol levels returns to normal
[16-18]. These homeostatic mechanisms involved are only partly understood.
6
Figure 3: Low intracellular levels of cholesterol stimulate the expression of proteins involved in
sterol synthesis, including HMG-CoA reductase and LDL-receptor proteins.
Although cholesterol is important and necessary for human health, high levels of
cholesterol in the blood is associated with damage to arteries and cardiovascular
disease, which leads us to the next topic, unbalanced cholesterol levels and what that
can do to your blood vessels.
2.2.2 Cholesterol and cardiovascular disease
The term ‘cardiovascular disease’ can be confusing. Commonly, it centers on
atherosclerosis, focusing on cholesterol levels, plaque formation, and the narrowing and
hardening of the arteries. From here, it is necessarily linked to the other diseases that
lead to and result from these changes, including hypercholesterolemia, diabetes,
hypertension and stroke. This broadens the scope of the relevant pathophysiology
tremendously. Atherosclerosis can be further linked with metabolic syndrome, which is
a group of risk factors (obesity, insulin resistance, aging, genetic predisposition) that
increase the risk for coronary artery disease, stroke and type 2 diabetes. Cardiovascular
disease, in this broad sense then, is not so much a single disease as an extensive web of
interconnected diseases.
2.2.2.1 Cholesterol affecting endothelial cells
A functional arterial blood vessel is to a large extent dependent on endothelial cells to
release vasoactive agents, such as nitric oxide and prostacyclin. In atherosclerotic and
high LDL-cholesterol vessels, this endothelium-dependent relaxation is lessened.
Several studies have shown that patients with increased cholesterol levels (mainly
oxidized LDL) have reduced ability to respond with vasodilation to acetylcholine, also
7
C. Skogastierna
in vessels without any visibly apparent atherosclerosis. Hypercholesterolemic patients
also lack the ability to release nitric oxide. Lipid lowering therapy with statins improves
and normalizes the ability to relax and dilate the blood vessels [19, 20].
2.3
PHARMACOLOGY OF STATINS
2.3.1 Function and molecular properties
HMG-CoA reductase is the rate-limiting step in cholesterol biosynthesis. The liver is
the main target for HMG-CoA reductase inhibition since most of the circulating
cholesterol comes from internal liver production rather than the diet. Statins are
competitive antagonists of HMG - CoA, as they directly compete with the endogenous
substrate for the active site cavity of HMG-CoA reductase. By blocking this enzyme,
the first committed enzyme of the HMG-CoA reductase pathway, they reduce the rate
by which the enzyme is able to produce mevalonate, the consecutive molecule in the
cascade that eventually produces cholesterol (see Figure 1). This ultimately reduces
cholesterol as well as a number of other compounds, including the isoprenoids
(required for production of dolichol3), tRNA isopentenylation, heme A, ubiquinone 4,
and prenylated5 proteins such as Ras [15]. Products of the isoprenoid pathway are
also required for proper germ cell migration during development [21].
When HMG-CoA reductase is inhibited by statins, intracellular sensors detect low
cholesterol levels and stimulate endogenous production by the HMG-CoA reductase
pathway, as well as increasing lipoprotein uptake by up-regulating the LDL-receptor.
The LDL receptor then relocates to the liver cell membrane and binds passing LDL and
VLDL particles. LDL and VLDL (very low density lipoprotein) extracted from the
circulation into the liver where the cholesterol is reprocessed into excretable bile salts.
The end result is lower LDL, TG (Triglycerides) and total cholesterol levels, as well as
increased HDL (High Density Lipoprotein) levels in serum [2, 4].
2.3.1.1 Structure
All statins have the same pharmacophore, a HMG-like moiety, which may be present in
an inactive lactone form. In vivo, these prodrugs are enzymatically hydrolyzed to their
active hydroxy-acid forms [22, 23]. The inhibitors differ from each other and from the
natural enzyme substrate in the rigid, hydrophobic structures covalently linked to the
HMG-like moiety (Figure 4), which also accounts for most of their difference in
3
Dolichols are long-chain mostly unsaturated organic compounds, involved in many processes in the
body; for example the co-translational modification of proteins known as N-glycosylation, the
posttranslational modifications of proteins and they can function as a membrane anchor of certain
oligosaccharides.
4
Ubiquinone is a component of the electron transport chain and participates in aerobic cellular
respiration, generating energy in the form of ATP.
5
Prenylation is the addition of hydrophobic molecules to a protein.
8
pharmacodynamic6 effects, such as affinity for the active site of the HMG-CoA
reductase, rates of entry into hepatic and non-hepatic tissues, availability in the
systemic circulation for uptake into non-hepatic tissues and routes and modes of
metabolic transformation and elimination. The activity of each statin is dependent on
the binding affinity of the compound at the substrate site and the length of time it binds
to the site [24].
HMG-CoA Reductase
inhibitor
HMG-CoA
Figure 4: The pharmacophore of statins (HMG-CoA reductase inhibitor). Shown for reference is
also the structure of HMG-CoA.
The statins can be classified as type I or type II statins due to their structural
relationship. The type I are nonsynthetic inhibitors, such as lovastatin, pravastatin and
simvastatin, with a decalin ring structure linked to the HMG-like moiety. Type II
statins are synthetic inhibitors featuring larger fluorophenyl groups linked to the HMGlike moiety and include fluvastatin, atorvastatin, cerivastatin and rosuvastatin (Figure
5). These additional groups are responsible for additional polar interactions that cause
tighter binding to the HMG-CoA reductase enzyme and range in character from very
hydrophobic (eg, cerivastatin) to partly hydrophobic (eg. rosuvastatin) [22, 25, 26].
6
Pharmacodynamics is the study of the biochemical and physiological effects of drugs at its site of
action, the mechanisms of drug action and the relationship between drug concentration and effect.
9
C. Skogastierna
Type 1
Butyryl group of
Butyryl group of
type
1 statins
type
1 statins
pravastatin
simvastatin
lovastatin
Type 2
rosuvastatin
fluvastatin
atorvastatin
Figure 5: The chemical structures of statins. Type 1 statins, e.g. lovastatin, simvastatin and
pravastatin, are partially reduced napthylene ring structures with a butyryl group. Type 2 statins all
exist in their active hydroxy-acid forms. Fluvastatin has an indole ring structure, while atorvastatin and
rosuvastatin have pyrrole and pyrimidine based ring structure respectively.
10
2.3.1.2 Comparative pharmacology of statins
The statins differ in their absorption, plasma protein binding, excretion and solubility
(Table 1), and exhibit variable dose-related efficacy in reducing LDL-C [27, 28]. They
are often divided into two groups depending on origin; naturally occurring or synthetic
(Table II).
Table I. Comparative efficiency and pharmacology of statins.
Drug
Reductio
n in LDL
(%)
Increase
in HDL
(%)
Reduction
in TG (%)
Metabolism
Protein
binding
(%)
T1/2 (h)
Hydrophilic
IC50
(nM)
FLU
22 – 36
3 – 11
12 – 25
CYP2C9
98
0,5 – 3,0
No
28
SIM
26 – 47
8 – 16
12 – 34
CYP3A4
95 – 98
1–3
No
11
ATV
26 – 60
5 – 13
17 – 53
CYP3A4
98
13–30
No
8
ROS
45 – 63
8 – 14
10 – 35
CYP2C9
88
19
Yes
5
LOV
21 – 42
2 – 10
6 – 27
CYP3A4
>95
2–4
No
NA
PRA
22 – 34
2 – 12
15 – 24
Sulfation
43 – 67
2–3
Yes
44
TC indicates total cholesterol; TG, triglycerides; T1/2, half-life. FLU indicates fluvastatin; SIM ,
simvastatin; ATV, atorvastatin; ROS, rosuvastatin; LOV, lovastatin; PRA, pravastatin.
Table II. The statins can be divided into two groups: fermentation-derived and synthetic.
Presentation of some of the most common statins along with brand names, which may vary between
countries.
Statin
Fluvastatin
Simvastatin
Brand name
Lescol, Lescol XL
Zocor, Lipex
Atorvastatin Lipitor, Torvast
Rosuvastatin Crestor
Mevacor, Altocor,
Lovastatin
Altoprev
Pravastatin
Pravachol,
Selektine, Lipostat
Derivation
Synthetic
Fermentation-derived (synthetic derivate of
a fermentation product of Aspergillus
terreus).
Synthetic
Synthetic
Fermentation-derived. Naturally occurring
compound (oyster mushrooms and red
yeast rice).
Fermentation-derived (of bacterium
Nocardia autotrophica).
11
C. Skogastierna
2.3.2 Pharmacokinetics
Statins have different pharmacokinetic7 profiles that are associated with their
physicochemical properties. Most of the statins are metabolized by the liver before
reaching the systemic circulation, which causes their relatively low systemic
bioavailability [29]. Lovastatin and simvastatin are administered in their lactone forms,
which are more lipophilic than their free acid forms, and therefore they have to be
activated by hydrolysis to the active anionic carboxylate form [29]. Cytochrome P450
(CYP) isoenzymes are involved in the oxidative metabolism of the statins, with
CYP3A4 and CYP2C9 isoenzymes being the most dominant. CYP3A4 isoenzyme is
the most predominant isoform involved in metabolism of lovastatin, simvastatin,
atorvastatin and cerivastatin [30]. CYP2C9 isoenzyme is the most predominant isoform
involved in metabolism of fluvastatin, but CYP3A4 and CYP2C8 isoenzymes also
contribute to the metabolism of fluvastatin [29]. Rosuvastatin is metabolized to a small
degree by CYP2C9 and to a lesser extent by CYP2C19 isoenzymes [30, 31].
Pravastatin and pitavastatin undergo little metabolism. Their plasma clearances are
governed by the transporters involved in the hepatic uptake and biliary excretion.
Also for other statins, which are orally administered as open acid forms (i.e.
fluvastatin, cerivastatin and atorvastatin), hepatic uptake transporter(s) play important
roles in their clearances. The statins that have the ability to be metabolized by multiple
CYP isoenzymes may avoid drug accumulation when one of the pathways is inhibited
by co-administered drugs.
Polymorphisms in transporter genes can have profound effects on statin
pharmacokinetics, providing a rational basis for the individualization of lipid-lowering
therapy according to some researchers [32]. The hepatic uptake of many statins are
reduced by a common genetic variant of the organic anion-transporting polypeptide
1B1, increasing the risk of statin-induced myopathy [33]. Similarly, genetically
impaired efflux activity of adenosine triphosphate (ATP)-binding cassette G2
transporter results in a marked increase in systemic exposure to various statins [34].
Importantly, the effects of these genetic polymorphisms differ depending on the
specific statin that is used [35-37].
2.3.3 Clinical applications
Statins are lipid-lowering agents, primarily prescribed to patients with
hypercholesterolemia or hyperlipidemia. In Sweden 2010, about 1/10 of the total
population were prescribed statins at least once (http://www.socialstyrelsen.se). Since
the big breakthrough for statin treatment with the 4S study [38] the treatment
recommendations have been made through monitoring goal LDL-levels, where the
target concentrations have been defined through consensus and gradually lowered with
7
Pharmacokinetics is the determination of the fate of substances administered externally to a living
organism. It includes the study of the mechanisms of absorption and distribution of an administered drug,
the rate at which a drug action begins and the duration of the effect, the chemical changes of the
substance in the body and the effects and routes of excretion of the metabolites of the drug and /or the
drug itself.
12
strengthened evidence for beneficial effects of statins. Clinical practice guidelines
generally recommend that patients have tried "lifestyle modification", including a
cholesterol-lowering diet and physical exercise, before statin use is considered; statins
or other pharmacologic agents may then be recommended for those who do not meet
their lipid-lowering goals through diet and lifestyle approaches [23, 31]. Treatment
with statins for atherosclerotic disease is recommended at total cholesterol levels over
4.5 or LDL cholesterol over 2.5, and is given the highest priority in the guidelines from
The Swedish National Board of Health and Welfare
(http://www.socialstyrelsen.se/nationellariktlinjerforhjartsjukvard/sokiriktlinjerna/atero
sklerotiskkarlsjukdomochk1).
Statins are effective in decreasing mortality in patients with preexisting cardiovascular
disease [39]. They are also currently advocated for use in patients at high risk of
developing heart disease. On average, statins can lower LDL cholesterol by 1.8 mmol/l
(70 mg/dl), which translates into a 60 % decrease in the number of cardiac events (heart
attack, sudden cardiac death) and a 17 % reduced risk of stroke after long-term
treatment [40]. The benefit of statins in secondary prevention8 for treating
cardiovascular disease (CVD) is convincingly shown, but their value in primary
prevention9 remains controversial. A recent meta-analysis on the placebo controlled
studies with statins performed by Cholesterol Treatment Trialists’ (CTT) Collaboration,
comparing low dose statin treatment with high dose, it was demonstrated that high dose
statin treatment reduces the risk even more in relation to the decrease in LDLcholesterol that the high dose treatment resulted in. The CTT authors suggest that
patients with high risk of cardiovascular events would benefit from intensive statin
therapy even if baseline LDL cholesterol is below 2.0 mmol/L [39, 41]. The
Scandinavian IDEAL trial also indicates that health benefits could be obtained with
statin therapy resulting in LDL cholesterol below 2.0 mmol/L compared with those
above this level. This turned some researchers into “the lower the better” advocates,
being convinced that some of the guidelines of today are far too conservative.
However, another recent meta-analysis did not find a mortality benefit in those at highrisk but without prior cardiovascular disease [42], while other reviews concluded that
there is a mortality and morbidity benefit, but concerns regarding the quality of the
evidence were raised [6, 43]. Some researchers conclude that with respect to quality of
life there is limited evidence of improvement when statins are used for primary
prevention [44]. Statins exhibit variable dose-related efficacy in reducing LDL-C [27],
in general a reduction by an additional 7 % with each doubling of the statin dose [45].
Higher doses also give additional CVD improvement effects but at the same time
increase the risk of adverse drug effects, hence in primary prevention the initial risk of
the patient should be decisive if treatment will be recommended. Other researchers
opine that statins are overly used since their use has included groups who do not benefit
from treatment or where evidence for treatment is not clarified [46, 47]. There are also
8
Secondary prevention are methods to diagnose and treat existent disease in early stages before it causes
significant morbidity.
9
Primary prevention are methods to avoid occurrence of disease.
13
C. Skogastierna
investigators that claim that elevated cholesterol levels cannot be coupled to CVD and
that statins thus are not effective nor safe [48].
As a class, the statins have been shown to measurably reduce the burden of
atherosclerotic illness. However, muscle- and, more recently, nerve-related toxicity has
emerged as potential complications contributing to treatment withdrawal [49]. The
adverse effects are relatively rare but severe, and they are thought to a large extent
being dose dependent. This is for example illustrated in the recent SEARCH study,
where 80 mg simvastatin gave more cases of myopathy10 than treatment with 20 mg
simvastatin [50, 51]. Generally, the myopathic signs and symptoms of tenderness,
myalgias, cramping and elevated serum creatine kinase activity are fully reversible after
drug discontinuation. Pathophysiologic clues regarding the potential causes of statin
myopathy with or without neuropathy are discussed with particular attention paid to the
implications of disrupted mevalonate metabolism. For example, secondary defects in
isoprenoid biosynthesis are expected to impair the production of a variety of
intermediaries such as dolichols (crucial for N-linked glycosylation), farnesylpyrophosphate (facilitates the endoproteolytic cleavage and maturation of prelamin A,
and modifies B-type lamins and G-proteins) and geranylgeranyl pyrophosphate
(necessary for coenzyme Q10 and G-protein synthesis). Also
isopentenylpyrophosphate, involved in a nucleoside modification of selenocysteinyltRNA and thus indirectly related to the synthesis of all selenoproteins is proposed to be
affected [49].
The beneficial effects of statins are indeed devaluated by some serious adverse
reactions (ADRs) in the muscular system, liver and kidneys. The ADR frequency varies
in different studies, although often reported to be of low risk. However, the clinical
impression is that muscular side effects are considerably more common as a cause of
termination of statin treatment. Independent studies on the safety and tolerabilty of this
treatment are lacking. There is a poor implementation of statin treatment, in all
probability adverse reactions contribute this, leading to under-treatment [52] and low
adherence to treatment with lipid-lowering drugs [53-56]. Considering that it takes at
least 18 to 24 months to observe an effect of statins on coronary heart disease [38] these
reports are worrying since a large proportion of patients at risk may be untreated.
An alternative way of translating the evidence to treatment guidelines has recently been
presented [57]. The authors advocate that treatment shall be adjusted to the risk of each
individual patient, where low dose of statins would be recommended for individuals at
moderate risk for CVD, and high dose for those at high risk, primarily as secondary
prevention. While no direct comparison exists, all statins appear equally effective on
reducing cardiovascular morbidity and mortality regardless of potency or degree of
cholesterol reduction [6]. A comparison of three statins; atorvastatin, pravastatin and
simvastatin at commonly prescribed doses, found that there are no statistically
10
Myopathy is a muscular condition in which the muscle fibers do not function, resulting in muscular
weakness.
14
significant differences in morbidity and mortality reduction of CVD based on their
effectiveness against placebo [29].
2.4
PLEIOTROPIC EFFECTS OF STATINS
2.4.1 Definition
In pharmacology, pleiotropy refers to the action of a drug, often unanticipated, other
than those for which the agent was specifically developed [58]. It may include adverse
effects which are detrimental, but is often used to denote additional beneficial effects,
illustrated in Figure 6 [59].
HMG-CoA reductase inhibitors (statins)
Cholesterol lowering
(LDL, HDL)
Rho GTPases
T-Cell activation
MCH II expression
chemokine secretion
tissue factor
Acute coronary syndrome
Heart failure
anti-inflammatory action
anti-oxidative effects
NO synthesis/ endothelial function
immunomodulatory effects
anti-cancer
Sepsis
Stroke
Multiple sclerosis
Chronic kidney
disease
Figure 6: Suggested pleiotropic effects of statins.
2.4.2 Statins and the vascular endothelium
The endothelium is the thin layer of cells that lines the interior surface of blood vessels
and lymphatic vessels, forming an interface between circulating blood or lymph in the
lumen and the rest of the vessel wall. The cells that form the endothelium are called
endothelial cells (ECs), and the endothelial cells in direct contact with blood are called
vascular endothelial cells. Vascular endothelial cells line the entire circulatory system,
from the heart to the smallest capillaries. These cells have very distinct and unique
functions that are paramount to vascular biology, including fluid filtration, such as in
the glomeruli of the kidney, blood vessel tone, hemostasis, lipid transport, neutrophil
recruitment and hormone trafficking [60, 61]. Although the exact role of the
15
C. Skogastierna
endothelium in the vascular diseases in vivo remains unclear, accumulating evidence
indicates that endothelial dysfunction is pivotal in the development of atherosclerosis
and its complications [62, 63].
The effectiveness and rapidity of statin-induced decreases in coronary events and
evidence for restoration of endothelial function before significant reduction in serum
cholesterol levels, have led to a continuous expansion of the medical significance of
HMG-CoA reductase in recent years [20, 64-66]. Many of the observed cholesterolindependent or "pleiotropic" vascular effects of statins appear to especially target the
concept of ‘vascular failure’, including the improvement of vascular endothelial
function, inhibition of vascular smooth muscle cell proliferation and migration, antiinflammatory actions, anti-oxidative effects or stabilization of vulnerable plaques [65,
67]. These effects have potential in the treatment of coronary artery disease in various
settings, such as prevention of its onset as well as its progression. Endothelial
dysfunction can be broadly defined as an imbalance between vasodilating and
vasoconstricting substances produced by, and/or acting on the endothelium. It has been
proposed to be of prognostic significance in predicting vascular events including stroke
and heart attacks and to be a useful marker of early cardiovascular diseases. A
dysfunctional endothelium may result from and/or contribute to increased production of
reactive oxygen species (ROS), decreased synthesis, release or activity of endothelial
derived nitric oxide (NO) [68] and /or modified expression/ activity of anti-oxidative
enzymes.
2.4.2.1 Vascular inflammation
Inflammation plays important roles in the genesis, progression and complications of
atherosclerosis and thrombosis [69, 70]. For example, clinical studies have stressed that
in as much as 80 % of all sudden cardiac deaths inflammation is the underlying cause
[71]. The inflamed vascular wall produces exaggerated levels of chemotactic proteins
and increased expression of adhesion molecules, leading to monocytic adhesion,
extravasion and formation of fatty streaks [72]. Other inflammatory mediators,
including mast cells and activated T cells, also attach to endothelial cells and contribute
to the progression of the atheromatous lesion. In addition, smooth muscle cells secrete a
number of factors in this chemically modified environment that contribute to an
increase in the inflammatory response. Some of the inflammatory cytokines, including
IL-6, IL1β and TNFα, induce the release of C reactive protein (CRP) by the liver,
which in turn together with modified LDL, superoxide anions and certain interleukins
may decrease the NO availability, contributing to endothelial dysfunction [73].
Inflammatory cells and molecules augment the risk of plaque rupture and exposure of
subendothelial tissue to blood end platelets through contribution of plaque instability
via the release of chemokines, interleukines and metalloproteinases that degrade the
collagen of the fibrous cap. Proinflammatory eicosanoid production is an important
hallmark of CVD [74]. Statins have been shown to modulate the expression of
16
eicosanoids in a favourable way, and to modulate other factors, reducing inflammation
of diseased blood vessels [75]. Both experimental and clinical outcome data support the
hypothesis that statins, in addition to being potent LDL-lowering agents, also attenuate
plaque inflammation and influence plaque stability. Simvastatin, fluvastatin and
atorvastatin appear to reduce intimal inflammation [76] and suppress the expression of
tissue factor and matrix metalloproteinases both in vivo and in vitro [77, 78], whereas
pravastatin and cerivastatin can reduce macrophage content within experimental
atherosclerotic plaques [79, 80]. Statins may also inhibit expression of adhesion
molecules critical for monocyte attachment and adhesion to the vascular endothelium
[81].
2.4.2.2 Oxidative stress
In all aerobic cells, being dependent on oxygen for energy production in the respiratory
chain, ROS (reactive oxygen species) are formed. Thus, all aerobic cells are dependent
on efficient machineries for detoxification of ROS. When excessive oxidative load risk
to damage the cells, these natural efficient defense systems are activated and an
intracellular reducing environment is created due to the presence of anti-oxidative stress
enzymes like these studied in Paper III (Figure 7). The condition called oxidative
stress occurs when redox homeostasis within the cell is altered, due to either an
overproduction of ROS or a deficiency in antioxidant defense mechanisms, leading to
up regulation of these systems. If these systems do not work properly, excess reactive
oxygen species can be deleterious. They can for example inhibit endotheliumdependent vasodilator pathways (i.e. the NO pathway and the endothelium-derived
hyperpolarizing factor (EDHF) pathways) and shift the balance in eicosanoids action
from vasodilatation and antithrombosis towards endothelial dysfunction,
vasoconstriction and thrombosis. Accumulating data suggest that several
proatherogenic stimuli lead to increased production of ROS within the endothelial
microenvironment and the resultant excessive oxidative stress plays a key role in
mediating the pathologic manifestations of EC dysfunction associated with
cardiovascular diseases such as hypertension, atherosclerosis or vascular diabetic
complications [82].
It is important to remember, that although ROS often are mentioned in negative
context, they also serve as regulators for crucial cellular functions, including the
regulation of many important proteins in signal transduction, such as protein kinase C
and tyrosine kinases [83] as well as the regulation of redox-sensitive transcription
factor like Nuclear Factor k (NFk) and activator protein-1 (AP-1) [84]. In addition,
activated phagocytes in the immune system produce ROS to kill bacteria [85].
Antioxidants in mammals include the lipid soluble vitamin E and ubiquinol, the water
soluble vitamin C, glutathione (GSH) and thioredoxin (Trx). Of major importance are
also the enzymatic antioxidants and antioxidant regenerating systems including the
superoxide dismutase (SOD), catalases (Cat), thioredoxin system (Trx system),
glutathione peroxidase (GPx) and the glutathione system [86].
17
C. Skogastierna
Figure 7: Reactive oxygen species and antioxidant systems in the vasculature. Highlighted in black
are the most important ROS of the vascular cells. Oxidases, such as NADPH oxidase or xanthine oxidase,
transfer an electron to oxygen, which is converted to superoxide (O2−). Superoxide dismutase (SOD)
converts superoxide to hydrogen peroxide (H2O2), which can be converted to H2O by either catalase or
glutathione peroxidase. H2O2 may also be converted to a hydroxyl radical (OH) in the presence of
reduced iron (Fe2+). Superoxide may also react with nitric oxide (NO) to form peroxynitrite (ONOO−),
which is unstable at a pH lower than 8, and therefore rapidly decomposes to OH. There is competition
between NO and SOD for O2−.
2.4.2.3 The thioredoxin system
The thioredoxin system comprises thioredoxin (Trx), thioredoxin reductase (TrxR) and
NADPH (Figure 8) [87]. The system exists in all living cells and is essential proteins
for regulating cellular redox balance and mitigating the damage caused by reactive
oxygen species. The system also participates in redox signaling using molecules like
hydrogen peroxide and nitric oxide [88] and in the regeneration of antioxidants,
including ascorbic acid [89] and lipoic acid [90] as well as ubiquinone. Up-regulation
of Trx and TrxR in several forms of cancer as well as during the carcinogenetic process
have been reported [91-93].
Figure 8: The thioredoxin system which includes thioredoxin (Trx), thioredoxin reductase (TrxR)
and NADPH.
18
Thioredoxins are a family of 12-kD redox active proteins ubiquitously expressed in
both prokaryotic and eukaryotic cells [94, 95] that have been implicated in a variety of
physiological processes and biological pathways. Trx1 is mainly found in the cytosol
but can be translocated to the nucleus. In addition of being an electron donor for
ribonucleotide reductase, Trx1 participates in the intracellular defence against oxidative
stress by restoring intracellular thiols11 lost by oxidation and regenerates other
antioxidant enzymes such as peroxiredoxins [86, 87]. Trx1 is also involved in signal
transduction and regulation of transcription factors, for example NF-Upon
oxidation of NF-in the nucleus Trx1 restores the DNA-binding activity, but in the
cytosol Trx1 is being inhibiting [96]. Since ROS are involved in the regulation of
intracellular signalling pathways, Trx1 may indirectly influence this regulation by
being a ROS scavenger. In addition, Trx1 contributes to the regulation of apoptosis by
binding to ASK-1 in a redox dependent manner and regulating the activity of p53 in
several ways. Trx is present in human plasma [97] and certain cells in the immune
system as well as various tumor cells have been shown to secret Trx extracellulary [98100]. Extracellulary, Trx has growth factor-like effects in an autocrine manner as well
as proinflammatory effects, inducing chemotaxis of neutrophils, monocytes and T-cells
[101].
TrxR, redox-active selenoenzymes, reduce Trx in a NADPH-dependent fashion [102],
and is a central component in the thioredoxin system [103]. Humans express three
thioredoxin reductase isozymes; TrxR1, TrxR2 and TrxR3. TrxR belongs to a family of
NADPH-dependent pyridine nucleotide-disulfide oxidoreductases, to which
glutathione reductase, lipoamide dehydrogenase and mercuric ion reductase also belong
[104]. The mammalian TrxR has an exceptionally broad substrate specificity in
comparison to the other enzymes of this family [105]. Mammalian TrxR is a
homodimer composed of two identical 58 kDa subunits, with a FAD-domain and a
NADPH-binding site in each subunit [106]. Three different isoforms of the mammalian
enzyme have been described so far. The classical TrxR1 is found in the cytosol, TrxR2
is localised in the inner mitochondria membrane and is structurally and biochemically
very similar to TrxR1 [107, 108] and the third TrxR isoenzyme, TGR, is expressed only
in testis. TrxR has been shown to be secreted extracellulary both by neoplastic and
normal cells and is present in human plasma [109].
2.4.2.4 Carcinogenesis due to chemical modification
Chemical alterations in DNA may occur due to chemical modifications of DNA-bases
caused by for example ROS or binding of chemical compounds to DNA, possibly
leading to errors during the replication process. Such DNA lesions are usually rapidly
discovered and eliminated by the DNA repair systems, but if cell division occurs before
DNA repair is complete, mutated daughter cells appear that might bear dysfunction in
11
A thiol is an organosulfur compound containing a carbon-bonded sulfhydryl (–C–SH or R–SH) group
(where R represents an alkane, alkene, or other carbon-containing group of atoms). Thiols are the sulfur
analogue of alcohols (that is, sulfur takes the place of oxygen in the hydroxyl group of an alcohol). The –
SH functional group itself is referred to as either a thiol group or a sulfhydryl group.
19
C. Skogastierna
their growth regulation, including defect contact inhibition and dysfunction in their
apoptotic machinery, possibly developing into a tumor. Such a mutated cell that shows
a growth advantage under the influence of a selective pressure during promotion
compared to the surrounding, normal cells, is called an initiated cell. The initiated cells
can respond to growth stimulatory signals appearing during regeneration after cell
injury and are able to grow under circumstances where growth is inhibited in normal
cells. As a consequence, focal proliferation may occur, generating clones of altered
preneoplastic cells [110]. Genetic instability facilitates further mutations and after
several steps of genetic alteration and selection due to growth advantages, malignant
tumor cells develop. The different cells within the same tumor can show great and
progressive genetic variability although they all, from the very beginning of the
carcinogenesis, originate from one single cell [110-112].
In experimental models the preneoplastic as well as the neoplastic12 cells are
characterised by changes in the expression of drug metabolising enzymes, upregulation of antioxidants and antioxidant regenerating systems and a capacity to avoid
apoptosis [113-115]. The carcinogenetic process can be described as a chronic selection
of cells with a drug resistant phenotype, at least for tumors that develop as a
consequence of environmental exposure and chronic cell injury.
During recent years it has been proposed that statins have anticarcinogenic effects, both
in liver [116, 117] and in other tissues such as the prostate, lung and pancreas [118121].
2.4.3 Prostanoids
The biosynthesis of prostanoids is initiated by the activation of phospholipase A2
(PLA2) and subsequent release of arachidonic acid (AA) from cell membranes. The AA
is then transformed by cyclooxygenases (COX) and specific prostaglandin (PG)
synthases. There are two major COX enzymes, COX-1 and COX-2, which differ in
structure, tissue distribution, subcellular localization and function. COX-1 is commonly
described as ubiquitous and constitutively expressed. COX-2 is on the other hand
normally absent from most cell types. Its expression is induced at sites of inflammation
and vascular injury by inflammatory mediators like TNF-α and IL-1β, and its mRNA as
well as protein have short half-lives. Both enzymes are membrane-bound homodimers,
found predominantly on the perinuclear membranes producing the intermediate PGH2,
which is then converted to the final prostanoid products by tissue specific, terminal
enzymes. For example, the predominant prostaglandin formed in endothelial cells after
12
Neoplasm is an abnormal mass of tissue as a result of neoplasia ("new growth" in Greek), the abnormal
proliferation of cells. Preneoplastic cells, such as metaplasia (cell type conversion) or dysplasia
(maturation abnormality) often undergo an abnormal pattern of growth but do not always progress to
neoplasia. The growth of neoplastic cells exceeds and is not coordinated with that of the normal tissues
around it. The growth persists in the same excessive manner even after cessation of the stimuli, usually
causing a lump or tumor. Neoplasms may be benign, pre-malignant (carcinoma in situ) or malignant
(cancer).
20
PLA2 activation is prostacyclin (PGI2) due to high expression of prostacyclin synthase
(PGIS, also known as CYP8A1). PGIS is a single-pass membrane-bound protein,
situated in the endoplasmic reticulum and isomerizes PGH2 to PGI2. It is also abundant
in the ovary, heart, skeletal muscle, lung, and prostate. Unlike most P450 enzymes,
PGIS does not require molecular oxygen (O2), instead it uses its heme cofactor to
catalyze the isomerization of prostaglandin H2 to prostacyclin.
2.4.3.1 Prostacyclin
PGI2 is released by healthy endothelial cells and performs its function through a
paracrine signaling cascade that involves G protein-coupled receptors on nearby
platelets, endothelial cells and smooth muscle cells; regulating homeostasis,
hemostasis, smooth muscle function, preventing inflammation, dilating vessels,
inhibiting platelet aggregation and also separating existing aggregates in vitro. PGI2 is
therefore considered to play an important role in vasoprotection and its deficiency may
lead to thrombosis and other vascular lesions [122, 123].
While the expression of PGIS is constitutive, the production of PGI2 can be
dramatically increased by the induced expression of COX-2, particularly in vascular
cells and macrophages. PGI2 is rapidly secreted from source cells, presumably through
an ATP-binding cassette (ABC) transporter, activating neighboring cells which bear the
specific I-prostanoid (IP) receptor, a G-protein coupled receptor (GPCR). The PGI2/IP
interaction signals through the Gαs subunit to stimulate G protein-coupled increase in
cAMP and protein kinase A (Figure 9, modified from www.caymanchem.com),
resulting in decreased [Ca2+]i. It could also cause inhibition of Rho kinase, leading to
vascular and bronchial smooth muscle relaxation. In addition, PGI2 intracrine signaling
may target nuclear peroxisome proliferator-activated receptors and regulate gene
transcription, suppressing the production of proinflammatory cytokines, angiogenic
cytokines, and mediators of extracellular matrix remodeling (e.g., IL-1β IL-6, VEGF,
TGF-α, thromboxane).
The transcriptional regulation of the human PTGIS gene is poorly understood. The core
PTGIS promoter contains several presumed cis-acting elements for different
transcription factors like Sp1, NFB and AP-2, which have been shown to be linked to
induction of other genes after treatment with statins [124, 125]. The PTGIS promoter
activity has been shown to be regulated by epigenetic mechanisms in human cancer
cells [122, 126] but the genetic regulation in normal cells is not well studied.
21
C. Skogastierna
Figure 9: Prostacyclin (PGI2) is synthesized from arachidonic acid (AA) in endothelial cells by
the COX pathway via prostacyclin synthase (PGIS). Secreted PGI2 activates the IP receptor on
neighbouring smooth muscle cells, which induces cAMP synthesis from ATP.
2.4.3.2 Thromboxane
Thromboxanes are a group of prostaglandins named for their role in clot formation
(thrombosis). Thromboxane A2 (TXA2), one of the major forms, is in the
cardiovascular system predominantly derived from platelet COX-1. The interaction
with the G-protein-coupled TXA2 receptor, TP, elicits not only platelet aggregation and
smooth muscle contraction but also the expression of adhesion molecules and the
adhesion and infiltration of monocytes/macrophages [127]. Vasoconstriction and
various pro-inflammatory effects exerted by TXA2 on tissue microvasculature is
considered to be strong contributing factors to why TXA2 is pathogenic in various
diseases, such as ischemia-reperfusion injury, hepatic inflammatory processes, acute
hepatotoxicity etc. [128, 129].
2.4.3.3 Prostacyclin vs. Thromboxane
In the circulatory system, TXA2 is in homeostatic balance with PGI2 [74]. The balance
of the oppositely-acting COX-derived prostanoids influences many processes
throughout the body, such as blood pressure regulation, clotting, and inflammation. The
22
PGI2/TXA2 ratio is of particular interest in vivo, with the corresponding synthases
shown to be differentially regulated in a variety of disease states [130, 131]. In many
cardiovascular diseases, the widespread vascular and organ inflammation and the
associated oxidative stress, enhance the production of eicosanoids and shift their
production/effects from vasodilatation and anti-thrombosis to vasoconstriction,
prothrombosis and further inflammation [132, 133], representing the functional
characteristics of endothelial dysfunction. An imbalance towards TXA2 seems to
promote atherosclerosis and increase risk for cardiovascular events, while an imbalance
towards PGI2 likely inhibits the development of CVD [134-136].
The widely used drug aspirin13 acts by irreversibly binding to COX and thus inhibits
the synthesis of the precursors of thromboxane within platelets. This anticoagulant
property makes aspirin useful for reducing the incidence of heart attacks, strokes, and
blood clot formation in people at high risk of developing cardiovascular diseases.
Aspirin irreversibly inhibits COX-1 and modifies the enzymatic activity of COX-2.
High analgetic doses of aspirin inhibits COX-2, disturbing the synthesis of PGI2 and
thus the protective anti-coagulative effect of PGI2 is decreased, increasing the risk of
thrombus and associated heart attacks and other circulatory problems. Newer NSAID
drugs, COX-2 inhibitors (coxibs), have been developed to inhibit only COX-2, with the
intent to reduce the incidence of gastrointestinal side-effects but [137] several of the
new COX-2 inhibitors have been withdrawn recently, after evidence emerged that
inhibition of COX-2 increases the risk of heart attack and stroke due to prostacyclin
down-regulation relative to thromboxane levels, as COX-1 in platelets is unaffected
[138]. Thus, the protective anticoagulative effect of PGI2 is removed, increasing the
risk of thrombus and associated heart attacks and other circulatory problems.
Prostacyclin synthase and thromboxane synthase signaling via arachidonic acid
metabolism affects a number of tumor cell survival pathways such as cell proliferation,
apoptosis, tumor cell invasion and metastasis, and angiogenesis. However, the effects
of these respective synthases differ considerably with respect to the pathways
described. While prostacyclin synthase expression generally is believed to be antitumor, a pro-carcinogenic role for thromboxane synthase has been implicated in a
variety of cancers [139-142]. In contrast, increased prostacyclin synthase expression
and activity has been suggested protect against tumor development [143-145].
13
Aspirin, also known as acetylsalicylic acid (abbreviated ASA), is a salicylate drug often used as an
analgesic to relieve minor aches and pains, as an antipyretic to reduce fever and as an antiinflammatory medication. Aspirin acts as an acetylating agent whereby an acetyl group is covalently
attached to a serine residue in the active site of the COX enzyme, making aspirin different from other
NSAIDs such as diclofenac and ibuprofen, which are reversible inhibitors. Aspirin is today one of the
most widely used medications in the world.
23
C. Skogastierna
2.4.4 Nitric Oxide
Nitric oxide (NO) is synthesized by the enzyme Nitric Oxide Synthase (NOS) in
biological systems. NOS is a remarkably complex enzyme which acts on molecular
oxygen, arginine and NADPH to produce NO, citrulline and NADPH+. This process
requires five additional cofactors; FMN, FAD, Heme, calmodulin and
tetrahydrobiopterin, and two divalent cations; calcium and heme iron. Three different
isoforms of NOS have been identified; neuronal, endothelial and inducible NOS. NO is
produced in trace quantities by neurons, endothelial cells, platelets and neutrophils in
response to homeostatic stimuli [146, 147] and scavenged rapidly, having a half-life of
about four seconds. NO acts in a paracrine fashion to transduce cellular signals through
interaction with guanylate cyclase, leading to activation of the enzyme and
subsequently increased cGMP levels. Other cells also produce NO, e.g. macrophages,
fibroblasts, and hepatocytes, in response to inflammatory or mitogenic stimuli,
providing a defense mechanism against pathogens through oxidative toxicity. These
high NO levels lead to the formation of peroxynitrite, destruction of iron-sulfur
clusters, nitration of protein tyrosine residues and thiol nitrosation. Thus, the amount of
NO produced in different biological systems can vary over several orders of magnitude
and its subsequent chemical reactivity is diverse.
24
3 AIMS
In the work included in this thesis, I have studied some of the commonly prescribed
HMG-CoA reductase inhibitors with respect to the vascular endothelium. More
specifically the aims were to:
Investigate the influence in vitro of clinically relevant fluvastatin concentrations on
the metabolism and production of eicosanoids and NO in human endothelial cells.
Study the impact on vascular function after fluvastatin exposure.
Study how clinically relevant simvastatin concentrations affect the production and
balance of two of the most important vascular active prostaglandins, prostacyclin
and thromboxane A2, in vitro as well as in vivo.
Compare fluvastatin and simvastatin with regard to impact on oxidative stress in
human vascular endothelium in vitro and in vivo.
Evaluate the suggested anti-carcinogenic properties of statins in relation to
expression of the redox-active enzymes TrxR, by investigating if statin treatment is
associated with alterations in the hepatic expression of TrxR.
25
C. Skogastierna
4 METHODOLOGICAL CONSIDERATIONS
The purpose of this section is to provide a methodological overview, considerations and
limitations to some of the techniques used in the studies of this thesis. More detailed
descriptions of the separate methods can be found in the Material and Methods section
of paper I-IV.
4.1
EXPERIMENTAL SYSTEMS
4.1.1 Cell culture systems
Endothelial cells are situated at the interface between the circulating blood and the
vessel wall. They serve as a sensor and transducer of signals within the circulatory
microenvironment and is integral in maintaining the homeostatic balance of the vessel
through the production of factors that regulate vessel tone, coagulation state, lipid
transport, cellular proliferative response and leukocyte trafficking [60, 61]. Cultivated
endothelial cells isolated from human vessels are commonly used for physiological and
pharmacological investigations. Endothelial cells vary in morphology and functions
according to the type and size of the associated vessel. The work presented in this
thesis involves therefore endothelial cells from two different locations in the body;
aorta and umbilical cord. Furthermore, only primary cells were used. Primary cells are
taken directly in vivo (e.g. biopsy material) and established for growth in vitro. These
cells have undergone very few population doublings and are therefore more
representative of the main functional component of the tissue from which they are
derived in comparison to continuous (tumor or artificially immortalized) cell lines, thus
representing a more representative model of the in vivo state. With the exception of
cells derived from tumors, most cell cultures have limited lifespan. After a certain
number of population doublings (called the Hayflick limit), cells undergo the process of
senescence and stop dividing, while generally retaining viability. The cells used in our
work were well within the limit of population doublings recommended by the
manufacturer.
In general, human endothelial cells are isolated from normal human tissue, in this case
large blood vessels. Human aortic endothelial cells (HAEC) are isolated from the
human ascending (thoracic) and descending (abdominal) aorta and human umbilical
vein endothelial cells (HUVEC) are isolated from the vein of the umbilical cord. These
cells are commercially available; we used pooled cells isolated from five different
donors, provided by PromoCell (Heidelberg, Germany). Shortly after isolation, cells
are cryopreserved in liquid nitrogen at passage one or passage two until experiments
are carried out. Rigid quality control tests are performed for each lot of cells. They
are tested for cell morphology, adherence rate and cell viability, cell-type specific
markers, e.g. von Willebrand Factor and CD31, as well as Dil-Ac-LDL uptake assays.
Growth performance is tested through multiple passages up to 15 population
doublings under culture conditions without antibiotics and antimycotics. In addition,
26
all cells have been tested for the absence of HIV-1, HBV, HCV and microbial
contaminants (fungi, bacteria, and mycoplasma).
4.2
STUDY SUBJECTS
4.2.1 Human
For our human pilot studies in Paper II and III, five healthy volunteers were recruited.
The subjects were two men and three women, age 30-45, taking no other medication or
naturopathic drugs, not having any disease or infection, not being pregnant or nursing
or with known sensitivity to statins. Each subject was given a single dose of 80 mg
simvastatin and 40 mg fluvastatin, at two separate time points with a two week washout
period in between. Serum was collected immediately before the tablets were taken and
two hours after the dose (time of Cmax for simvastatin) [148]. Urine was collected for 24
hours before and for 24 hours after administration and thereafter aliquoted and kept at
-80 °C until urinalysis.
For Paper IV we used patient samples from two different cohorts. Cohort 1included
stored RNA from liver biopsies from normocholesterolemic gallstone patients treated
with either fluvastatin 20 mg/day (N=5) or atorvastatin 80 mg/day (N=6) or placebo
(N=8) for two weeks. Fluvastatin 20 mg/day was used to achieve a low cholesterol
synthesis inhibition and atorvastatin 80 mg/day to achieve a high cholesterol synthesis
inhibition. From each subject stored plasma was used for the lathosterol och LDLmeasurements [149]. Cohort 2 included cDNA from 18 human livers belonging to the
human donor liver bank established at the Division of Clinical Pharmacology,
Karolinska University Hospital, Huddinge. In this cohort three subjects were treated
with statins and 15 had no statin-treatment according to the medical records. We had no
information about which statin or which dose the subjects were using.
4.2.2 Animals
A strain, in reference to rodents, is a group in which all members are as nearly as
possible genetically identical. In rats, this is accomplished through inbreeding. By
having this kind of population, it is possible to conduct experiments on the roles of
genes, or conduct experiments that exclude variations in genetics as a factor.
The Fischer 344 (F344) rat is one of the most commonly used rat strain in
carcinogenesis because of its genetically in-bred status, relatively small size, ease of
maintenance and sensitivity to various carcinogens and its relatively low spontaneous
tumor rate except for testicular Leydig cell tumors [150]. The rat model was originally
described by Solt and Farber [151] and was called “the resistant hepatocyte model”
implementing the appearance and selection of resistant hepatocytes with up-regulated
cellular defence. In Paper IV we used rat liver tissue from a study conducted earlier
in our laboratory, where male rats had been treated according to the chemical induced
hepatocarcinogenesis protocol described previously [38] and 5 rats had been given
27
C. Skogastierna
lovastatin in the diet for 5 weeks (dose approximate 13 mg/kg bodyweight/ day) and
5 rats standard chow diet (R36) for 5 weeks. Since rodents have a much quicker
metabolism of statins compared to humans this is likely to be an adequate statin dose
with an exposure similar to or less than that in humans. Similar or higher doses have
been used in previous works [152, 153].
4.3
EXPERIMENTAL METHODS
4.3.1 Quantitative real time PCR
Real-time polymerase chain reaction, also called quantitative real time polymerase
chain reaction (Q-PCR/qRT-PCR) or kinetic polymerase chain reaction (KPCR), is a
powerful technique which is used to amplify and simultaneously quantify a targeted
DNA molecule as the reaction progresses in real time. The quantity can be either an
absolute number of copies or a relative amount when normalized to DNA input or
additional normalizing genes. Prior to the PCR step, reverse transcription was
performed to obtain the first strand DNA, then TaqMan Probe-based assays were used
in the expression experiments in Papers I-IV. Briefly, the assays use a fluorogeniclabeled oligonucleotide probe to enable the detection of a specific PCR product as it
accumulates during PCR cycles. A reporter dye is incorporated on the 5´end and a
quencher dye on the 3´end of the probe. As long as the probe is intact, the proximity of
the quencher greatly reduces the reporter dye emitted fluorescence. If the target
sequence however is present, the probe anneals between primer sites and is cleaved by
the 5´nuclease activity of the DNA polymerase during the extension phase of the PCR
reaction. The reporter dye is then separated from the quencher, which increases the
reporter dye signal and also allows the primer extension to continue to the end of the
template strand. With each cycle additional reporter dye molecules are cleaved,
resulting in increased fluorescence intensity proportional to the amount of amplicon
produced. Thus the higher the starting copy number of the target sequence, the sooner
significant increase in fluorescence is observed, i.e. when the fluorescence increases
above the baseline and crosses the threshold [154]. The cycle at which this occurs is
called the Ct value and can be employed for quantification [155].
4.3.2 Promoter studies
In Paper I and II, to assess the genetic background for the variation observed in statin
induced regulation of PGIS mRNA in endothelial cells, we transfected HUVECs with
the PTGIS core promoter incorporated into a reporter construct. Briefly, the method
works as follows (see also Figure 10):
1. Amplification by PCR is carried out. We amplified PGIS promoter fragments,
including the cis-acting elements required for basal transcriptional activity
(approximately 300 bp), using human genomic DNA as template. The PCR products
were verified on an agarose gel by electrophoresis.
28
2. Next step is subcloning. The PCR product is cloned into a vector14 (here supplied
with single 3´-thymidine (T) overhangs, allowing PCR inserts to ligate efficiently
with the vector. The plasmid also contains topoisomerase I covalently bound to the
vector - referred to as "activated" vector) by cleaving the plasmid and the PCR product
from step 1, using restriction enzymes15, and then ligate them together.
3. We are now ready to perform transformation16 into competent17 bacteria and expand
them overnight on selective agar plates, on which only successfully transformed
bacteria are able to grow.
4. Isolated clones are selected for further expansion and subsequent purification of
plasmids. The plasmids are then cut by restriction enzymes and desired fragments
isolated by gel-purification. We also analyzed purified fragments from each clone for
verification of insert by sequence analysis and compared with PGIS official sequence
using BLAST18.
5. A second round of subcloning can now be executed, but this time we put our
promoter sequence into a construct containing an expression reporter downstream of
our insert. This results in a luciferase19-gene containing expression vector construct
driven by the PGIS promoter insert.
6. The complete vector is then expanded in bacteria through transformation, purified
and analysed as before.
7. Human umbilical endothelial cells (HUVECs) could then be transfected20 with our
expanded and purified reporter constructs. As expression control, renilla21-containing
plasmids were co-transfected into the HUVECs.
8. Eight hours after the transfection, statin or vehicle was added and cells were let grow
for 24 hours before harvest and analysis.
14
Vector: used in genetic engineering and are commonly used by molecular biologists to deliver genetic
material into cells. A vector is a type of plasmid, a DNA molecule that is separate from, and can replicate
independently of, the chromosomal DNA usually occurring naturally in bacteria, but is sometimes also
found in eukaryotic organisms.
15
Restriction enzymes: enzymes that cut DNA at specific recognition nucleotide known as restriction
sites.
16
Transformation: bacterial transformation may be referred to as a stable genetic change due to the
uptake of naked DNA (DNA without associated cells or proteins). Transformation occurs naturally in
some species of bacteria, but it can also be performed by artificial means in other cells.
17
Competent bacteria: refers to the state of being able to take up exogenous DNA from the environment.
18
BLAST: Basic Local Alignment Search Tool, an algorithm used in bioinformatics.
19
Luciferase: class of oxidative enzymes used in bioluminescence.
20
Transfection: the process of deliberately introducing nucleic acids into cells. The term is used notably
for non-viral methods in eukaryotic cells.
21
Renilla luciferase control reporter vectors constitutively express Renilla luciferase, cloned from the
anthozoan coelenterate Renilla reniformis (sea pansy), and thus provide an internal control value to which
expression of the experimental firefly reporter gene may be normalized.
29
C. Skogastierna
9. Luciferase activity was measured by the Dual-Luciferase Reporter Assay System
where the ratio between the PTGIS firefly luciferase signal and the control renilla
luciferase signal for each statin exposed sample was compared to the ratios for each
vehicle treated sample.
8. ”Experiment”
9. Measure Luciferase activity
Figure 10: Schematic principle of the transfection procedure. See text for details.
30
4.3.3 Enzyme Immunoassay
Enzyme immunoassay (EIA) or enzyme-linked immunosorbent assay (ELISA) is a
powerful type analytic biochemistry technique used for detecting and quantifying the
presence of an antigen in tissue homogenates, plasma or other body fluids [156, 157].
There are many variants including indirect, sandwich, reverse and competitive EIA.
The work in Papers I, II and III was performed using the competitive EIA method.
The principal protocol for competitive EIA (see Figure 11 and www.caymanchem.com)
utilizes an immunoplate, pre-coated with a secondary antibody and the non-specific
binding sites blocked. Sample containing an unknown amount of antigen is added to
the wells of the immunoplate, together with tracer (molecules of the analyte each
covalently attached to a molecule of acetylcholinesterase (AChE22 )) and antiserum
(primary antibody with a Fc fragment to which the secondary antibody can bind, and a
Fab fragment specific to the analyte). Any unbound reagents are washed away after
incubation and the plate is developed with Ellman’s Reagent which contains the
substrate of AChE. The product of this enzyme reaction is a distinct yellow color,
which absorbs strongly at 412 nm. The intensity of the color determined
spectrophotometrically, is proportional to the amount of analyte Tracer (labeled
antigen) bound to the well, which is inversely proportional to the amount of free
analyte (sample antigen) in the well during the incubation, i.e. in the sample added. In
other words, the labeled antigen now competes for primary antibody binding sites with
the sample antigen. The more antigen in the sample the less labeled antigen is retained
in the well and the weaker the signal.
Figure 11: Schematic principle of the EIA method.
22
AChE: a stable enzyme isolated from the electric eel, Electrophorus electricus, with a high turnover for
the hydrolysis of acetylthiocholine. The reaction produces thiocholine, which after non-enzymatic
convertion to 5-thio-2-nitrobenzoic acid has a strong absorbance at 412 nm.
31
C. Skogastierna
Interpretation of the signal produced in an immunoassay requires reference to a
calibrator that mimics the characteristics of the sample medium. For qualitative assays
the calibrators consist of a negative sample with no analyte and a positive sample
having the lowest concentration of the analyte that is considered detectable. For
quantitative measures additional calibrators with known analyte concentrations are also
included. Comparison of the assay response of a real sample to the assay responses
produced by the calibrators makes it possible to interpret the signal strength in terms of
the presence or concentration of analyte in the sample. The main limitation with EIA is
that due to the very small volume, even a small deviation of each reagent can have a
compounded effect. Therefore, samples should ideally be run in triplicates. Other
parameters should also be taken into account when using EIA; accuracy of the
measurement, detection limit and detectability range of the EIA and the specificity of
the antibodies [158]. Accuracy is especially crucial when determining concentration of
the samples. In the studies included in this thesis we therefore chose to use relative
concentrations, i.e. changes in detection between untreated controls and the samples.
4.3.3.1 Enzyme Immunoassay - PGI2
PGI2 is very short-lived. In the body it is quickly non-enzymatically hydrated to 6-keto
PGF1α and then converted to the major metabolite, 2,3-dinor-6-keto PGF1α (t1/2 = 30
minutes) [159-161], which is why we measured the contents of both metabolites in the
urine. Although 6-keto PGF1α is commonly measured in plasma and urine as an
estimate of prostacyclin synthesis, it should be noted that there may be more than one
source of PGI2 in these samples [162]. Urinary concentrations of 6-keto PGF1α are
confounded by the fact that some plasma prostacyclin (~14 %) is excreted into urine as
6-keto PGF1α and the remainder is of renal origin [162, 163]. These problems are
circumvented by measuring urinary 2,3-dinor-6-keto PGF1α as an indicator of systemic
PGI2 production. Moreover, in our studies we only use the relative changes and not
absolute values when interpreting and presenting the data. The EIAs for these
prostacyclin metabolites typically displays an IC50 (50 % B/B0) of about 40 pg/ml (6keto PGF1α) and 400 pg/ml (2,3-dinor-6-keto PGF1α), and a detection limit (80 % B/B0)
of approximately 6 pg/ml (6-keto PGF1α) and 100 pg/ml (2,3-dinor-6-keto PGF1α).
4.3.3.2 EIA – Thromboxane A2
In the body, the produced thromboxane A2 is rapidly hydrolyzed non-enzymatically to
form thromboxane B2 (TXB2). Most of the TXB2 measured in the plasma or urine of
healthy individuals is however due to ex vivo platelet activation or intra-renal
production [159]. Normal concentrations of circulating TXB2 are extremely low (1-2
pg/ml) and highly transient (t1/2 = 5-7 minutes), which is why we chose to assay a
metabolite of TXB2, 11-dehydro TXB2, not formed by platelets or the kidney and with
a longer circulating half-life of 45 minutes [164, 165]. In Paper II a competitive EIA
assay was used for quantification of 11-dehydro TXB2 in urine. Its measurement in
plasma or urine will give a time-integrated indication of TXA2 production and is
32
recommended to estimate TXA2 levels to circumvent measurement complications
associated with TXB2. The EIA typically displays an IC50 (50 % B/B0) value of 120
pg/ml and a detection limit (80 % B/B0) of approximately 34 pg/ml.
4.3.4 Western Blotting
The Western blot is an analytical technique used to detect specific proteins in a sample.
The technique uses gel electrophoresis to separate native or denatured proteins by the
size of the polypeptide or by the 3-D structure of the protein. Western blots allow
investigators to determine the molecular weight of a protein and to measure relative
amounts of the protein present in different samples. The general protocol (Figure 12)
starts with separation of the proteins and biotinylated molecular weight markers by gel
electrophoresis, usually SDS-PAGE23. The proteins are then transferred to a sheet of
nitrocellulose membrane, retaining the same pattern of separation they had on the gel.
Figure 12: Schematic principle of the Western Blot procedure. See text for detailed description.
23
SDS-PAGE: sodium dodecyl sulfate polyacrylamide gel electrophoresis separates proteins according to
their electrophoretic mobility, which is a function of the length of a polypeptide chain and its charge and
no other physical feature. SDS is an anionic detergent applied to protein sample to linearize proteins and
to impart a negative charge to linearized proteins. In most proteins, the binding of SDS to the polypeptide
chain imparts an even distribution of charge per unit mass, thereby resulting in a fractionation by
approximate size during electrophoresis.
33
C. Skogastierna
The blot is incubated with a generic protein (such as milk proteins) to bind to any
remaining sticky places on the nitrocellulose and block unspecific binding sites. A
primary antibody specific to the target protein is then added to the solution, let bind
during incubation and unbound antibody is then washed away. We then used a
chemiluminescent detection method based on a HRP-linked (horseradish peroxidase)
secondary antibody, which forms a complex with the primary antibody. The location of
the antibody complex is revealed by incubating it with specific substrate to generate a
light signal and the image is analysed by densitometry, which evaluates the relative
amount of protein staining and quantifies the results in terms of optical density. HRP
conjugates have a very high turnover rate, yielding good sensitivity with short reaction
times.
4.3.5 Colorimetric assay – detection of NO production
In biological fluids, NO undergoes a series of reactions with several molecules, the
end-products being nitrite (NO2-) and nitrate (NO3-). The relative proportion of these
two is variable and cannot be predicted with certainty, thus the best index of total NO
production is the sum of NO2- and NO3-. The fluorometric assay used in Paper I is a
convenient and accurate method for measurement of total NO2- and NO3- concentration
by firstly converse all nitrate to nitrite utilizing nitrate reductase, followed by 2,3diaminonaphthalene (DAN) and NaOH. DAN is then converted to the fluorescent
product, 1(H)-naphthotriazole. Measurement of this compound determines the NO2concentration [166].
4.3.6 LC-MS/MS
Liquid chromatography – mass spectrometry (LC-MS) is a technique in analytical
chemistry that combines the physical separation capabilities of liquid chromatography
(or HPLC24) with the mass analysis capabilities of mass spectrometry (MS25). LC-MS
is a powerful technique used for many applications, having very high sensitivity and
selectivity, and is generally used for the detection and potential identification of
compounds in a complex mixture in the presence of other chemicals. The major
advantage MS has is the use of tandem MS-MS, also known as MS/MS or MS2, where
the detector may be programmed to select certain ions to fragment and further separate
[167].
Sample concentrations of simvastatin, simvastatin-acid (SIM-OH) and fluvastatin in
serum from the healthy volunteers and from simvastatin or fluvastatin incubated HAEC
in Paper III, were measured by a standard LC-MS/MS method previously developed
for at our department. Briefly, sample preparation was based on pH-controlled solid
24
HPLC is a common chromatographic technique used to separate a mixture of compounds in analytical
chemistry and biochemistry with the purpose of identifying, quantifying and purifying the individual
components of the mixture.
25
MS is a powerful technique where the sample molecules are ionized and the mass-to-charge ratio of
charged particles or molecule fragments is measured.
34
phase extraction followed by evaporation under nitrogen and subsequent reconstitution.
Subsequent analysis was performed on a reversed-phase column with a triple
quadrupole mass spectrometer as detector and quantification was calculated on
analyte/internal standard peak area ratios. The limit of detection was 0.02 ng/mL.
4.3.7 Myographic readings
A myograph is any device used to measure the force produced by a muscle when under
contraction and can be used to study the velocity and intensity of muscular contraction.
In Paper I ex vivo experiments were conducted on vessels isolated from fat biopsies
obtained from ten healthy normotensive pregnant women (two nulliparous26). Using a
stereomicroscope, one or more subcutaneous arteries of similar size, internal diameter
of 203±8 µm, were dissected and immediately placed in ice cold physiological salt
solution. The arterial vessel rings were mounted on two parallel stainless steel wires, 25
m in diameter, in organ baths of a four-channel wire myograph filled with KrebsRinger physiological salt solution continuously gassed with 95 % O2 / 5 % CO2 at a
temperature of 37 °C. One pin was connected to a force transducer and the other to a
micrometer screw for length adjustment.
The vessels were preconstricted with norepinephrine, NE, a catecholamine with
multiple roles but here acting through α-adrenergic receptor activation of the vascular
smoth muscle cells. The concentration added was sufficient to evoke a sustained, steady
contraction before adding cumulatively concentrations of fluvastatin (10-7 - 10-4 mol/L,
log unit steps). Failure to respond to NE in the freshly isolated vessels excluded the
preparations from further experimentation. Concentration-response curves were in this
way obtained prior to and after incubation with either N-nitro-L-arginine methyl ester
(L-NAME) or indomethacin. L-NAME is an inhibitor of the enzyme endothelial NO
synthase, eNOS, and thus reduces the cellular formation of cGMP. Indomethacin is a
non-steroidal anti-inflammatory drug, nonselectively inhibiting COX-1 and COX-2,
which are enzymes responsible for formation of the prostacyclin precursor PGH2 in
endothelial cells.
In order to figure out the relative contribution of eNOS and COX products to the
fluvastatin-induced relaxation, their respective inhibitors were added alone or in
combination. The force (mN) developed per length (mm) of artery segment during
application of each concentration of vasoactive compound was calculated. All absolute
measurements were corrected for the baseline force developed by the arteries. The
relaxation to fluvastatin was calculated as percentage of reduction of the active force at
the stable plateau level. The contractions and concentration-response curves were then
compared before and after incubation with the two different pharmacological inhibitors.
26
Nulliparous refers to a woman who has never completed a pregnancy beyond 20 weeks and never
given birth.
35
C. Skogastierna
5 RESULTS AND DISCUSSION
5.1 GENERAL COMMENTS
Notably, many previous studies in vitro claiming mechanistic insights behind
pleiotropic effects of statins have used concentrations 1000-fold higher than those
detected in human plasma [168]. In the studies of this thesis much lower, clinically
relevant concentrations of simvastatin and fluvastatin, were used in our in vitro
experiments. Also, the intracellular concentrations, analyzed by means of LC-MS/MS,
of statins in our cultivated cells were in the same range as the plasma concentrations of
statins of our human subjects (reported in Paper III). Further, when testing cell
viability for concentrations higher than used in this work, 10 µM, the cells showed
signs of decreased membrane integrity by retaining dye in the viability test, which was
another reason for us to excluded concentrations above 1.0 µM.
Another intention with this work was to use time points that are clinically relevant.
Since statins are usually therapeutically administrated every 24 h, we chose this as time
point for our studies. One can argue that when doing transcriptional studies, the
information on the time profile is of interest and by only testing for 24 h we may miss
the acute effects on the transcription. But since we here not only assess the genetic
effects but also the phenotype consequences (i.e. effect on prostacylin release) we
decided to only include 24 h.
I have also received the question why we have not extended and/or verified the effects
of the statins on PGI2 generation by ECs using different models, i.e. laminar shear
stress that would mimic the flow of blood in the vessels and/or in response to an
inflammatory stimulator like IL1-β. I cannot but agree, these two situations would be
very valuable to add to the studies. The models are commonly used to assess the
protective effects of compounds and to stimulate an atherosclerotic (inflammatory)
environment. But the ultimate model is of course to study humans, and since we
confirmed our findings in healthy volunteers, we considered these extra in vitro models
not to be required in this work. I pass this task on to my successor PhD student, and the
exciting job to study these effects in statin patients.
Regarding the choice of different doses of simvastatin (80 mg) and fluvastatin (40 mg)
in the in vivo study, the rationale behind this was that we aimed to study both a
commonly given maximum dose of statin and a commonly given medium dose of
statin. 80 mg fluvastatin is approved by the Swedish Medical Products Agency
(Läkemedelsverket) to be prescribed but is extremely rare.
36
5.2
PAPER I: BENEFICIAL VASOACTIVE ENDOTHELIAL EFFECTS OF
FLUVASTATIN: FOCUS ON PROSTACYCLIN AND NITRIC OXIDE
We show in Study I that fluvastatin is a modulator of vascular tone in human small
arteries, most likely via acute and possibly also prolonged increased formation and
release of endothelium-derived relaxing factors such as NO and PGI2, since inhibitors
of both eNOS and COX significantly decreased relaxation in response to fluvastatin. A
robust concentration dependent relaxation was produced with fluvastatin, reaching a
maximum within three minutes. Fluvastatin-induced relaxation was reproducible and
did not deteriorate after repeated application. Moreover, we showed that fluvastatin
induces significant transcriptional and translational up-regulation of PGIS and eNOS,
with increased cellular production of PGI2 and NO in EC cultures, suggesting that this
compound may have beneficial effects on endothelial maintenance in vivo. Relaxation
due to fluvastatin administration in the resistance vasculature may associate with
reduced peripheral resistance and increased blood flow to target organs. The tone of
resistance arteries is considered to be critical for blood pressure control. To our
knowledge this is a first study that reports an acute relaxant effect of a statin –
fluvastatin - in isolated small human arteries. Interestingly, preliminary data using the
same technique, protocol and same type of material as in Paper I, but incubating with
atorvastatin, show no effect on vascular reactivity.
As discussed in the methodological considerations section, endothelial cells vary in
morphology and functions according to the type and size of the associated vessel. The
works presented in this thesis therefore involve endothelial cells from two different
locations in the body; aorta (HAEC) and umbilical cord (HUVEC), both cell types
being commonly used for studies of the vascular endothelium. It is important to note
that although HUVECs have venous features, the umbilical cord vein has the
physiological role of conveying oxygenated, nutrient-rich “arterial blood” from the
placenta to the foetus. In fact, umbilical cord veins have long been used in clinical
arterial transplantation [169].
Regarding patient group for the ex vivo experiments, one might question the rationale
for choosing pregnant women and how to approach effects of pregnancy sex hormones
- would it not be more accurate to use samples from men having abdominal surgery?
Indeed, other patients groups are of interest, however at the time for Study I it was
not possible to get such biopsies from e.g. males with normal or altered lipid profile.
Furthermore, normal pregnancy is associated with significant changes in serum lipids
(a shift towards small, dense LDL subfractions, raised triacylglycerols and
cholesterol) and by the third trimester most women have a lipid profile which would
be considered highly atherogenic in the non-pregnant state. This undoubtedly
represents a transient disturbance which reverts to normal after delivery, and is
related to the maintenance of nutrient fuel to the mother and fetus. Therefore, it might
be anticipated that vessels from normal pregnant women might represent a good
model to test the direct effects of fluvastatin on vascular function. It is well known
that sex hormones can affect vascular reactivity, but since we have worked with
isolated arteries in conditions when tissue was kept out from organism's environment,
37
C. Skogastierna
ex vivo, for several hours the acute modifying effects of hormones can be neglected.
Also, in Study I, the aim was to show the primary vascular effect of fluvastatin with
subsequent clarification of the contribution of endothelium-derived factors to
fluvastatin-induced responses of resistance arteries. With such an aim in mind we
withdrew our attention from possible modifying effects of pregnancy hormones.
5.3
PAPER II: INFLUENCE OF SIMVASTATIN ON THE THROMBOXANE
AND PROSTACYCLIN PATHWAYS, IN VITRO AND IN VIVO
In contrast to Paper I which concerns fluvastatin, the HMG-CoA reductase inhibitor
simvastatin, studied in Paper II, shows a potentially unfavorable alteration of the
vascular endothelium both in vivo and in vitro. After treating endothelial cells at
clinically relevant concentrations of simvastatin, the cells were shown to decrease their
production and release of PGI2. Addition of mevalonic acid lactone, a precursor of
cholesterol, reverted the effects of simvastatin on PGI2 release in ECs, indicating that
this effect is mevalonate dependent. Also, simvastatin administrated as a single dose to
healthy volunteers was shown to significantly increase urinary thromboxane A2 (TXA2)
levels, which may result in a shift of the balance between PGI2 and TXA2, favoring the
thromboxane pathway. Uncoupling of this balance could have pathophysiological
implications by promoting a prothrombotic state in the blood vessels as discussed in
Paper II. These findings add novel insight in the field of pleiotropic effects of statins
and provide some insight for functional differences among statins.
As a drug class, statins are considered by clinicians to be useful to their patients but
these data may question the effects of statins on health and raise the question of
thorough comparative studies on secondary vascular effects of statins.
One of the aims with Paper II was to compare the effect on PGI2 metabolism after
exposure to fluvastatin, studied in Paper I, with exposure to the in Europe more
commonly prescribed simvastatin. The majority of the in vitro experiments in these two
papers are directly comparable with each other. This is for example why we in Paper
II chose to include the PTGIS promoter activity studies performed in HUVEC only,
although the transcriptional effect on PTGIS seemed more pronounced in HAEC.
Unfortunately, the transfection method was for unknown reasons not successful in the
HAEC. Being primary cells make them more similar to the in vivo situation, but it also
renders them more sensitive to chemical modifications than cell lines.
On the subject of presenting and discussing the data from the human subjects, the
TXA2/PGI2 biosynthesis ratio is commonly used in the literature to visualize balance
changes of these two important metabolites. An abnormal TXA2/PGI2 ratio may
predispose affected patients to for example thrombosis. Also, the TXA2/PGI2 balance
is particularly critical in the regulation of maternal and fetal vascular function during
pregnancy and in the newborn. An increase in the ratio in the maternal, fetal and
neonatal circulation may contribute to preeclampsia, intrauterine growth restriction and
38
persistent pulmonary hypertension of the newborn, respectively [170]. On the other
hand, increased PGI2 activity may contribute to patent ductus arteriosus27 and
intraventricular hemorrhage in premature newborns [171].
Recent studies have shown that urinary metabolites of TXA2 and PGI2, constitute
unique markers of the activation and/or interaction between platelets and vascular
cells. Such an approach reflects the in vivo production of these mediators but has the
advantage of circumventing the artifactual production of eicosanoids occurring during
blood or tissue sampling. There are other arachidonic acid metabolites of interest that
are active and affected in the vasculature, but these are two of the most important, being
abundant, potent and having contrasting effects.
Also worth highlighting is the seeming dependence on the mevalonate - HMG-CoA
reductase pathway for the actions of simvastatin reported in study II, since addition of
mevalonate abolished the reduction of PGI2 synthesis in HAECs. Mounting
experimental evidence suggests that inhibition of the isoprenoids by statins might
explain the clinical observations that statins improve cardiovascular outcomes, even in
subjects with atherosclerosis and normal cholesterol levels [172]. However, these basic
observations have not been fully translated into humans and may be challenged by our
findings of a simvastatin mediated perturbation of the balance between the
vasoregulatory TXA2 and PGI2 pathways with a potentially negative effect on the
vascular homeostasis. It should also be noted that statins usually in the clinical situation
are used in combination with low doses of acetylsalicylic acid, which could influence
the levels of TXA2, as described in section 2.4.3.3, and perhaps the weight of our
findings.
5.4
PAPER III: ANTI-OXIDATIVE EFFECTS OF STATINS ON VASCULAR
ENDOTHELIUM
Although statins in the last years have been acknowledged for their range of often
beneficial pleiotropic effects, particularly relevant to cardiovascular disease including
improved endothelial function and reduced oxidative stress, very sparse data on how
statins affect the anti-oxidative status of the vascular endothelium are to be found. Our
aim with Paper III is thus to provide additional information and hopefully to shed
some light on the complex processes of cellular oxidative stress. The same cellular
model systems as in Paper I and II was used, cells were exposed in the same way to
either fluvastatin or simvastatin, and the expression pattern of central oxidative stress
defence enzyme genes (SOD-1, TXN, TrxR1, GPx4 and Cat) and the generation of
ROS in human vascular ECs was assessed. However, in order to estimate a time for
maximum ROS generation, which does not necessarily parallel the expression of the
enzymes included in the study, three different time points were studied. Moreover, the
effect on oxidative capacity in vivo was analysed in urine after statin administration, a
single dose of simvastatin (80mg) or fluvastatin (40mg), to healthy volunteers.
27
Ductus arteriosus ia a congenital disorder in the heart wherein a neonate's ductus arteriosus, a blood
vessel connecting the pulmonary artery to the aortic arch, fails to close after birth.
39
C. Skogastierna
The results from Study III indicate that the effects of statins may also here be
compound specific and could have major impact on the vascular endothelial oxidative
stress status. Analogous to Study I and II, the two statins were shown to have different
impact on the mRNA expression of the investigated genes. Simvastatin significantly
down-regulated the expression of all genes tested, whereas for fluvastatin no clear trend
was observed. Also the levels of intracellular reactive oxygen species activity in vitro
decreased after exposure to fluvastatin but not to the same extent for simvastatin. A
small but significant increase in anti-oxidative capacity was observed in urine after
fluvastatin but not simvastatin administration compared to before statin intake, which is
in accordance with our in vitro results, i.e. that FLU seems to have a less undesirable
effect on the expression on the anti-oxidative enzymes.
As discussed more thoroughly in Paper III, the antioxidative capacity of fluvastatin
has been reported by others in other model systems, such as human aortic smooth
muscle cells [173] and on the plasma lipids of hyperlipidemic subjects [174]. This is
proposed to be a consequence of its unique structure compared to other statins, giving it
a free radical-scavenging activity against the superoxide anion and hydroxyl radical
[175, 176] that is independent of its HMG-CoA reductase inhibition capacity [177].
5.5
PAPER IV: STATINS INHIBIT EXPRESSION OF THIOREDOXIN
REDUCTASE 1 IN RAT AND HUMAN LIVER AND REDUCE TUMOUR
DEVELOPMENT
In Paper III we concluded that statins have an impact on the expression of the TrxR1
enzyme. Since this enzyme has been suggested to be a significant player in
carcinogenesis, we set out to expand our studies of this enzyme in relation to cancer
and statins, Paper IV. We show in this article that statin treatment decreases the
hepatic expression of TrxR1 in humans and rats. Further, a clear correlation between
inhibition of carcinogenesis and decreased TrxR1-mRNA levels in a rat model for liver
cancer was observed, making us postulate that a possible causal relationship between
statin-induced decrease in TrxR1expression and inhibition of carcinogenesis seems to
exist. Since the statins display a clear inhibition of TrxR1 independent of
carcinogenesis in our human material, we conclude that the reduced TrxR activity is
caused directly by the statins and not to a statin-induced reduction of nodule size.
These findings add insight to the field of possible anti-carcinogenic effects of statins, as
well as other side effects of statins. I also hope that these findings may invite larger
studies involving human subjects to further clarify the relationship between statins,
TrxR1 and carcinogenesis in man.
40
5.6 UNDISCLOSED AND UNPUBLISHED RESULTS
An initial aim with the thesis was to include all four of the most commonly prescribed
statins around the world, something I could not fully proceed with due to unforeseen
circumstances and the nature of science. This however means that there are some
results that are not finalized for publication but that I still mean to share.
5.6.1 Atorvastatin and rosuvastatin vs. expression of COX, PGIS and
eNOS
Similar effects on transcription and translation of PGIS were observed after exposure to
the other two statins, i.e. both atorvastatin and rosuvastatin increase the mRNA
expression of PGIS in HUVEC (Figure 13A). The mRNA expression however, did not
correlate with the PGI2 production (Figure 13B), probably due to inhibition of COX
activity. When assaying the activity of the COX enzymes in EC cultures, we found that
simvastatin, atorvastatin and rosuvastatin all interfered with the enzymes, inhibiting
approximately 90 % of the total COX activity. Possibly this could decrease the
production of PGH2 and depleting the cells of the substrate for PGIS, resulting in a
decrease in prostacyclin production. This might partly explain why the increase in
mRNA and protein does not correlate with product release.
A
41
C. Skogastierna
B
Relative change in 6KPG1Fα
2,50
2,00
1,50
ATV - MEV
ATV + MEV
1,00
ROS - MEV
ROS + MEV
0,50
0,00
0,0
0.01
(µM)
1.0
Figure 13: Additional HUVEC and HAEC analyses. A) mRNA expression in HUVEC exposed to
either rosuvastatin for 24 hours or 48 hours (ROS 24 and ROS 48, respectively) or atorvastatin for 24
hours or 48 hours (ATV 24 and ATV 48, respectively). B) 6-keto-PG1Fα (6KPG1Fα) release in HAEC
cell medium after treatment with rosuvastatin (ROS) or atorvastatin (ATV), alone (-MEV) or with
mevalonate 100 µM (+MEV).
5.6.2 Atorvastatin and rosuvastatin vs. PTGIS promoter activity
Apart from fluvastatin and simvastatin, we have also looked at the influence on PTGIS
promoter activity in PGIS core promoter transfected HUVECs exposed to 0.1 µM
atorvastatin, rosuvastatin or corresponding vehicle for 24 hours, using the same cloning
and transfection procedure as in Papers I and II. Atorvastatin exposed cells displayed a
significant twofold increase in promoter activity (P = 0.001), while exposure to
rosuvastatin indicated a slightly increased promoter activity although not significant
(Figure 14).
42
control
activity,
luciferase
of control
fold of
activity,fold
Luciferase
4
3
2
1
0
ATV
ROS
SIM
FLU
M annactivity
Whi in
tney
test
Figure 14: PTGIS promoter
PGIS core
promoter transfected HUVECs exposed to 0.1
P
val
ue
0.0011
µM atorvastatin (ATV), rosuvastatin (ROS) or corresponding vehicle for 24 hours.
The bars
Exact
or
approxi
m
ate
P
val
ue?
Gaussi
an Approxi m a
represent mean ± S.E.M., N=15. The luciferase expression was normalised to the transfection
efficiency
P valexpression
ue sum
m ary
by the control renilla luciferase
in each
sample and normalised against the**
mean of respective
control, set as 1.
P val ue
0.3183
Exact or approxi m ate P val ue?
P val ue sum m ary
Gaussi an Approxi m a
ns
P val
ue
0.0304
Atorvastatin
and
rosuvastatin vs. anti-oxidative stress
enzyme
Exact
or
approxi
m
ate
P
val
ue?
Gaussi
an Approxi m a
genes
val ue sum m ary
In addition to studyPhow
fluvastatin and simvastatin affects the mRNA* expression of
P val in
ue
0.0034
several enzymes involved
the defence against oxidative stress (Paper
III), the HAEC
Exact
or
approxi
m
ate
P
val
ue?
Gaussi
cells were also exposed to atorvastatin and rosuvastatin for 24 hours (figure 14). an
In Approxi m a
P val ue sum m ary
**
opposite to the other statins, rosuvastatin exert a significant increase in GPx4.
In agreement with fluvastatin and simvastatin, atorvastatin and rosuvastatin also
inhibits mRNA expression of catalase. Neither rosuvastatin or atorvastatin inhibits the
mRNA expression of TXN in HAEC. In fact simvastatin appears to be the only statin
that significantly inhibit the TXN mRNA level in HAEC. This is in agreement with our
now ongoing studies that are being performed in human hepatoma (HepG2) cells to
further assess the molecular mechanisms behind the statin induced inhibition on TrxR1
transcription. Preliminary results in HepG2 cells indicate that the statins inhibit TrxR1
to different extent, and that simvastatin exert highest inhibitory effects. The in vitro
findings in HAEC and HepG2 cells are not agreement with our in vivo results in Paper
IV, i.e. that atorvastatin inhibits the hepatic expression of TrxR1 in patients
administrated with atorvastatin for four weeks. The reason for this discrepancy may be
explained by the fact that the human subjects had been taking statins for a long period
time, whereas in the in vitro experiments, the cells have been exposed to a single dose
of statins.
5.6.3
43
C. Skogastierna
Figure 15: mRNA expression of oxidative stress enzyme genes in HAEC cells exposed to increasing
concentration (0.01-1 uM) of rosuvastatin (ROS) and atorvastatin (ATV) for 24 hours.
44
6 CONCLUSIONS
The main results obtained from these studies can be summarized as follows:
Fluvastatin is proposed a protective role of on the cardiovascular system,
particularly at the level of vascular endothelium since it up-regulates
transcription and translation of PGIS and eNOS in human vascular endothelial
cells, associated with an increase in cellular production of PGI2 and NO, and
induces rapid dilatation in isolated human arteries via contribution of
endothelium derived factors like NO and PGI2.
Simvastatin induces a potentially unfavorable alteration of the vascular
endothelial cells both in vivo and in vitro. Exposure to clinically comparable
concentrations of simvastatin decreased the production and release of PGI2 in
cultivated endothelial cells. Simvastatin was further shown to significantly
increase urinary TXA2 levels in vivo, which may result in a negative alteration
of the balance between PGI2 and TXA2.
Fluvastatin and simvastatin have different impact on vascular endothelial
oxidative stress status. Compared to simvastatin, fluvastatin seems beneficial
both regarding expression of anti-oxidative stress enzymes and reactive oxygen
species activity in vitro and anti-oxidative capacity in vivo.
Statin treatment decreases the hepatic expression of TrxR1 in humans and rats
which is relevant for suggested anti-carcinogenic effects of statins.
Overall, our results add to the conjecture that the impact on production of vascular
active substances may be significantly different among the statins, and thus the
consequences of statin exposure may not be drug class related but rather compound
specific, highlighting the importance of more comparative studies where several statins
are included.
45
C. Skogastierna
7 ACKNOWLEDGEMENTS
I would like to express my sincere gratitude to the following people, without whom I
could not have completed my PhD:
Lena Ekström, my main supervisor. We have had some fun during this time, haven´t
we? Our Japan trip still makes me laugh! Thank you for accepting me, first for a master
thesis project, giving me the first real glimpses of science, and later as a PhD student.
Under your supervision I have learned countless valuable things about research and
molecular biology. From the bottom of my heart, thank you for always having time for
me, always being supportive and for being that creative “doer”.
My co-supervisors Anders Rane, Linda Bergman-Björkhem and Erik Eliasson,
thank you for being great advisors, for sharing your experiences and knowledge along
the way, and being supportive.
Anders, for you extensive knowledge in clinical pharmacology, your excellent inputs
and good advice. I highly appreciate that you have always taken time for detailed
proof-reading of my material.
Linda, you have truly been that spark of energy that made this project take its final
form! I am truly grateful that you came into the picture and agreed to be a part of this
work. Thank you for always being positive and helpful, and being incredible fast with
feedback.
Erik, for you good advice and for being the “sensible one”, always thinking two rounds
and coming with invaluable thoughts and comments.
Janeric Seidegård, for being the helpful and supportive connection to the industry.
Thank you for the fun meetings and chats. I hope our collaboration will not stop here!
My gratitude to all co-authors for our successful collaboration.
Margit Ekström, I would not have been able to finish this work without you, you are
truly the goddess of paperwork! Thank you for always taking time when I have been in
need and for all the fun conversations and stories. Clin Pharm has not been the same
since you left.
Birgitta Ask, what would I have done without you? Thank you for your patience with
me in the lab and for sharing your valuable experience.
My roomies, (present) Emmanuel Strahm, Jenny Schulze, Maria Johansson, Eleni
Aklillu; (past) Roza Ghotbi, Sara Karlsson, Annika Alqvist and Maja Hotzen, for
all the non-scientific discussions, endless coffees, dinners, drinks and fun! Yassin
Ahmed and Jonas Lundmark, I count you into this category as well. Thanks for being
great friends and for being a blast!
Other past and present members of “plan 8”, the power ladies Lilleba Boman, Jolanta
Wiren and Margarita Mahindi, for being sweet and helpful.
46
To all you on “plan 6”, esprecially Tobias Bäckström (thanks for great music tips and
training talk, keep it up!), Jonatan Lindh, Marine Andersson, Annika Asplund,
Fadiea Al-Aieshy, Staffan Olsson, Nina Gårevik, Camilla Linder and Karin
Nilsson, for nice company during and off working hours.
Lars L Gustavsson, for your enthusiasm. It was fun and a good experience to start up
and run the journal club with you. I hope it will survive for many years!
My friends at Fysiologen, especially Thomas Gustavsson and Anna Strömberg, for
all the nice chats and laughs. Good luck with research and life my future colleauges!
My wonderful friends in science and in life, Karin Larsson, love you to pieces! I will
always and forever be grateful that “forskarskolan” brought us together Can´t
believe that we made it! Carolina Gustavsson, Britta Stensson and Kylie Foo, for the
awesome time and all the adventures in Tokyo! Carolina, my ENDOMET board buddy,
we were great representatives, weren´t we? You made some of my travels, both
scientific and non-scientific, really into something extra! Kylie, I will see you in NY!
Soon! I wish you all the best and hope our paths will keep on crossing in life and in
research.
My dear and lovely friends outside KI, Jessie Dahlström, Louise Brattström-Stolt,
Linda Kylberg, Frida Olofsson, Stina Erhardsson, Martin Krook, you have all kept
me updated with the real world, without you life would indeed be a much duller place!
You are the best! Jessie, for being a great friend from day one at Astra Zeneca! I really
look forward to all the adventures still to experience with you. Louise,for your warmth,
all “fikas” and for encouraging me to apply for Med School. Linda, the #1 bundle of
energy! Thanks for introducing me to the world of house music and real clubbing!
Frida, this journey really started with you, in Lund 2004. It would definitely not have
been the same without you! You are truly the strongest person I know. Stina, for always
being there with smiles and laughter. You brought lovely knasighet in my life for real!
Martin, you have made my time in Umeå. The best in so many ways! “Inga
begränsningar, tid och pengar är allt vi har!”
Magnus Hellsten, for always being there. You and your family mean a lot to me.
To my big and warm family, Sven-Bertil Skogastierna,Tina, Pontus, Diana,
Rickard; Janet Andersson, Lennart, Filip, Hanna. Although my research has not
always been very clear to you, you have always been supportive and cheered me on.
You are the best!
47
C. Skogastierna
8 REFERENCES
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
48
Virchow R (1956) Standpoints in Scientific Medicine, 1877. Bull Hist Med
30:537-43
Tobert JA (2003) Lovastatin and beyond: the history of the HMG-CoA
reductase inhibitors. Nat Rev Drug Discov 2:517-26
Duff GL and Mc MG (1951) Pathology of atherosclerosis. Am J Med 11:92108
Endo A (1992) The discovery and development of HMG-CoA reductase
inhibitors. J Lipid Res 33:1569-82
Endo A, Kuroda M and Tsujita Y (1976) ML-236A, ML-236B, and ML-236C,
new inhibitors of cholesterogenesis produced by Penicillium citrinium. J
Antibiot (Tokyo) 29:1346-8
Tonelli M, Lloyd A, Clement F, Conly J, Husereau D, Hemmelgarn B,
Klarenbach S, McAlister FA, Wiebe N and Manns B (2011) Efficacy of statins
for primary prevention in people at low cardiovascular risk: a meta-analysis.
CMAJ 183:E1189-202
Yeagle PL (1991) Modulation of membrane function by cholesterol. Biochimie
73:1303-10
Haines TH (2001) Do sterols reduce proton and sodium leaks through lipid
bilayers? Prog Lipid Res 40:299-324
Incardona JP and Eaton S (2000) Cholesterol in signal transduction. Curr Opin
Cell Biol 12:193-203
Intake of Calories and Selected Nutrients for the United States Population,
1999-2000, U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES
Centers for Disease Control and Prevention National Center for Health
Statistics.
Liscum L, Finer-Moore J, Stroud RM, Luskey KL, Brown MS and Goldstein
JL (1985) Domain structure of 3-hydroxy-3-methylglutaryl coenzyme A
reductase, a glycoprotein of the endoplasmic reticulum. J Biol Chem 260:52230
Hua X, Nohturfft A, Goldstein JL and Brown MS (1996) Sterol resistance in
CHO cells traced to point mutation in SREBP cleavage-activating protein. Cell
87:415-26
Yabe D, Brown MS and Goldstein JL (2002) Insig-2, a second endoplasmic
reticulum protein that binds SCAP and blocks export of sterol regulatory
element-binding proteins. Proc Natl Acad Sci U S A 99:12753-8
Yang T, Espenshade PJ, Wright ME, Yabe D, Gong Y, Aebersold R, Goldstein
JL and Brown MS (2002) Crucial step in cholesterol homeostasis: sterols
promote binding of SCAP to INSIG-1, a membrane protein that facilitates
retention of SREBPs in ER. Cell 110:489-500
Goldstein JL and Brown MS (1990) Regulation of the mevalonate pathway.
Nature 343:425-30
Wang X, Sato R, Brown MS, Hua X and Goldstein JL (1994) SREBP-1, a
membrane-bound transcription factor released by sterol-regulated proteolysis.
Cell 77:53-62
Gasic GP (1994) Basic-helix-loop-helix transcription factor and sterol sensor in
a single membrane-bound molecule. Cell 77:17-9
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
Espenshade PJ and Hughes AL (2007) Regulation of sterol synthesis in
eukaryotes. Annu Rev Genet 41:401-27
Vita JA, Yeung AC, Winniford M, Hodgson JM, Treasure CB, Klein JL, Werns
S, Kern M, Plotkin D, Shih WJ, Mitchel Y and Ganz P (2000) Effect of
cholesterol-lowering therapy on coronary endothelial vasomotor function in
patients with coronary artery disease. Circulation 102:846-51
Treasure CB, Klein JL, Weintraub WS, Talley JD, Stillabower ME, Kosinski
AS, Zhang J, Boccuzzi SJ, Cedarholm JC and Alexander RW (1995) Beneficial
effects of cholesterol-lowering therapy on the coronary endothelium in patients
with coronary artery disease. N Engl J Med 332:481-7
Santos AC and Lehmann R (2004) Germ cell specification and migration in
Drosophila and beyond. Curr Biol 14:R578-89
Istvan ES and Deisenhofer J (2001) Structural mechanism for statin inhibition
of HMG-CoA reductase. Science 292:1160-4
Hamelin BA and Turgeon J (1998) Hydrophilicity/lipophilicity: relevance for
the pharmacology and clinical effects of HMG-CoA reductase inhibitors.
Trends Pharmacol Sci 19:26-37
White CM (2002) A review of the pharmacologic and pharmacokinetic aspects
of rosuvastatin. J Clin Pharmacol 42:963-70
McTaggart F, Buckett L, Davidson R, Holdgate G, McCormick A, Schneck D,
Smith G and Warwick M (2001) Preclinical and clinical pharmacology of
Rosuvastatin, a new 3-hydroxy-3-methylglutaryl coenzyme A reductase
inhibitor. Am J Cardiol 87:28B-32B
Holdgate GA, Ward WH and McTaggart F (2003) Molecular mechanism for
inhibition of 3-hydroxy-3-methylglutaryl CoA (HMG-CoA) reductase by
rosuvastatin. Biochem Soc Trans 31:528-31
Igel M, Sudhop T and von Bergmann K (2002) Pharmacology of 3-hydroxy-3methylglutaryl-coenzyme A reductase inhibitors (statins), including
rosuvastatin and pitavastatin. J Clin Pharmacol 42:835-45
Vaughan CJ and Gotto AM, Jr. (2004) Update on statins: 2003. Circulation
110:886-92
Corsini A, Bellosta S, Baetta R, Fumagalli R, Paoletti R and Bernini F (1999)
New insights into the pharmacodynamic and pharmacokinetic properties of
statins. Pharmacol Ther 84:413-28
Malmstrom RE, Ostergren J, Jorgensen L and Hjemdahl P (2009) Influence of
statin treatment on platelet inhibition by clopidogrel - a randomized comparison
of rosuvastatin, atorvastatin and simvastatin co-treatment. J Intern Med
266:457-66
McTaggart F (2003) Comparative pharmacology of rosuvastatin. Atheroscler
Suppl 4:9-14
Niemi M (2010) Transporter pharmacogenetics and statin toxicity. Clin
Pharmacol Ther 87:130-3
Link E, Parish S, Armitage J, Bowman L, Heath S, Matsuda F, Gut I, Lathrop
M and Collins R (2008) SLCO1B1 variants and statin-induced myopathy--a
genomewide study. N Engl J Med 359:789-99
Robey RW, To KK, Polgar O, Dohse M, Fetsch P, Dean M and Bates SE
(2009) ABCG2: a perspective. Adv Drug Deliv Rev 61:3-13
Lee E, Ryan S, Birmingham B, Zalikowski J, March R, Ambrose H, Moore R,
Lee C, Chen Y and Schneck D (2005) Rosuvastatin pharmacokinetics and
pharmacogenetics in white and Asian subjects residing in the same
environment. Clin Pharmacol Ther 78:330-41
49
C. Skogastierna
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
50
Ieiri I, Suwannakul S, Maeda K, Uchimaru H, Hashimoto K, Kimura M, Fujino
H, Hirano M, Kusuhara H, Irie S, Higuchi S and Sugiyama Y (2007) SLCO1B1
(OATP1B1, an uptake transporter) and ABCG2 (BCRP, an efflux transporter)
variant alleles and pharmacokinetics of pitavastatin in healthy volunteers. Clin
Pharmacol Ther 82:541-7
Keskitalo JE, Pasanen MK, Neuvonen PJ and Niemi M (2009) Different effects
of the ABCG2 c.421C>A SNP on the pharmacokinetics of fluvastatin,
pravastatin and simvastatin. Pharmacogenomics 10:1617-24
(1994) Randomised trial of cholesterol lowering in 4444 patients with coronary
heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet
344:1383-9
Baigent C, Keech A, Kearney PM, Blackwell L, Buck G, Pollicino C, Kirby A,
Sourjina T, Peto R, Collins R and Simes R (2005) Efficacy and safety of
cholesterol-lowering treatment: prospective meta-analysis of data from 90,056
participants in 14 randomised trials of statins. Lancet 366:1267-78
Pfefferkorn JA, Song Y, Sun KL, Miller SR, Trivedi BK, Choi C, Sorenson RJ,
Bratton LD, Unangst PC, Larsen SD, Poel TJ, Cheng XM, Lee C, Erasga N,
Auerbach B, Askew V, Dillon L, Hanselman JC, Lin Z, Lu G, Robertson A,
Olsen K, Mertz T, Sekerke C, Pavlovsky A, Harris MS, Bainbridge G, Caspers
N, Chen H and Eberstadt M (2007) Design and synthesis of hepatoselective,
pyrrole-based HMG-CoA reductase inhibitors. Bioorg Med Chem Lett
17:4538-44
Baigent C, Blackwell L, Emberson J, Holland LE, Reith C, Bhala N, Peto R,
Barnes EH, Keech A, Simes J and Collins R (2010) Efficacy and safety of more
intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000
participants in 26 randomised trials. Lancet 376:1670-81
Ray KK, Seshasai SR, Erqou S, Sever P, Jukema JW, Ford I and Sattar N
(2010) Statins and all-cause mortality in high-risk primary prevention: a metaanalysis of 11 randomized controlled trials involving 65,229 participants. Arch
Intern Med 170:1024-31
Mills EJ, O'Regan C, Eyawo O, Wu P, Mills F, Berwanger O and Briel M
(2011) Intensive statin therapy compared with moderate dosing for prevention
of cardiovascular events: a meta-analysis of >40 000 patients. Eur Heart J
32:1409-15
Taylor F, Ward K, Moore TH, Burke M, Davey Smith G, Casas JP and
Ebrahim S (2011) Statins for the primary prevention of cardiovascular disease.
Cochrane Database Syst Rev CD004816
Roberts WC (1997) The rule of 5 and the rule of 7 in lipid-lowering by statin
drugs. Am J Cardiol 80:106-7
Abramson J and Wright JM (2007) Are lipid-lowering guidelines evidencebased? Lancet 369:168-9
Hippisley-Cox J and Coupland C (2010) Unintended effects of statins in men
and women in England and Wales: population based cohort study using the
QResearch database. BMJ 340:c2197
Ravnskov U, Rosch PJ, Sutter MC and Houston MC (2006) Should we lower
cholesterol as much as possible? BMJ 332:1330-2
Baker SK and Tarnopolsky MA (2005) Statin-associated neuromyotoxicity.
Drugs Today (Barc) 41:267-93
Pedersen TR, Faergeman O, Kastelein JJ, Olsson AG, Tikkanen MJ, Holme I,
Larsen ML, Bendiksen FS, Lindahl C, Szarek M and Tsai J (2005) High-dose
atorvastatin vs usual-dose simvastatin for secondary prevention after
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
62.
63.
64.
65.
66.
67.
68.
69.
myocardial infarction: the IDEAL study: a randomized controlled trial. JAMA
294:2437-45
Armitage J, Bowman L, Wallendszus K, Bulbulia R, Rahimi K, Haynes R,
Parish S, Peto R and Collins R (2010) Intensive lowering of LDL cholesterol
with 80 mg versus 20 mg simvastatin daily in 12,064 survivors of myocardial
infarction: a double-blind randomised trial. Lancet 376:1658-69
Wettermark B and Hjemdahl P (2001) [Can we afford good cholesterol
lowering therapy? Budgeting of statin costs versus medical needs in the county
of Stockholm]. Lakartidningen 98:5472-3, 5476-8, 5481-3
Andrade SE, Walker AM, Gottlieb LK, Hollenberg NK, Testa MA, Saperia
GM and Platt R (1995) Discontinuation of antihyperlipidemic drugs--do rates
reported in clinical trials reflect rates in primary care settings? N Engl J Med
332:1125-31
Ando H, Tsuruoka S, Yamamoto H, Takamura T, Kaneko S and Fujimura A
(2004) Effects of pravastatin on the expression of ATP-binding cassette
transporter A1. J Pharmacol Exp Ther 311:420-5
Bergman U, Anderssen M, Vaccheri A, Larsen J and Montanaro N (1999)
Marked differences in lipid-lowering drug use in Bologna, Italy and Funen,
Denmark. Eur Heart J 20:1135
Larsen J, Vaccheri A, Andersen M, Montanaro N and Bergman U (2000) Lack
of adherence to lipid-lowering drug treatment. A comparison of utilization
patterns in defined populations in Funen, Denmark and Bologna, Italy. Br J Clin
Pharmacol 49:463-71
Hayward RA, Krumholz HM, Zulman DM, Timbie JW and Vijan S (2010)
Optimizing statin treatment for primary prevention of coronary artery disease.
Ann Intern Med 152:69-77
Davignon J (2004) Beneficial cardiovascular pleiotropic effects of statins.
Circulation 109:III39-43
Rang HP and Dale MM, Pharmacology. 2nd ed1991, Edinburgh ; New York:
Churchill Livingstone. 955 p.
Ross R (1995) Cell biology of atherosclerosis. Annu Rev Physiol 57:791-804
Kunsch C and Medford RM (1999) Oxidative stress as a regulator of gene
expression in the vasculature. Circ Res 85:753-66
Gibbons GH and Dzau VJ (1996) Molecular therapies for vascular diseases.
Science 272:689-93
Ross R (1999) Atherosclerosis--an inflammatory disease. N Engl J Med
340:115-26
Arnaud C, Veillard NR and Mach F (2005) Cholesterol-independent effects of
statins in inflammation, immunomodulation and atherosclerosis. Curr Drug
Targets Cardiovasc Haematol Disord 5:127-34
Lazar HL, Bao Y, Zhang Y and Bernard SA (2003) Pretreatment with statins
enhances myocardial protection during coronary revascularization. J Thorac
Cardiovasc Surg 125:1037-42
Wolfrum S, Jensen KS and Liao JK (2003) Endothelium-dependent effects of
statins. Arterioscler Thromb Vasc Biol 23:729-36
Ebrahim S and Smith GD (2000) Statins and risk of coronary heart disease.
Jama 283:2935-6
Harrison DG (1997) Endothelial function and oxidant stress. Clin Cardiol 20:II11-7
Libby P and Ridker PM (2004) Inflammation and atherosclerosis: role of Creactive protein in risk assessment. Am J Med 116 Suppl 6A:9S-16S
51
C. Skogastierna
70.
71.
72.
73.
74.
75.
76.
77.
78.
79.
80.
81.
82.
83.
84.
85.
52
Rosenson RS and Hurt-Camejo E (2012) Phospholipase A2 enzymes and the
risk of atherosclerosis. Eur Heart J
Albert CM, Ma J, Rifai N, Stampfer MJ and Ridker PM (2002) Prospective
study of C-reactive protein, homocysteine, and plasma lipid levels as predictors
of sudden cardiac death. Circulation 105:2595-9
Moreno PR, Falk E, Palacios IF, Newell JB, Fuster V and Fallon JT (1994)
Macrophage infiltration in acute coronary syndromes. Implications for plaque
rupture. Circulation 90:775-8
Verma S, Wang CH, Li SH, Dumont AS, Fedak PW, Badiwala MV, Dhillon B,
Weisel RD, Li RK, Mickle DA and Stewart DJ (2002) A self-fulfilling
prophecy: C-reactive protein attenuates nitric oxide production and inhibits
angiogenesis. Circulation 106:913-9
Khanapure SP, Garvey DS, Janero DR and Letts LG (2007) Eicosanoids in
inflammation: biosynthesis, pharmacology, and therapeutic frontiers. Curr Top
Med Chem 7:311-40
Kleemann R, Bureeva S, Perlina A, Kaput J, Verschuren L, Wielinga PY, HurtCamejo E, Nikolsky Y, van Ommen B and Kooistra T (2011) A systems
biology strategy for predicting similarities and differences of drug effects:
evidence for drug-specific modulation of inflammation in atherosclerosis. BMC
Syst Biol 5:125
Bustos C, Hernandez-Presa MA, Ortego M, Tunon J, Ortega L, Perez F, Diaz
C, Hernandez G and Egido J (1998) HMG-CoA reductase inhibition by
atorvastatin reduces neointimal inflammation in a rabbit model of
atherosclerosis. J Am Coll Cardiol 32:2057-64
Aikawa M, Rabkin E, Sugiyama S, Voglic SJ, Fukumoto Y, Furukawa Y,
Shiomi M, Schoen FJ and Libby P (2001) An HMG-CoA reductase inhibitor,
cerivastatin, suppresses growth of macrophages expressing matrix
metalloproteinases and tissue factor in vivo and in vitro. Circulation 103:276-83
Bellosta S, Via D, Canavesi M, Pfister P, Fumagalli R, Paoletti R and Bernini F
(1998) HMG-CoA reductase inhibitors reduce MMP-9 secretion by
macrophages. Arterioscler Thromb Vasc Biol 18:1671-8
Fukumoto Y, Libby P, Rabkin E, Hill CC, Enomoto M, Hirouchi Y, Shiomi M
and Aikawa M (2001) Statins alter smooth muscle cell accumulation and
collagen content in established atheroma of watanabe heritable hyperlipidemic
rabbits. Circulation 103:993-9
Williams JK, Sukhova GK, Herrington DM and Libby P (1998) Pravastatin has
cholesterol-lowering independent effects on the artery wall of atherosclerotic
monkeys. J Am Coll Cardiol 31:684-91
Niwa S, Totsuka T and Hayashi S (1996) Inhibitory effect of fluvastatin, an
HMG-CoA reductase inhibitor, on the expression of adhesion molecules on
human monocyte cell line. Int J Immunopharmacol 18:669-75
Mehta JL, Rasouli N, Sinha AK and Molavi B (2006) Oxidative stress in
diabetes: a mechanistic overview of its effects on atherogenesis and myocardial
dysfunction. Int J Biochem Cell Biol 38:794-803
Dalton TP, Shertzer HG and Puga A (1999) Regulation of gene expression by
reactive oxygen. Annu Rev Pharmacol Toxicol 39:67-101
Kamata H and Hirata H (1999) Redox regulation of cellular signalling. Cell
Signal 11:1-14
Thomas EL, Lehrer RI and Rest RF (1988) Human neutrophil antimicrobial
activity. Rev Infect Dis 10 Suppl 2:S450-6
86.
87.
88.
89.
90.
91.
92.
93.
94.
95.
96.
97.
98.
99.
100.
101.
102.
Nordberg J and Arner ES (2001) Reactive oxygen species, antioxidants, and the
mammalian thioredoxin system. Free Radic Biol Med 31:1287-312.
Gromer S, Urig S and Becker K (2004) The thioredoxin system--from science
to clinic. Med Res Rev 24:40-89
Yamawaki H, Haendeler J and Berk BC (2003) Thioredoxin: a key regulator of
cardiovascular homeostasis. Circ Res 93:1029-33
May JM, Mendiratta S, Hill KE and Burk RF (1997) Reduction of
dehydroascorbate to ascorbate by the selenoenzyme thioredoxin reductase. J
Biol Chem 272:22607-10
Arner ES, Nordberg J and Holmgren A (1996) Efficient reduction of lipoamide
and lipoic acid by mammalian thioredoxin reductase. Biochem Biophys Res
Commun 225:268-74
Sun X, Dobra K, Bjornstedt M and Hjerpe A (2000) Upregulation of 9 genes,
including that for thioredoxin, during epithelial differentiation of mesothelioma
cells. Differentiation 66:181-8.
Berggren M, Gallegos A, Gasdaska JR, Gasdaska PY, Warneke J and Powis G
(1996) Thioredoxin and thioredoxin reductase gene expression in human
tumors and cell lines, and the effects of serum stimulation and hypoxia.
Anticancer Res 16:3459-66.
Kumar S and Holmgren A (1999) Induction of thioredoxin, thioredoxin
reductase and glutaredoxin activity in mouse skin by TPA, a calcium ionophore
and other tumor promoters. Carcinogenesis 20:1761-7
Holmgren A (1985) Thioredoxin. Annu Rev Biochem 54:237-71
Holmgren A (1989) Thioredoxin and glutaredoxin systems. J Biol Chem
264:13963-6
Hirota K, Murata M, Sachi Y, Nakamura H, Takeuchi J, Mori K and Yodoi J
(1999) Distinct roles of thioredoxin in the cytoplasm and in the nucleus. A twostep mechanism of redox regulation of transcription factor NF-kappaB. J Biol
Chem 274:27891-7
Nakamura H, De Rosa S, Roederer M, Anderson MT, Dubs JG, Yodoi J,
Holmgren A and Herzenberg LA (1996) Elevation of plasma thioredoxin levels
in HIV-infected individuals. Int Immunol 8:603-11
Ericson ML, Horling J, Wendel-Hansen V, Holmgren A and Rosen A (1992)
Secretion of thioredoxin after in vitro activation of human B cells. Lymphokine
Cytokine Res 11:201-7
Rubartelli A, Bajetto A, Allavena G, Wollman E and Sitia R (1992) Secretion
of thioredoxin by normal and neoplastic cells through a leaderless secretory
pathway. J Biol Chem 267:24161-4
Nakamura H, Masutani H, Tagaya Y, Yamauchi A, Inamoto T, Nanbu Y, Fujii
S, Ozawa K and Yodoi J (1992) Expression and growth-promoting effect of
adult T-cell leukemia-derived factor. A human thioredoxin homologue in
hepatocellular carcinoma. Cancer 69:2091-7
Bertini R, Howard OM, Dong HF, Oppenheim JJ, Bizzarri C, Sergi R, Caselli
G, Pagliei S, Romines B, Wilshire JA, Mengozzi M, Nakamura H, Yodoi J,
Pekkari K, Gurunath R, Holmgren A, Herzenberg LA and Ghezzi P (1999)
Thioredoxin, a redox enzyme released in infection and inflammation, is a
unique chemoattractant for neutrophils, monocytes, and T cells. J Exp Med
189:1783-9.
Mustacich D and Powis G (2000) Thioredoxin reductase. Biochem J 346 Pt 1:18
53
C. Skogastierna
103.
104.
105.
106.
107.
108.
109.
110.
111.
112.
113.
114.
115.
116.
117.
118.
54
Selenius M, Rundlof AK, Olm E, Fernandes AP and Bjornstedt M (2010)
Selenium and the selenoprotein thioredoxin reductase in the prevention,
treatment and diagnostics of cancer. Antioxid Redox Signal 12:867-80
Williams CHJ, ed. Lipoamide dehydrogenase, glutathione reductase,
thioredoxin reductase and mercuric ion reductase - A family of flavoenzyme
transhydrogenase. Chemistry and Biochemistry of Flavoenzyme, ed. Müller F.
Vol. 3, 121-211. 1992, CRC Press: Boca, Raton.
Tamura T and Stadtman TC (1996) A new selenoprotein from human lung
adenocarcinoma cells: purification, properties, and thioredoxin reductase
activity. Proc Natl Acad Sci U S A 93:1006-11
Sandalova T, Zhong L, Lindqvist Y, Holmgren A and Schneider G (2001)
Three-dimensional structure of a mammalian thioredoxin reductase:
implications for mechanism and evolution of a selenocysteine-dependent
enzyme. Proc Natl Acad Sci U S A 98:9533-8
Miranda-Vizuete A, Damdimopoulos AE, Pedrajas JR, Gustafsson JA and
Spyrou G (1999) Human mitochondrial thioredoxin reductase cDNA cloning,
expression and genomic organization. Eur J Biochem 261:405-12
Miranda-Vizuete A, Damdimopoulos AE and Spyrou G (1999) cDNA cloning,
expression and chromosomal localization of the mouse mitochondrial
thioredoxin reductase gene(1). Biochim Biophys Acta 1447:113-8
Soderberg A, Sahaf B and Rosen A (2000) Thioredoxin reductase, a redoxactive selenoprotein, is secreted by normal and neoplastic cells: presence in
human plasma. Cancer Res 60:2281-9
Farber E (1984) Pre-cancerous steps in carcinogenesis. Their physiological
adaptive nature. Biochim Biophys Acta 738:171-80
Farber E and Sarma DS (1987) Hepatocarcinogenesis: a dynamic cellular
perspective. Lab Invest 56:4-22
Kinzler KW and Vogelstein B (1996) Lessons from hereditary colorectal
cancer. Cell 87:159-70
Van Gijssel HE, Ohlson LC, Torndal UB, Mulder GJ, Eriksson LC, PorschHallstrom I and Meerman JH (2000) Loss of nuclear p53 protein in
preneoplastic rat hepatocytes is accompanied by Mdm2 and Bcl-2
overexpression and by defective response to DNA damage in vivo. Hepatology
32:701-10
Zhivotovsky B and Orrenius S (2003) Defects in the apoptotic machinery of
cancer cells: role in drug resistance. Semin Cancer Biol 13:125-34
Rotstein J, Sarma DS and Farber E (1986) Sequential alterations in growth
control and cell dynamics of rat hepatocytes in early precancerous steps in
hepatocarcinogenesis. Cancer Res 46:2377-85
Kawata S, Yamasaki E, Nagase T, Inui Y, Ito N, Matsuda Y, Inada M, Tamura
S, Noda S, Imai Y and Matsuzawa Y (2001) Effect of pravastatin on survival in
patients with advanced hepatocellular carcinoma. A randomized controlled trial.
Br J Cancer 84:886-91
Graf H, Jungst C, Straub G, Dogan S, Hoffmann RT, Jakobs T, Reiser M,
Waggershauser T, Helmberger T, Walter A, Walli A, Seidel D, Goke B and
Jungst D (2008) Chemoembolization combined with pravastatin improves
survival in patients with hepatocellular carcinoma. Digestion 78:34-8
Platz EA, Leitzmann MF, Visvanathan K, Rimm EB, Stampfer MJ, Willett WC
and Giovannucci E (2006) Statin drugs and risk of advanced prostate cancer. J
Natl Cancer Inst 98:1819-25
119.
120.
121.
122.
123.
124.
125.
126.
127.
128.
129.
130.
131.
132.
133.
134.
Khurana V, Sheth A, Caldito G and Barkin JS (2007) Statins reduce the risk of
pancreatic cancer in humans: a case-control study of half a million veterans.
Pancreas 34:260-5
Khurana V, Bejjanki HR, Caldito G and Owens MW (2007) Statins reduce the
risk of lung cancer in humans: a large case-control study of US veterans. Chest
131:1282-8
Poynter JN, Gruber SB, Higgins PD, Almog R, Bonner JD, Rennert HS, Low
M, Greenson JK and Rennert G (2005) Statins and the risk of colorectal cancer.
N Engl J Med 352:2184-92
Stearman RS, Grady MC, Nana-Sinkam P, Varella-Garcia M and Geraci MW
(2007) Genetic and epigenetic regulation of the human prostacyclin synthase
promoter in lung cancer cell lines. Mol Cancer Res 5:295-308
Moncada S, Gryglewski R, Bunting S and Vane JR (1976) An enzyme isolated
from arteries transforms prostaglandin endoperoxides to an unstable substance
that inhibits platelet aggregation. Nature 263:663-5
Ota K, Suehiro T, Arii K, Ikeda Y, Kumon Y, Osaki F and Hashimoto K (2005)
Effect of pitavastatin on transactivation of human serum paraoxonase 1 gene.
Metabolism 54:142-50
Jia X, Wei M, Fu X, Gu X, Fan W, Zhang J and Xue L (2009) Intensive
cholesterol-lowering therapy improves large artery elasticity in acute
myocardial infarction patients. Heart Vessels 24:340-6
Frigola J, Munoz M, Clark SJ, Moreno V, Capella G and Peinado MA (2005)
Hypermethylation of the prostacyclin synthase (PTGIS) promoter is a frequent
event in colorectal cancer and associated with aneuploidy. Oncogene 24:7320-6
Nakahata N (2008) Thromboxane A2: physiology/pathophysiology, cellular
signal transduction and pharmacology. Pharmacol Ther 118:18-35
Katagiri H, Ito Y, Ishii K, Hayashi I, Suematsu M, Yamashina S, Murata T,
Narumiya S, Kakita A and Majima M (2004) Role of thromboxane derived
from COX-1 and -2 in hepatic microcirculatory dysfunction during
endotoxemia in mice. Hepatology 39:139-50
Yokoyama Y, Nimura Y, Nagino M, Bland KI and Chaudry IH (2005) Role of
thromboxane in producing hepatic injury during hepatic stress. Arch Surg
140:801-7
Pidgeon GP, Tamosiuniene R, Chen G, Leonard I, Belton O, Bradford A and
Fitzgerald DJ (2004) Intravascular thrombosis after hypoxia-induced pulmonary
hypertension: regulation by cyclooxygenase-2. Circulation 110:2701-7
Cathcart MC, Tamosiuniene R, Chen G, Neilan TG, Bradford A, O'Byrne KJ,
Fitzgerald DJ and Pidgeon GP (2008) Cyclooxygenase-2-linked attenuation of
hypoxia-induced pulmonary hypertension and intravascular thrombosis. J
Pharmacol Exp Ther 326:51-8
Helliwell RJ, Adams LF and Mitchell MD (2004) Prostaglandin synthases:
recent developments and a novel hypothesis. Prostaglandins Leukot Essent
Fatty Acids 70:101-13
Christman BW, McPherson CD, Newman JH, King GA, Bernard GR, Groves
BM and Loyd JE (1992) An imbalance between the excretion of thromboxane
and prostacyclin metabolites in pulmonary hypertension. N Engl J Med 327:705
Weitz-Schmidt G, Welzenbach K, Brinkmann V, Kamata T, Kallen J, Bruns C,
Cottens S, Takada Y and Hommel U (2001) Statins selectively inhibit leukocyte
function antigen-1 by binding to a novel regulatory integrin site. Nat Med
7:687-92
55
C. Skogastierna
135.
136.
137.
138.
139.
140.
141.
142.
143.
144.
145.
146.
147.
148.
149.
150.
151.
56
Amarenco P (2001) Hypercholesterolemia, lipid-lowering agents, and the risk
for brain infarction. Neurology 57:S35-44
Nakayama T (2010) Genetic polymorphisms of prostacyclin synthase gene and
cardiovascular disease. Int Angiol 29:33-42
Warner TD and Mitchell JA (2002) Cyclooxygenase-3 (COX-3): filling in the
gaps toward a COX continuum? Proc Natl Acad Sci U S A 99:13371-3
Tohgi H, Konno S, Tamura K, Kimura B and Kawano K (1992) Effects of lowto-high doses of aspirin on platelet aggregability and metabolites of
thromboxane A2 and prostacyclin. Stroke 23:1400-3
Sakai H, Suzuki T, Takahashi Y, Ukai M, Tauchi K, Fujii T, Horikawa N,
Minamimura T, Tabuchi Y, Morii M, Tsukada K and Takeguchi N (2006)
Upregulation of thromboxane synthase in human colorectal carcinoma and the
cancer cell proliferation by thromboxane A2. FEBS Lett 580:3368-74
Nie D, Che M, Zacharek A, Qiao Y, Li L, Li X, Lamberti M, Tang K, Cai Y,
Guo Y, Grignon D and Honn KV (2004) Differential expression of
thromboxane synthase in prostate carcinoma: role in tumor cell motility. Am J
Pathol 164:429-39
Kajita S, Ruebel KH, Casey MB, Nakamura N and Lloyd RV (2005) Role of
COX-2, thromboxane A2 synthase, and prostaglandin I2 synthase in papillary
thyroid carcinoma growth. Mod Pathol 18:221-7
Cathcart MC, Reynolds JV, O'Byrne KJ and Pidgeon GP (2010) The role of
prostacyclin synthase and thromboxane synthase signaling in the development
and progression of cancer. Biochim Biophys Acta 1805:153-66
Honn KV, Cicone B and Skoff A (1981) Prostacyclin: a potent antimetastatic
agent. Science 212:1270-2
Keith RL, Miller YE, Hoshikawa Y, Moore MD, Gesell TL, Gao B, Malkinson
AM, Golpon HA, Nemenoff RA and Geraci MW (2002) Manipulation of
pulmonary prostacyclin synthase expression prevents murine lung cancer.
Cancer Res 62:734-40
Keith RL, Miller YE, Hudish TM, Girod CE, Sotto-Santiago S, Franklin WA,
Nemenoff RA, March TH, Nana-Sinkam SP and Geraci MW (2004) Pulmonary
prostacyclin synthase overexpression chemoprevents tobacco smoke lung
carcinogenesis in mice. Cancer Res 64:5897-904
Moncada S (1992) The 1991 Ulf von Euler Lecture. The L-arginine: nitric
oxide pathway. Acta Physiol Scand 145:201-27
Nathan C (1992) Nitric oxide as a secretory product of mammalian cells.
FASEB J 6:3051-64
MSD, Zocord, 2011.
Parini P, Gustafsson U, Davis MA, Larsson L, Einarsson C, Wilson M, Rudling
M, Tomoda H, Omura S, Sahlin S, Angelin B, Rudel LL and Eriksson M
(2008) Cholesterol synthesis inhibition elicits an integrated molecular response
in human livers including decreased ACAT2. Arterioscler Thromb Vasc Biol
28:1200-6
Ward JM, Rehm S and Reynolds CW (1990) Pathology of tumours in
laboratory animals. Tumours of the rat. Tumours of the haematopoietic system.
IARC Sci Publ 625-57
Solt DB, Medline A and Farber E (1977) Rapid emergence of carcinogeninduced hyperplastic lesions in a new model for the sequential analysis of liver
carcinogenesis. Am J Pathol 88:595-618
152.
153.
154.
155.
156.
157.
158.
159.
160.
161.
162.
163.
164.
165.
166.
167.
168.
169.
Inman SR, Stowe NT, Cressman MD, Brouhard BH, Nally JV, Jr., Satoh S,
Satodate R and Vidt DG (1999) Lovastatin preserves renal function in
experimental diabetes. Am J Med Sci 317:215-21
Tatsuta M, Iishi H, Baba M, Iseki K, Yano H, Uehara H, Yamamoto R and
Nakaizumi A (1998) Suppression by pravastatin, an inhibitor of p21ras
isoprenylation, of hepatocarcinogenesis induced by N-nitrosomorpholine in
Sprague-Dawley rats. Br J Cancer 77:581-7
Livak KJ, Flood SJ, Marmaro J, Giusti W and Deetz K (1995) Oligonucleotides
with fluorescent dyes at opposite ends provide a quenched probe system useful
for detecting PCR product and nucleic acid hybridization. PCR Methods Appl
4:357-62
Livak KJ and Schmittgen TD (2001) Analysis of relative gene expression data
using real-time quantitative PCR and the 2(-Delta Delta C(T)) Method.
Methods 25:402-8
Engvall E and Perlmann P (1971) Enzyme-linked immunosorbent assay
(ELISA). Quantitative assay of immunoglobulin G. Immunochemistry 8:871-4
Van Weemen BK and Schuurs AH (1971) Immunoassay using antigen-enzyme
conjugates. FEBS Lett 15:232-236
Porstmann T and Kiessig ST (1992) Enzyme immunoassay techniques. An
overview. J Immunol Methods 150:5-21
Samuelsson B, Goldyne M, Granstrom E, Hamberg M, Hammarstrom S and
Malmsten C (1978) Prostaglandins and thromboxanes. Annu Rev Biochem
47:997-1029
Dusting GJ, Lattimer N, Moncada S and Vane JR (1977) Prostaglandin X, the
vascular metabolite of arachidonic acid responsible for relaxation of bovine
coronary artery strips [proceedings]. Br J Pharmacol 59:443P
Rosenkranz B, Fischer C, Reimann I, Weimer KE, Beck G and JC FR (1980)
Identification of the major metabolite of prostacyclin and 6-ketoprostaglandin
F1 alpha in man. Biochim Biophys Acta 619:207-13
Catella F, Nowak J and Fitzgerald GA (1986) Measurement of renal and nonrenal eicosanoid synthesis. Am J Med 81:23-9
Frolich JC (1984) Measurement of icosanoids. Report of the Group for
Standardization of Methods in Icosanoid Research. Prostaglandins 27:349-68
Lawson JA, Patrono C, Ciabattoni G and Fitzgerald GA (1986) Long-lived
enzymatic metabolites of thromboxane B2 in the human circulation. Anal
Biochem 155:198-205
Ciabattoni G, Pugliese F, Davi G, Pierucci A, Simonetti BM and Patrono C
(1989) Fractional conversion of thromboxane B2 to urinary 11dehydrothromboxane B2 in man. Biochim Biophys Acta 992:66-70
Misko TP, Schilling RJ, Salvemini D, Moore WM and Currie MG (1993) A
fluorometric assay for the measurement of nitrite in biological samples. Anal
Biochem 214:11-6
Arpino P (1992) Combined liquid chromatography mass spectrometry. Part III.
Applications of thermospray. Mass Spectrometry Reviews 11:3-40
Bjorkhem-Bergman L, Lindh JD and Bergman P (2011) What is a relevant
statin concentration in cell experiments claiming pleiotropic effects? Br J Clin
Pharmacol 72:164-5
Tang XL, Jiang ZY, Dong J, Liu XC, Cai SY, Xiao R and Lu YR (2006)
[Expression of tissue factor induced by IL-6 in HUVEC]. Sichuan Da Xue Xue
Bao Yi Xue Ban 37:234-7
57
C. Skogastierna
170.
171.
172.
173.
174.
175.
176.
177.
58
Majed BH and Khalil RA (2012) Molecular Mechanisms Regulating the
Vascular Prostacyclin Pathways and Their Adaptation during Pregnancy and in
the Newborn. Pharmacol Rev 64:540-82
Wright DH, Abran D, Bhattacharya M, Hou X, Bernier SG, Bouayad A, Fouron
JC, Vazquez-Tello A, Beauchamp MH, Clyman RI, Peri K, Varma DR and
Chemtob S (2001) Prostanoid receptors: ontogeny and implications in vascular
physiology. Am J Physiol Regul Integr Comp Physiol 281:R1343-60
Liao JK (2002) Beyond lipid lowering: the role of statins in vascular protection.
Int J Cardiol 86:5-18
Kugi M, Matsunaga A, Ono J, Arakawa K and Sasaki J (2002) Antioxidative
effects of fluvastatin on superoxide anion activated by angiotensin II in human
aortic smooth muscle cells. Cardiovasc Drugs Ther 16:203-7
Miwa S, Watada H, Omura C, Takayanagi N, Nishiyama K, Tanaka Y, Onuma
T and Kawamori R (2005) Anti-oxidative effect of fluvastatin in hyperlipidemic
type 2 diabetic patients. Endocr J 52:259-64
Vandjelovic N, Zhu H, Misra HP, Zimmerman RP, Jia Z and Li Y (2012) EPR
studies on hydroxyl radical-scavenging activities of pravastatin and fluvastatin.
Mol Cell Biochem 364:71-7
Imaeda A, Tanigawa T, Aoki T, Kondo Y, Nakamura N and Yoshikawa T
(2001) Antioxidative effects of fluvastatin and its metabolites against oxidative
DNA damage in mammalian cultured cells. Free Radic Res 35:789-801
Nakamura T, Nishi H, Kokusenya Y, Hirota K and Miura Y (2000) Mechanism
of antioxidative activity of fluvastatin-determination of the active position.
Chem Pharm Bull (Tokyo) 48:235-7