Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Dental emergency wikipedia , lookup
Public health genomics wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Transmission (medicine) wikipedia , lookup
Canine parvovirus wikipedia , lookup
Compartmental models in epidemiology wikipedia , lookup
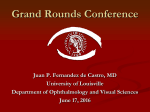
Case Reports Severe Oculofacial Sequelae of Cutaneous Blastomyces dermatitidis Joseph S. Schmutz, M.D.*, Nicholas A. Ramey, M.D.*, Gregory M. Gauthier, M.D.†, and Mark J. Lucarelli, M.D., F.A.C.S.* Abstract: This study reports a case of Blastomyces dermatitidis soft tissue infection resulting in a disfiguring lower eyelid ectropion from cicatricial and postinflammatory cutaneous changes. Primary treatment included intravenous amphotericin B followed by long-term oral itraconazole, which resulted in complete remission of the disease without debridement, after which cicatricial ectropion was repaired surgically with scar release, full-thickness skin graft, and temporary Frost tarsorraphy. Cutaneous blastomycosis may cause severe oculofacial sequelae, ranging from eyelid ectropion to widespread facial cicatrix, and may mimic other more common infectious processes, in addition to malignancy. Recommended antifungal therapy includes induction with intravenous amphotericin B and a long course of oral antifungals, preferably coordinated in conjunction with an infectious disease specialist. Ectropion repair should be delayed until the inflammatory response has completely healed. If the ocular surface is compromised or nearby ocular structures are threatened, primary debridement and repair may be indicated. B lastomyces dermatitidis, the etiologic agent of blastomycosis, causes pyogranulomatous inflammation. Infection is primarily acquired by inhalation of aerosolized spores following disruption of soil to cause pneumonia, which can be followed by lymphohematogenous dissemination to the skin. This pathogen can also cause primary cutaneous disease by a penetrating injury to the skin. This report illustrates a patient with severe facial and periocular blastomycosis complicated by cicatricial lower eyelid ectropion. Primary treatment and secondary repair are discussed. The medical literature is reviewed for recent clinical and microbiologic updates on blastomycosis. Informed written consent was obtained for the use of clinical photographs from the patient, and this study is Health Insurance Portability and Accountability Act (HIPAA) compliant. CASE REPORT A 45-year-old man in August of 2010 was evaluated for bilateral facial lesions (Figure), OS irritation, malaise, and weight loss. He developed periauricular and cervical lymphadenopathy, and purulent nodules involving his face, trunk, and upper and lower extremities 14 months prior to presentation. Over a period of several weeks after initial presentation, several cutaneous lesions spontaneously resolved, but those on his face and buttocks persisted. In 2009, he sought medical attention at an urgent care *Department of Ophthalmology, Oculoplastic, Facial Cosmetic and Orbital Surgery Service; and †Department of Medicine, University of Wisconsin, Madison, Wisconsin, U.S.A. Accepted for publication June 1, 2014. Supported, in part, by an unrestricted grant from Research to Prevent Blindness Inc., New York, NY, to the Department of Ophthalmology and Visual Sciences. This work has not been previously presented. The authors have no financial or conflicts of interest to disclose. Address correspondence and reprint requests to Joseph Schmutz, M.D., University of Wisconsin, Madison, WI 53705. E-mail: [email protected] DOI: 10.1097/IOP.0000000000000245 Ophthal Plast Reconstr Surg, Vol. XX, No. XX, 2014 facility for the facial lesions. He was prescribed clindamycin for 10 days but was unable to complete the antibiotic course due to the development of a drug rash. From December 2009 to August 2010, the patient experienced progression of his facial and buttock lesions. He was diagnosed with cutaneous Blastomycosis based on skin biopsy demonstrating broad-based budding yeast and a positive urine Blastomyces antigen. Culture of the skin lesions grew B. dermatitidis. Following induction therapy with liposomal amphotericin B, which was stopped at 9 days due to development of a morbilliform rash from the amphotericin, he was treated with oral itraconazole solution for 9 months. Itraconazole levels were monitored monthly and were therapeutic (>1 μg/ml) throughout the treatment course. Therapy was discontinued due to side effects of headache, nausea, and fatigue. Surgical debridement of infected tissue was not required to clear the active infection, as appropriate medical treatment yielded dramatic results. (Figure). The verrucous lesions ultimately improved after several months of the above regimen, leaving large cheek and left lower eyelid cicatricial plaques in its wake. The resulting left lower eyelid cicatricial ectropion was repaired in a single-stage procedure 9 months after finishing antifungal therapy. The scar was released. A 35 mm × 17 mm full-thickness skin graft was taken from the right retroauricular area to exactly match and fill the defect, and then a lateral tarsal strip procedure was performed, followed by temporary Frost tarsorraphy. DISCUSSION Blastomyces dermatitidis grows in the moist soil of wooded areas rich in organic debris of the Mississippi and Ohio River basins, United States, and Canadian regions bordering the Great Lakes and the St. Lawrence River Valley. It is hyperendemic in north-central Wisconsin with an incidence up to 40 per 100,000 in certain counties.1 The fungus is thermally dimorphic, existing as a filamentous mold in the soil (22–25°C) and as a pathogenic yeast in the tissue (37°C). Following disruption of soil, aerosolized mycelial fragments and infectious spores are inhaled into the lungs and converted into broad-based budding yeast. Once established in the lung, yeast can spread to extrapulmonary sites, most often to the skin, bone, and genitourinary system.2,3 Integumentary manifestations occur in up to 80% of patients with disseminated infection, with predilection for the face and exposed areas.4 Eyelid involvement with systemic blastomycosis infection is rare, occurring in less than 2% of cases.5 Cutaneous blastomycosis may cause severe oculofacial sequelae, ranging from eyelid ectropion to widespread facial cicatrix. Rarely, intraocular involvement and optic nerve infection have also been reported.6 Although integumentary manifestations are common after hematogenous dissemination, direct inoculation of the skin is also possible after a penetrating injury.7 Cutaneous and systemic manifestations of blastomycosis may mimic other more common infectious processes and malignancy.2,4 Understanding the risk factors associated with acquisition of B. dermatitidis is important for prompt diagnosis. Practice guidelines published by the Infectious Diseases Society of America recommend that patients with severe infection be treated with intravenous amphotericin B followed by a prolonged course of oral antifungals such as itraconazole.8 Coordination with an expert in infectious diseases is recommended. Whenever possible, surgical correction of oculofacial sequelae should be delayed until clearance of infection. Delay may not be feasible when nearby ocular structures are threatened or when refractory lagophthalmos or severe retraction threaten to compromise protection of the ocular surface. In e1 Copyright © 2014 The American Society of Ophthalmic Plastic and Reconstructive Surgery, Inc. Unauthorized reproduction of this article is prohibited. Ophthal Plast Reconstr Surg, Vol. XX, No. XX, 2014 Case Reports External photographs documenting severe active Blastomyces dermatitidis facial cellulitis (top left and center). Postinfectious cicatricial left lower eyelid ectropion remained after 9 months of systemic antifungal treatment (top right). Postoperative photographs demonstrate successful repair after scar release, full thickness skin graft, and temporary Frost tarsorraphy (below). these cases, earlier surgical intervention should be considered. In this case, the patient required 9 months of therapy for the infection to completely clear, after which successful cicatricial ectropion repair was accomplished. In summary, B. dermatitidis infection can have severe oculofacial sequelae. If possible, reconstruction should be delayed until active infection is cured and cicatrix is no longer progressing. REFERENCES 1.Baumgardner DJ, Buggy BP, Mattson BJ, et al. Epidemiology of blastomycosis in a region of high endemicity in north central Wisconsin. Clin Infect Dis 1992;15:629–35. 2. Saccente M, Woods GL. Clinical and laboratory update on blastomycosis. Clin Microbiol Rev 2010;23:367–81. e2 3.Smith JA, Kauffman CA. Blastomycosis. Proc Am Thorac Soc 2010;7:173–80. 4. Woofter MJ, Cripps DJ, Warner TF. Verrucous plaques on the face. North American blastomycosis. Arch Dermatol 2000;136:547–50. 5.Bartley GB. Blastomycosis of the eyelid. Ophthalmology 1995;102:2020–3. 6. Pariseau B, Lucarelli MJ, Appen RE. Unilateral Blastomyces dermatitidis optic neuropathy case report and systematic literature review. Ophthalmology 2007;114:2090–4. 7.Shukla S, Singh S, Jain M, et al. Paediatric cutaneous blastomycosis: a rare case diagnosed on FNAC. Diagn Cytopathol 2009;37:119–21. 8. Chapman SW, Dismukes WE, Proia LA, et al.; Infectious Diseases Society of America. Clinical practice guidelines for the management of blastomycosis: 2008 update by the Infectious Diseases Society of America. Clin Infect Dis 2008;46:1801–12. © 2014 The American Society of Ophthalmic Plastic and Reconstructive Surgery, Inc. Copyright © 2014 The American Society of Ophthalmic Plastic and Reconstructive Surgery, Inc. Unauthorized reproduction of this article is prohibited.