Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
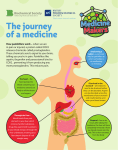
BHS 116.2: Physiology II Notetaker: Stephanie Cullen Date: 2/6/13 Page: 1 Review Hour 2: MORE PICTURES WILL BE ON THE PRINTED VERSION Liver - - - Functions o Metabolizing fats Chylomicrons enter systemic circulation right from the GI tract via the lymph system Primary source of lipids after a meal Eventually go to the liver and are processed In b/t meals, tissues need fat so use lipoproteins VLDL: rich in triglycerides LDL: primary lipid particle b/t meals o Rich in cholesterol o “Bad” lipoparticle o VLDL is taken up by its target tissues quickly so they can use the triglycerides so left w/ LDL particles (cholesterol) HDL: rich in proteins o Bile production Bile salts are made from cholesterol Released and stored in the gallbladder Concentrated in the gallbladder (vs in the liver) Acts even better as an emulsifier Blood from 2 sources o ¼: systemic blood from the hepatic a. Supplies hepatocytes and other liver cells with oxygen o ¾: portal system Blood from the spleen and intestines All absorbed nutrients (except fat) have to go through the liver first Anatomy o Portal triad Hepatic portal v., hepatic a., and common bile duct Stay together throughout the liver All split into smaller vessels together o Portal v. and hepatic a. fuse and dump contents into sinusoids (modified capillary lined w/ endothelial cells) Travel the length of the liver in all different directions Drain into central v. Central veins drain into hepatic v. Vena cava o Hepatocytes: main liver cells Carry out all functions of the liver except phagoyctosis of bacteria (Kupffer cells) Endothelial cells line sinusoids (large pores) Fluid drains through pores and get into space b/t hepatocytes and endothelial cells (space of Disse) Where all the nutrients from the GI tract come into direct contact w/ hepatocytes to be taken up Not empty o Stellate cell- quiescent (stores fat) o Collagen network for structure o Kupffer cell: the protector cell BHS 116.2: Physiology II Notetaker: Stephanie Cullen o o Date: 2/6/13 Page: 2 Phagocytosis of bacteria or large aggregates Lobules: functional units of the liver Sinusoids lined w/ hepatocytes Allows liver to process and detoxify blood very efficiently Esophagus - Esophagitis: inflammation of esophagus o Due to gastroesophageal reflux disease o Irritates lower portion of esophagus o Causes inflammatory response o Heart burn and difficulty swallowing o If it persists, the epithelium of the esophagus will undergo metaplasia and convert from stratified squamous to columnar (more protective against acid being refluxed) - Esophageal varices o End result of cirrhosis leading to portal hypertension o Esophageal v. as part of portal system Normally small w/ no role Portal hypertension: back up of blood going into liver, dilate into the esophagus, can rupture and lead to significant bleeding o Can be fatal Stomach - Hiatal hernia o Sliding Upward shift of the stomach through the diaphragm o Paraesophageal Esophagus is not pulled up but the fundus of the stomach squeezes through alongside the esophagus Dangerous over time because blood vessels supplying the greater curvature of the stomach are pinched off in the area of the esophageal sphincter Ischemia of this part of the stomach - Gastritis o Inflammation of the stomach o Usually chronic (build up inflammation overtime) Atrophy of gastric mucosa Long time: metaplasia to more columnar type of epithelia to be more protective against acid and pepsin in stomach Main cause: helicobacter pylori infection especially in antral region of stomach Other causes: autoimmune, toxicity, mechanical, etc. Age increases incidence of H. pylori infection Mostly asymptomatic (silent) Eventually the mucosa atrophies Decrease mucus production since there are no longer functional cells Decrease acid production o If H. pylori infection: hyperchlorhydia o If autoimmune: destroys parietal cells so no HCl is produced (achlorhydria) No intrinsic factor produced either (pernicious anemia and achlorhydria) BHS 116.2: Physiology II Notetaker: Stephanie Cullen Date: 2/6/13 Page: 3 - - w/o proper acid secretion: decreased pepsin activation so decreased protein breakdown, increased bacterial infection possibility o Can have acute bouts Can be severe but short length (there then disappears all the sudden) Can get some bleeding but usually a minor inflammatory reaction then it’s gone Pain in the stomach region, nausea, vomiting Main causes: increased acid secretion, decreased HCO3- secretion (protective) Epithelium is more subject to being weakened or destroyed Decreased blood flow (ischemia) Disruption of protective mucus layer Peptic ulcers o Can occur in any portion of the GI tract but are typically localized to the stomach and duodenum 80% of peptic ulcers are found in the duodenum When the chyme is at its most acidic point, it touches duodenum unless NaHCO3 is already being released from the pancreas giving it protective mucus o Result of imbalance of protective mechanism (mucus and HCO3-) and damaging forces Maybe more acid is being produced than normal Impaired defenses and increase in aggregating factors o 2 requirements for it to be a peptic ulcer: Pepsin and HCl (gastric acid) must be present since these are what it actually breaking down the lining of the stomach mucosa o H. pylori major role causing nearly all duodenal ulcers and 70% of gastric ulcers o Chronic gastritis can lead to peptic ulceration because of the presence of H. pylori Peptic ulcer vs chronic gastritis o Chronic gastritis: limited to the mucosal layer Atrophy of mucosa Influx of lymphocytes and other immune cells Metaplasia of stomach epithelium o Peptic ulcer Degradation all the way through into the submucosa Inflammation and fibrosis in submucosa If untreated: digests all the way through and ruptures the lining of the SI (sepsis) Small Intestine - Infectious enterocolitis o Viral Gets into epithelium and destroys intestinal epithelium Prevents absorption of fluids or nutrients Causes diarrhea o Bacterial Caused by: Toxogenic bacteria o Releases enterotoxin to stimulate the cell to be hypersecretory or breakdown the cell to prevent absorption Enteroinvasive bacterial (acts like a virus) o Enters the cell and destroys epithelium Enterotoxin (B. toxin) taken in w/o the bacteria present - Chron’s disease o Idiopathic inflammatory bowel disease BHS 116.2: Physiology II Notetaker: Stephanie Cullen Date: 2/6/13 Page: 4 o o - - Autoimmune Granulomas form Anywhere in GI tract but typically the small and large intestine are the main targets o Iritis and uveitis Ulcerative colitis o Restricted to colon (large intestine) o No granulomas o Autoimmune o Uveitis Chron’s vs ulcerative colitis o Chron’s: skip lesions Sections of diseased tissue followed by section of normal tissue, etc. Inflammation affects all 3 walls of the lining- transmural inflammation Only in small intestine or large intestine o Ulcerative Colitis Only affects mucosa and submucosa Pseudopolyps: islands of normal tissue throughout the colon Continuous disease: affects entire section of intestine Don’t have the skip lesions Liver Pathologies - Hepatic responses o Inflammation: hepatitis Continued inflammation results in degeneration Damaged hepatocytes Hepatocytes don’t function fully and look weird under microscope Necrosis- hepatocytes die o Regenerates If the toxin is removed after necrosis occurs, can get hepatocyte regeneration to normal If insult is continually present after necrosis begins to occur, get fibrosis Strands of bridging fibrosis from blood vessel to blood vessel throughout the liver IRREVERSIBLE: can’t get regeneration once fibrosis occurs o Cirrhosis Fibrotic corrals Fibrosis around necrosis areas BHS 116.2: Physiology II Notetaker: Stephanie Cullen Date: 2/6/13 Page: 5 - - - - - Regeneration of necrotic cells but they are surrounded by fibrotic bands Disrupts normal architecture of the liver (no lobules) so it doesn’t function normally 3 characteristics: bridging fibrous septa, nodules (micronodules or macronodules) Lab tests and Clinical Consequences, and disruption of the architecture o Is the disease affecting hepatocyte integrity? Affecting biliary excretion? Affecting hepatocyte function? Jaundice o Accumulation of conjugated or unconjugated bilirubin in skin or eye Gives a yellowish tint o Heme is converted into bilirubin when RBCs die o Bilirubin is carried to liver and conjugated (post-hepatic) Conjugated : hepatitis and obstruction of bile flow are the major causes o Unconjuagted : hemolytic anemia is the major cause Before bilirubin gets to the liver (pre-hepatic) Cholestasis o Accumulation of bilirubin and bile salts and cholesterol in the skin o Post-hepatic since it has to do with bile formation and release o Itchy skin, cholesterol build up, presence of serum alkaline phosphatase (should be in the bile duct epithelium so when it is in the blood it means there is rupture and necrosis) Pathogenesis of Cirrhosis o Hepatocytes undergo necrosis (must have hepatocyte death either by toxin, bacteria, etc) o Regeneration of hepatocytes o Progressive fibrosis encircling regions of regeneration o Trigger Lots of collagen (types I and III) is present during cirrhosis Makes up fibrotic bands and fills up space of Disse No filtration through the sinusoids Liver blood pressure builds up Portal hypertension Stellate cells are activated and hypersecrete the excess collagen o Causes of portal HTN Due to increased resistance to blood flow Pre-hepatic: Blood clot in portal vessel before the liver Post-hepatic: Right-sided heart failure leads to back up through whole system Post-hepatic: Obstruction in hepatic v. leaving liver Cirrhosis is the main cause because of the high pressure sinusoids 4 clinical consequences of portal hypertension: BHS 116.2: Physiology II Notetaker: Stephanie Cullen Date: 2/6/13 Page: 6 o o - Ascites: edema build up in abdominal cavity Formation of porto-systemic venous shunts (esophageal varices) Back up in the veins o Splenomegaly: no drainage of the spleen causing swelling o Hepatic encephalopathy: excess ammonia is the byproduct from breaking down amino groups Converted to urea by liver Ammonia left in blood (causing swelling of the brain) when the liver isn’t functioning properly Viral hepatitis o o o o o Inflammation of liver due to viral infection A and E never result in cirrhosis or issues w/ liver B: only DNA virus; rest are RNA Fairly common but rarely results in cirrhosis or death Mostly subclinical or acute C: dangerous Major cause of liver disease 85% get to chronic hepatitis Then 20% lead to cirrhosis Actue vs chronic infection Know antigens or antibodies present or not present for hep B and hep C o D: requires co-infection w/ hep B Uninfected person infected w/ both at the same time: 90% chance of recovery w/o issues Hep B carrier who is then infected w/ hep D: major chance (80%) for cirrhosis to occur (liver disease) o Clinical syndromes of viral hepatitis Carrier state: asymptomatic BHS 116.2: Physiology II Notetaker: Stephanie Cullen - Date: 2/6/13 Page: 7 Asymptomatic infection: have the disease but don’t show symptoms but can have do have elevated liver enzymes (some cells are breaking down) Acute viral hep: goes through various stages talked about previously Chronic viral hep: continuing or relapsing hepatic disease for more than 6 months Bridging fibrosis and necrosis of hepatocytes Not seen in acute viral hep Alcoholic liver disease o 3 forms: Steatosis: fatty liver Alcoholic hepatitis: could skip steatosis phase Either of these is reversible if quit drinking Cirrhosis (10%): have to go through fatty liver or hepatitis stage first Breaks down the liver and affects its function