Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Major depressive disorder wikipedia , lookup
Emil Kraepelin wikipedia , lookup
History of psychiatric institutions wikipedia , lookup
Antipsychotic wikipedia , lookup
Glossary of psychiatry wikipedia , lookup
Depersonalization disorder wikipedia , lookup
Sluggish schizophrenia wikipedia , lookup
Bipolar II disorder wikipedia , lookup
Asperger syndrome wikipedia , lookup
Parkinson's disease wikipedia , lookup
Separation anxiety disorder wikipedia , lookup
Anti-psychiatry wikipedia , lookup
Cases of political abuse of psychiatry in the Soviet Union wikipedia , lookup
Political abuse of psychiatry in Russia wikipedia , lookup
Generalized anxiety disorder wikipedia , lookup
Rumination syndrome wikipedia , lookup
Abnormal psychology wikipedia , lookup
Alcohol withdrawal syndrome wikipedia , lookup
History of mental disorders wikipedia , lookup
Spectrum disorder wikipedia , lookup
Political abuse of psychiatry wikipedia , lookup
Critical Psychiatry Network wikipedia , lookup
Diagnostic and Statistical Manual of Mental Disorders wikipedia , lookup
Child psychopathology wikipedia , lookup
Factitious disorder imposed on another wikipedia , lookup
Death of Dan Markingson wikipedia , lookup
Classification of mental disorders wikipedia , lookup
History of psychiatry wikipedia , lookup
Emergency psychiatry wikipedia , lookup
Dissociative identity disorder wikipedia , lookup
Conversion disorder wikipedia , lookup
Depression in childhood and adolescence wikipedia , lookup
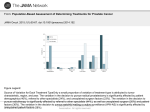
135 J. Indian Assoc. Child Adolesc. Ment. Health 2017; 13(2):135-148 Original Article Children with unexplained physical symptoms referred to psychiatry: A descriptive study Bheemsain Tekkalaki, Sameeran S. Chate, Veerappa Y. Patil, Nanasaheb M. Patil , Jitendra Mugali Address for correspondence: Bheemsain Tekkalaki, MD, Assistant Professor, Department of Psychiatry, K.L.E University’s J.N Medical College, Belagavi, and Karnataka, India. [email protected] Abstract: Background: Unexplained physical symptoms are reported to be common in pediatric population, and are associated with excessive medical resource use, poor quality of life and long term psychiatric complications. Researches focusing on such children are sparse. Aims: This study was done with the aim to assess the sociodemographic and clinical characteristics of children who were referred to psychiatry department for assessment of unexplained physical symptoms. Methods: A retrospective chart analysis of all children and adolescents below 19 years of age, referred to psychiatry for evaluation of unexplained physical symptoms, from January 2010 to December 2015 was done. Data collected and statistical analysis done. Results: Sixty children and adolescents were included in the study. Mean age of the sample was 12.44(±3.21) years, with slight male predominance (58.33%).Most common complaints were headache (26.66%), followed by loss of consciousness (18.33%) and other body aches (15%). Mean number of symptoms per subject was 1.5. Most common psychiatric diagnoses were somatoform 136 and dissociative disorders (48.33%), followed by depressive disorder (11.67%). Pharmacotherapy was started in significantly more number of girls compared to boys (84% v/s48.57%). Conclusion: Majority of subjects referred for evaluation of unexplained somatic symptoms were adolescent males. Abnormal body movements, head ache, and other body aches were the commonest presenting complaints. Somatoform and dissociative disorders, depressive disorders were the commonest psychiatric diagnoses. Key words: Unexplained physical symptoms, Pediatric somatoform disorder, Pediatric liaison psychiatry, General hospital psychiatry. Introduction Unexplained physical symptoms also known as functional somatic symptoms are common in pediatric population [1].Children with functional somatic symptoms often are first seen by general practitioner or a pediatrician. They are referred to mental health professionals late in the course of illness, often leading to excessive, unnecessary investigations and overuse of medical services [2]. According to one estimation, about 20% of pediatric visits to primary care are because of unexplained somatic symptoms and about 47% of the patients referred to pediatric specialist have functional somatic symptoms [3]. According to the literature available, children with functional somatic symptoms often utilize more medical resources, report more school absenteeism, poor functioning and quality of life [4]. Psychiatric comorbidies are very common in these children [5]. Data also suggests that children with functional somatic symptoms continue to have psychiatric morbidities even in adolescence [6]. 137 Data on unexplained physical symptoms in children is sparse and also there are very few studies from India. We took up this study with the aim to assess the sociodemographic and clinical characteristics of children and adolescents who were referred to psychiatry department for assessment of unexplained physical symptoms. Materials and methods Study was carried out in a tertiary care super-specialty teaching hospital of a south Indian city. We conducted a retrospective review. Case files of all children and adolescents (mentioned simply as “children” hereafter unless specified) referred to Psychiatry OPD for assessment of unexplained physical symptoms, for a period of five years from 1st January 2010 to 31st December 2015 were analyzed. Socio-demographic and clinical details were collected using a semi structured proforma. Data was tabulated and appropriate statistical tests were applied using Epi Info-7 software. Results A total of 232 children and adolescents were referred during this period. Out of them, sixty children were referred for the evaluation of unexplained physical symptoms, which formed the sample of our study. Mean age of the sample was 12.44(±3.21) years, with male sex being slightly predominant (58.33%). About half of the subjects (53.33%) were referred from the department of neurosciences, comprising of neuro-medicine, neurosurgery and pediatric neurology. Next most common source of referrals were department of pediatrics (28.33%). (Table no.1). 138 139 Majority (83%) of these subjects had not received any medical/surgical diagnosis. Four (6.67%), children had comorbid seizure disorder and other 6 (10%) had various other comorbidities. On an average, each subject had 1.5 unexplained medical symptoms. Most common complaints were headache (26.66%), followed by loss of consciousness (18.33%) and other body aches (15%) (Table no.1). Most common psychiatric diagnoses were somatoform and dissociative disorders (48.33%), followed by depressive disorder (11.67%), tic disorder (11.67%) and anxiety disorders (8.33%). Almost equal number of subjects received pharmacotherapy (51.67%) and non-pharmacotherapy (49.33%) (Table no.1). We further made comparisons between boys and girls (Table no.2) and between children and adolescents (Table no.3). The only statistically significant difference observed was that, significantly large number of girls (84%) were started on pharmacotherapy compared to boys (48.57%). 140 Discussion In this study, out of 232 children referred to psychiatry, 60 were for evaluation of unexplained physical symptoms, which is about 25.82% of all referred children. Similar figures (20.5%) were reported by Mullick (2002) in his clinical study [7], suggesting high 141 142 prevalence of functional somatic symptoms in clinical population. Mean age of our sample was 12.44 (±3.41) years. A Similar findings were reported by available studies from Indian subcontinent and elsewhere [7-9]. Adolescents being more communicative than children may be a reason for this age distribution. Slight male predominance (58.33%) was observed in our study, a finding similar to the data from Indian subcontinent [7, 10], but different from western data (only 29% were males in a study by Coffelt et al) [9], including the large epidemiological Copenhagen study [11], Socio-cultural differences in help seeking may be the reason for this discrepancy. About half (58.33%) of these children were referred from the Neuroscience departments (Neurology, Neurosurgery and Pediatric Neurology). This may be because, many psychiatric problems such as pseudo seizures, dissociative motor disorders, and sensory disorders resemble neurological disorders. Literature states that about 15% of the patients seen by neurologist have no physical base for their symptoms and in another 15%, the symptoms are out of proportion to the cause [12, 13]. The next major other source of referral was the department of pediatrics (28.33%), which is understandable considering the pediatric sample of this study. These findings also reflect the pathway of care for such symptoms. Given the obvious physical nature of these symptoms, stigma associated with psychiatric consultations and lack awareness about psychiatric illness in general may be the reasons why these children usually visit a pediatrician first. This further indicates the need for sensitization of non-psychiatric physicians about the prompt identification and timely referral of such children. 143 Mean number of symptoms in our study (1.5) was much smaller compared to the other prospective studies on unexplained physical symptoms in children. Mullick has reported a mean of 14.21 symptoms [7], and Konijenberg et al have reported a mean of 8.4 symptoms in boys and 10.7 symptoms in girls [14]. The striking differences in the findings are due to the retrospective nature of our study and the clinicians might have not made extensive efforts to explore all somatic symptoms. Another reason may be that, no structured tool were used to assess functional somatic symptoms (Konijenberg et al. [14] have used Children Somatic Inventory). These findings imply that a number of somatic symptoms may go undetected if an extensive work up is not done looking for all possible somatic symptoms. About 11.67% and 8.33% of these children were diagnosed with depressive and anxiety disorders respectively. Depressive and anxiety symptoms are known to commonly cooccur functional somatic symptoms (FSS) and in fact FSS are a common reason for depressed adolescent to seek treatment [5]. In a study, 86% of depressed youth reported at least one FSS [15]. Some researchers have reported that the likelihood of comorbid anxiety and depression increases with the number of FSS and also pediatric anxiety and depressive symptoms are associated with heightened likelihood of multiple FSS in later life. They have also questioned the existing nosology that classifies anxiety and depressive syndromes as different from somatic syndromes and, have argued that there is a strong reciprocal association between them. These findings imply that, the clinicians should actively look for unrecognized anxiety and depression in children with FSS in general medical setting [5]. 144 Almost equal number of subjects received pharmacological (51.67%) and nonpharmacological (49.33%) therapy. Benzodiazepines (28.33%) and Selective serotonin reuptake inhibitors (21.7%) were the commonest groups of drugs used. Although there are no strong evidences suggesting use of psychotropic medications in functional pain symptoms, clinicians often use antidepressants based on the experience from adult patients [16]. High proportion of dissociative symptoms in this sample may be the reason for benzodiazepine prescription and presence of depressive and anxiety symptoms may be the reason for frequent prescription of SSRIs. Relatively high reliance on pharmacotherapy may also be because of the fact that, the Indian patients (parents in this case) expect therapist to follow a medical model and less receptive for nonpharmacological intervention [17]. We further divided the sample and made comparisons like boys v/s girls (table no.3) and children v/s adolescents (table no.4). These comparisons did not reveal any statistically significant differences in terms of demographic variables and clinical presentation, and diagnoses, except that more number of girls received pharmacotherapy than the boys. This may be because symptoms in girls may be more severe than boys. Existing literature also suggests that girls present with more number of symptoms than boys [18]. The study findings should be interpreted with the following limitations in the mind, that this is a retrospective study with no standard screening or diagnostic tool used to assess the functional somatic symptoms. Relatively small sample size also is a limitation of this study. Nevertheless, this is one of the earliest efforts to study the children referred to psychiatry for unexplained physical symptoms in Indian context. 145 Conclusions Evaluation of unexplained physical symptoms was the reason for psychiatric referral in about a quarter of children referred to psychiatry. Adolescent males formed the majority of the sample. Neurosciences departments and department of pediatrics were the commonest sources of referral. Abnormal body movements, head ache, and other body aches were the commonest presenting complaints. Majority of these children had not received any medical/surgical diagnoses. Somatoform and dissociative disorders, depressive disorders and anxiety disorders were the commonest psychiatric diagnoses. References 1. Dingle AD. Disorders with physical symptoms. In: Sexson SB editor. Child and Adolescent Psychiatry. 2 edition. Blackwell Publishing Ltd. 2005 2. Beck JE. A Developmental Perspective on Functional Somatic Symptoms. Journal of Pediatric Psychology. 2008; 33(5): 547–562. 3. Garralda, M.E. A selective review of child psychiatric syndromes with a somatic presentation. Br J Psychiatry. 1992;161: 759-773 4. Beck JE. A Developmental Perspective on Functional Somatic Symptoms. Journal of Pediatric Psychology. 2008; 33(5) : 547–562. 5. Campo J V. Annual research review: Functional somatic symptoms and associated anxiety and depression - Developmental psychopathology in pediatric practice. J Child Psychol Psychiatry Allied Discip. 2012;53(5):575–92. 146 6. Fiertag O, Taylor S, Tareen A, Garralda E. Somatoform disorders. In Rey JM (ed), IACAPAP e-Textbook of Child and Adolescent Mental Health. Geneva: International Association for Child and Adolescent Psychiatry and Allied Professions 2012 7. Mullick MSI. Somatoform Disorders in Children and Adolescents. Bangladesh Med. Res. Counc. Bull. 2002; 28(3): 112-122 8. Bisht J, Sankhyan N, Krishan Kaushal R, Sharmi RC, Grover N. Clinical profile of pediatric somatoform disorders. Indian Pediatr 2007;45:111–5. 9. Coffelt TA, Bauer BD,Carroll AE. Inpatient Characteristics of the Child Admitted With Chronic Pain. Pediatrics. 2013; 132(2):e422-9 10. Deshpande SS, Ganapathy V, Bendre N. Psychosocial Morbidities In Children With Medically Unexplained Pain Symptoms: A Study From India. ASEAN J Psy. 2015;16(1): 11. Rask CU1, Olsen EM, Elberling H, Christensen MF, Ornbøl E, Fink P, Thomsen PH, Skovgaard AM. Functional somatic symptoms and associated impairment in 5-7year-old children: the Copenhagen Child Cohort 2000. Eur J Epidemiol. 2009;24(10):625-34. 12. Crimlisk HL, Bhatia K, Cope H, David A, Marsden CD,Ron MA. Slater revisited: 6 year follow up study of patients with medically unexplained motor symptoms. BMJ 1998; 316:582-6 147 13. Stone J, Carson A, Duncan R, Coleman R, Roberts R, Warlow C, et al. Symptoms ‘unexplained by organic disease’ in 1144 new neurology out-patients: How often does the diagnosis change at follow-up? Brain 2009;132(Pt 10):2878-88. 14. Konijnenberg AY, Uiterwaal CSPM, Kimpen JLL, van der Hoeven J, Buitelaar JK, de Graeff-Meeder ER. Children with unexplained chronic pain: substantial impairment in everyday life. Arch Dis Child 2005;90:680–6 15. Bohman H, Jonsson U, Von Knorring A, Von Knorring L, Paaren A, Olsson G. Somatic symptoms as marker for severity in adolescent depression. Acta Paediatrica. 2010; 99: 1724–30. 16. Dell ML, Campo JV. Somatoform Disorders in Children and Adolescents. Psychiatr Clin N Am 34 (2011) 643–660. 17. Sethi BB, Trivedi JK. Psychotherapy for the economically less privileged classes (with special reference to India). Indian J Psychiatry 1982;24:318-21. 18. Mohapatra S, Deo SJK, Satapathy A, Rath N. Somatoform Disorder in Children and Adolescents. German J Psychiatry. 2014;17(1): 19-24. 148 Bheemsain Tekkalaki, MD. Assistant Professor; Sameeran, S. Chate MD. Associate Professor; Nanasaheb M. Patil MD, Professor; Sandeep Patil MD. Assistant Professor. Department of Psychiatry, K.LE University’s J.N Medical College, Belagavi, Karnataka, India. Veerappa Y. Patil, MD. Post-Doctoral Fellow in Addiction Medicine, Department of Addiction Medicine, NIMHANS, Bengaluru. Jitendra Mugali MD. Assistant Professor, Department of Psychiatry, Gadag Institute of Medical Sciences, Gadag, Karnataka, India.