Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
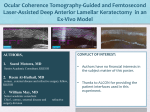
BASIC INVESTIGATION “Ultrathin” DSAEK Tissue Prepared With a Low–Pulse Energy, High-Frequency Femtosecond Laser Paul M. Phillips, MD,* Louis J. Phillips, OD,* Hisham A. Saad, MD,† Mark A. Terry, MD,‡§ Donna B. Stolz, PhD,¶ Christopher Stoeger, CEBT,§ Jonathan Franks, PhD,¶ and David Davis-Boozer, MPH§ Purpose: To evaluate the endothelial cell survival and stromal bed quality when creating deep stromal cuts with a low–pulse energy, high-frequency femtosecond laser to produce “ultrathin” tissue for Descemet stripping automated endothelial keratoplasty. Methods: Seventeen corneas were used for this study. Five corneas were cut with the laser at a depth of 420 to 500 mm to produce a tissue thickness of approximately #70 mm. Five corneas served as an uncut comparison group. Vital dye staining and computer digitized planimetry analysis were performed on these corneas. The 7 remaining corneas were cut for scanning electron microscopy evaluation. Results: The mean central posterior stromal thickness of cut corneas was 60.6 mm (range, 43–72 mm). Endothelial cell damage in cut and comparison corneas was 3.92% ± 2.22% (range, 1.71%– 6.51%) and 4.15% ± 2.64% (range, 1.21%–7.01%), respectively (P = 0.887). Low-magnification (·12) scanning electron microscopy revealed a somewhat irregular-appearing surface with concentric rings peripherally. Qualitative grading of higher magnification (·50) central images resulted in an average score of 2.56 (between smooth and rough). Conclusions: Ultrathin tissue for Descemet stripping automated endothelial keratoplasty can be safely prepared with minimal endothelial cell damage using a low–pulse energy, high-frequency femtosecond laser; however, the resulting stromal surface quality may not be optimal with this technique. Key Words: Descemet stripping automated endothelial keratoplasty, Descemet stripping endothelial keratoplasty, endothelial keratoplasty, femtosecond laser, ultrathin DSAEK, endothelium (Cornea 2012;0:1–6) Received for publication January 31, 2012; revision received April 2, 2012; accepted April 18, 2012. From the *Sightline Ophthalmic Associates, Sewickley, PA; †Tanta University Faculty of Medicine, Tanta, Egypt; ‡Devers Eye Institute, Portland, OR; §Lions VisionGift, Portland, OR; and ¶University of Pittsburgh School of Medicine, Center for Biologic Imaging, Pittsburgh, PA. The authors state that they have no financial or conflicts of interests to disclose. Reprints: Paul M. Phillips, Sightline Ophthalmic Associates, Suite 104, 2591 Wexford-Bayne Rd, Sewickley, PA 15143 (e-mail: paulphillipsmd@ gmail.com). Copyright © 2012 by Lippincott Williams & Wilkins Cornea Volume 0, Number 0, Month 2012 D escemet stripping automated endothelial keratoplasty (DSAEK) is currently the surgical standard of care for the treatment of endothelial failure. Although there is no question regarding the efficacy of this surgery, which results in the vast majority of patients with best spectacle-corrected acuity of 20/40 or better,1–4 there has been a great deal of debate regarding the cause for the relatively small percentage of patients achieving 20/20 vision despite beautifully clear postoperative corneas. One theory is that the added stromal thickness resulting from DSAEK surgery may have some bearing on the final visual acuity and that the use of very thin donor tissue, also referred to as “ultrathin” tissue, may result in better outcomes. Currently, there is no precise definition of ultrathin tissue, but most surgeons would consider such tissue to be 100 mm or thinner. Despite the lack of clear evidence at this time to support the notion that thinner tissue yields better visual outcomes in DSAEK, some surgeons argue that this ultrathin tissue may result in both faster vision recovery and better final visual acuity. Thinner tissue may also theoretically allow for less crushing of tissue when using new injector systems. Many surgeons are now attempting to produce such tissue for their surgeries or are requesting that eye banks produce this ultrathin tissue for their use. With advancing femtosecond technology, allowing for much deeper stromal cuts, it may now be possible to produce ultrathin DSAEK tissue using this technology. One concern regarding the use of a femtosecond laser to cut such thin tissue is that the laser’s photodisruption process may be damaging to the endothelium when cutting close to the delicate cells. There is some evidence that this may be the case when cutting within around 100 mm of the endothelium using the Intralase (Abbott Medical Optics, Abbott Park, IL) femtosecond laser.5 Additionally, although femtosecond lasers may make smoother laser in situ keratomileusis flaps than microkeratomes when cutting at depths of 110 to 140 mm,6 some studies have shown that when cutting deeper (300–400 mm), the stromal surface appears to be rougher with the laser than with the microkeratome.7,8 To date, no study has been published looking at endothelial survival when cutting ultrathin grafts of 70-mm thickness. Additionally, no study has looked at stromal bed quality when using a low–pulse energy, high-frequency (LPEHF) femtosecond laser (Ziemer Femto LDV; Ziemer Ophthalmic Systems, Port, Switzerland). Theoretically, this high-frequency laser (.5 MHz), which uses closely www.corneajrnl.com | 1 Cornea Volume 0, Number 0, Month 2012 Phillips et al overlapping spot and line separation, may lead to a smoother bed, although at the same time, through a low pulse energy (,100 nJ), avoid damage to the nearby endothelium. The goal of this study, therefore, was to evaluate both endothelial survival and stromal bed quality when using an LPEHF femtosecond laser to cut ultrathin tissue at an approximate thickness of 70 mm. MATERIALS AND METHODS Donor Tissue Seventeen corneoscleral buttons unsuitable for transplantation were supplied by the Lions VisionGift. All samples were free of gross deformities and generally clear optically. Ten corneas were chosen to have reasonably good endothelial cell counts (1736–3135 cells/mm2) and were used for the endothelial cell survival analysis. Of these, 5 corneas were cut up to depths of 420 to 500 mm to produce ultrathin tissue of approximately #70 mm, and 5 corneas were used as uncut comparisons. An additional 7 corneas were cut at depths of 450 to 500 mm for a goal depth of approximately #70 mm for evaluation with scanning electron microscopy (SEM) to determine the stromal bed quality produced by these deep cuts. Femtosecond Laser Protocol The endothelium of the donor button was coated with Healon 10 (Abbott Medical Optics), and the donor button was secured onto the Ziemer artificial anterior chamber (AAC; Ziemer Ophthalmic Systems). The chamber was then infused with balanced salt solution (BSS) through an intravenous line at a bottle height of ;80 cm above the base of the anterior chamber maintainer to achieve a moderately firm pressure by tactile tension, and the infusion line was clamped closed. The corneal thickness was measured with a Sonogage ultrasonic pachymeter (Sonogage, Cleveland, OH), and the epithelium was wiped clear of the surface with a blunt spatula and Merocel sponge (Beaver-Visitec International, Waltham, MA). The central corneal thickness was again measured with the pachymeter. To get precise diameter measurements, the laser head was applied to the Ziemer AAC above the surface of the dry cornea. The head was then lowered by turning the peripheral ring of the AAC clockwise until the central part of the cornea touched the Intershield. The ring was turned until the applanated surface, shown on the monitor of the laser, reached the goal diameter of 9.5 mm. The laser head was then removed, and Healon was applied to the cornea in a peripheral ring of ;6 mm and BSS applied centrally. A laser Intershield was then chosen and applied to the laser head based on this “epi-off ” pachymetry measurement to achieve a depth that would most likely result in the desired target goal of a residual stromal bed of #70 mm. The laser head was then gently reapplied to the cornea on the AAC and the laser cut then created. The entire process from the point of application of the laser shield to the cornea until removal after treatment took 45 seconds. The identical procedure was followed for uncut comparison corneas, including mounting them onto the 2 | www.corneajrnl.com AAC and applying the laser head to the surface of the corneas for the same 45 seconds to simulate the laser treatment, but in these comparison cases the laser was not fired. Once the laser procedure was performed, the interface was entered with a Thorlakson spatula (Katena Products, Inc, Denville, NJ), and the flap was separated and lifted from the posterior stromal bed. In the case of the 5 cut corneas used for endothelial analysis, the caps were then replaced, and all 10 corneoscleral rims placed back into the Optisol storage chambers. These 10 corneas used for endothelial analysis (5 comparisons and 5 study eyes) were sent back to the eye bank where the posterior stromal bed thickness was measured using an Optovue optical coherence tomographer (Optovue, Inc, Fremont, CA), before performing the endothelial cell analysis (see following). In the case of the 7 corneas sent for electron microscopy, the caps were removed after laser cutting, and the corneoscleral rims were immediately placed in the fixative. The corneoscleral rims were then placed in buffer solution and dehydrated in ascending concentrations of ethanol. They were treated with hexamethyldisilazane and air-dried. They were attached to aluminum SEM stubs with colloidal graphite and were coated with gold–palladium. They were then viewed with a JEOL JEM-6335F transmission electron microscope (JEOL Ltd, Tokyo, Japan). The total bed surface was observed at ·12 magnification, whereas the central area was observed at ·50 magnification. Staining and Quantification of Endothelial Damage The tissues sent for endothelial analysis were removed from the Optisol-GS storage chamber, rinsed with BSS, and trephinated with an 8-mm punch. They were then stained with 0.25% trypan blue (MP Biomedicals, LLC, Solon, OH) and 0.2% alizarin red S (GFS Chemicals, Inc, Columbus, OH). The technique used for vital dye staining was identical to that described in a previous study.9 After vital dye staining, quantitative analysis of the endothelial damage was performed. The graft was placed in BSS within a clear vial and mounted on the slit lamp and photographed at ·16 magnification. Illumination was adjusted to avoid shadows or excessive light reflections. The image then underwent planimetry quantitative processing using Adobe Photoshop 7.0 software as described previously.9 The number of pixels that made up the stained area was determined, and this was divided by the number of pixels making up the entire endothelial area, thus giving a percentage of the endothelial damage. The reproducibility of this technique has been previously established.9,10 Statistical Analysis All data were analyzed using SPSS version 19.0. An independent samples t test was used to compare cell loss between study and comparison eyes. Power analyses were performed using G*Power 3. 2012 Lippincott Williams & Wilkins Cornea Volume 0, Number 0, Month 2012 Ultrathin DSAEK Tissue With Femtosecond Laser TABLE 1. Laser Settings and Pre- and Postlaser Corneal Thickness Measurements Donor Cornea 1 2 3 4 5 Epi-Off Pachymetry* (mm) Laser Cut Depth (mm) Anticipated Residual Bed (mm) Achieved Residual Bed, OCT† (mm) Error (mm) 453 465 509 581 516 420 420 500 500 500 33 45 9 81 16 61 72 63 64 43 +28 +27 +54 217 +27 *Prelaser measurements performed with a pachymeter preoperatively. †Postlaser, posterior lenticule bed thickness measurements taken with optical coherence tomography (OCT) postoperatively. Grading of Stromal Smoothness The SEM images of the central stromal surface of the resulting posterior corneoscleral buttons (·50) were subjectively graded by 3 masked independent observers in a manner similar to that of Cheng et al.11 The smoothness of the central stromal surfaces imaged at ·50 were graded on the following scale: 1 = very smooth, 2 = smooth, 3 = rough, and 4 = very rough. of 3.92% ± 2.22% (range, 1.71%–6.51%) and 4.15% ± 2.64% (range, 1.21%–7.01%), respectively (P = 0.887; Fig. 1). The resulting effect size for the groups before removal of trephination damage (overall damage) and for the groups with trephination damage removed was extremely small (Cohen d = 0.095 and 0.09, respectively). As a result, a priori power calculations using the means and standard deviations above show that this study lacks the power needed to detect this very small effect, which would require a sample of .1000 to gain the appropriate statistical power. RESULTS Laser Cutting Accuracy Stromal Bed Quality The intended laser cut depths chosen ranged from 420 to 500 mm resulting in an average residual stromal bed thickness in the 5 study corneas of 60.6 mm (range, 43–72 mm). There was an average deviation from expected target results of 30.6 mm (range, 217 to 54 mm; Table 1). On low-magnification inspection, some of the corneas had noticeable concentric ring irregularities, but this pattern was not seen uniformly (Fig. 2). In these corneas with concentric ring formation, the rings were seen peripherally, whereas the central 2 to 4 mm seemed uninvolved. Grading of the central stromal bed smoothness was performed at high magnification (·50) with a subjective grading scale that resulted in an average grading of all 5 corneas of 2.56 (range, 1.33–4.0, SD = 1.03). This grading fell between “smooth” and “rough” on a 4-point grading scale of “very smooth” to “very rough” (Fig. 3). Endothelial Analysis Endothelial cell analysis did not reveal a statistically significant difference between the study and comparison groups. Overall, cell damage for cut and comparison corneas was 8.4% ± 3.6% (range, 4.88%–13.26%) and 8.7% ± 2.4% (range, 6.05%–11.26%), respectively (P = 0.855). When damage occurring from trephination was removed, the results continued to demonstrate no statistically significant difference between cut and comparison corneas, with a damage cell area DISCUSSION Although good prospective studies are required to validate the theory that the use of ultrathin DSAEK grafts FIGURE 1. Vital dye staining and computer digitized planimetry analysis of endothelial cell damage resulting from laser procedure (corneas 1–5) and comparison procedure (corneas 6–10) after corneal trephination damage was removed. *No significant difference was found at 3.92% (range, 1.71%–6.51%) and 4.15% (range, 1.21%–7.01%), respectively (P = 0.887). 2012 Lippincott Williams & Wilkins www.corneajrnl.com | 3 Phillips et al Cornea Volume 0, Number 0, Month 2012 FIGURE 2. SEM low-magnification (·12) postlaser images demonstrating an example of a generally smooth bed (cornea F) as compared with a rougher bed with characteristic concentric ring (arrows) formation (cornea G). can achieve better vision outcomes than standard DSAEK grafts, surgeons have begun requesting thin DSAEK tissue from eye banks (J. Clover B.S., C.E.B.T, Lions VisionGift, Oregon, Personal communications, November 2011). The use of a femto- second laser to create such tissue may prove to be a viable method because these lasers can cut to depths of up to 500 mm. This study was designed to provide preliminary evidence to determine whether such deep cuts can be made effectively and safely. FIGURE 3. SEM high magnification (·50) of central corneal images of all 7 study corneas. The stromal bed quality grading score (average) of each image is noted in parentheses. Grading was on a scale of 1 to 4 (very smooth = 1, smooth = 2, rough = 3, and very rough = 4). 4 | www.corneajrnl.com 2012 Lippincott Williams & Wilkins Cornea Volume 0, Number 0, Month 2012 We believe that the laser does cut relatively accurately at depths of 450 to 500 mm, with a deviation from expected targeted depths of 30.6 mm. A larger study would be necessary to determine if this deviation is consistent, however. Our study does demonstrate that the use of a low–pulse energy (,100 nJ), high-frequency (,5 MHz) laser, to cut deep within the stroma and close to the endothelium, does not result in significant amounts of cell loss or death. Although we did not find a statistically significant difference between the cut corneas and corneas of the uncut comparison group, as noted previously, this study was not powered to detect the very small difference found between the groups. It is important to note, however, that with such a small effect size, it would take an impractically large study (.1000 corneas) to detect this difference. We feel that it is reasonable though to consider that the 0.3 percentage points between the groups before removing the trephination damage and the 0.23 percentage points between the groups after the trephination damage was removed are not likely to be clinically significant. This is even more evident when considering the fact that the cell damage that did occur was variable, with no repeatable pattern observed. Specifically, because the Ziemer laser pulses are applied in a linear fashion, occurring from left to right across the cornea, cell death resulting from these pulses then would be expected to follow such a pattern along the endothelium, which was not noted in any of the study corneas. Although the lack of cell death does give promise for the possible use of this technology, the resulting stromal bed may not be ideally smooth. In some of the study corneas, there seemed to be a concentric ring pattern in the stromal bed, which has been described in a previous study.12 This concentric ring pattern is likely the result of an applanation effect of the laser deforming the posterior stoma more than the anterior stroma. It is unclear, however, why some tissues in this study developed these concentric rings, whereas the others did not. It is possible that this may be caused by different amounts of corneal rigidity either inherent in the individual donor corneas or, alternatively, because of differing amounts of stromal hydration of individual corneas. Although the cause of the concentric rings is speculation, it is also unclear whether these concentric rings would significantly affect vision outcomes because they mostly tended to be more pronounced in the periphery. The central stroma appeared more reasonably smooth, with subjective grading of the resulting central bed falling between smooth and rough, at an average score of 2.6. This was similar to that found in previous studies (average score of 2.8) when cutting less deep (400 mm) within the stroma with a 60-kHz laser.11 As noted previously, this irregular-resulting stroma may be a result of the loosely arranged collagen deep within the cornea.12 If loosely arranged posterior collagen results in a rougher stromal bed, then it might also be expected that a rougher stromal surface would occur when using the “double-pass” microkeratome technique for the creation of ultrathin tissue, as developed by Busin.13 To our knowledge, though, there has been no study reporting on an electron microscopy evaluation of the stromal bed quality created with the double-pass technique. Therefore, at this 2012 Lippincott Williams & Wilkins Ultrathin DSAEK Tissue With Femtosecond Laser time, a comparison cannot be made between the stromal bed quality created with the double-pass technique and our current technique. Alternatively, the irregular stroma may be a result of the increased scatter and attenuation of laser efficacy at this greater depth in edematous corneas.12 A double cut or triple cut with the femtosecond laser has been demonstrated to result in a smoother stromal bed when cutting standard DSAEK tissue at depths of 350 mm with a 40-kHz laser.14 This double-cut technique was also demonstrated in another recent study to improve stromal bed quality with a 60- and 150-kHz laser. In this recent study, it was demonstrated that a more ideal stromal bed quality was achieved with a doublelayer profile technique that involved first cutting at a depth of 350 mm, followed by a second cut at a depth of 150 mm. The authors argued that this result was achieved by avoiding the diffraction and optical aberrations occurring when cutting deep (400–500 mm).15 Such double-cut and double-layer profile techniques were not attempted in the current study and may improve stromal quality while potentially not increasing endothelial damage. Further studies would be required to validate or refute this theory. In conclusion, the use of the LPEHF laser to create ultrathin DSAEK tissue holds promise, as seen in our study, that this laser can reliably create ultrathin DSAEK tissue without causing significant damage to the delicate endothelium. Modification of energy settings and cutting techniques may improve the final stromal bed quality, which should be the focus of future studies. REFERENCES 1. Bahar I, Kaiserman I, McAllum P, et al. Comparison of posterior lamellar keratoplasty techniques to penetrating keratoplasty. Ophthalmology. 2008;115:1525–1533. 2. Chen ES, Terry MA, Shamie N, et al. Descemet-stripping automated endothelial keratoplasty: six-month results in a prospective study of 100 eyes. Cornea. 2008;27:514–520. 3. Price MO, Baig KM, Brubaker JW, et al. Randomized, prospective comparison of precut vs surgeon-dissected grafts for Descemet stripping automated endothelial keratoplasty. Am J Ophthalmol. 2008; 146:36–41. 4. Price MO, Price FW Jr. Descemet’s stripping with endothelial keratoplasty: comparative outcomes with microkeratome-dissected and manually dissected donor tissue. Ophthalmology. 2006;113: 1936–1942. 5. Sikder S, Snyder RW. Femtosecond laser preparation of donor tissue from the endothelial side. Cornea. 2006;25:416–422. 6. Sarayba MA, Ignacio TS, Binder PS, et al. Comparative study of stromal bed quality by using mechanical, IntraLase femtosecond laser 15- and 30-kHz microkeratomes. Cornea. 2007; 26:446–451. 7. Jones YJ, Goins KM, Sutphin JE, et al. Comparison of the femtosecond laser (IntraLase) versus manual microkeratome (Moria ALTK) in dissection of the donor in endothelial keratoplasty: initial study in eye bank eyes. Cornea. 2008;27:88–93. 8. Mootha VV, Heck E, Verity SM, et al. Comparative study of Descemet stripping automated endothelial keratoplasty donor preparation by Moria CBm microkeratome, horizon microkeratome, and Intralase FS60. Cornea. 2011;30:320–324. 9. Saad HA, Terry MA, Shamie N, et al. An easy and inexpensive method for quantitative analysis of endothelial damage by using vital dye staining and Adobe Photoshop software. Cornea. 2008;27: 818–824. www.corneajrnl.com | 5 Phillips et al 10. Terry MA, Saad HA, Shamie N, et al. Endothelial keratoplasty: the influence of insertion techniques and incision size on donor endothelial survival. Cornea. 2009;28:24–31. 11. Cheng YY, Kang SJ, Grossniklaus HE, et al. Histologic evaluation of human posterior lamellar discs for femtosecond laser Descemet’s stripping endothelial keratoplasty. Cornea. 2009;28:73–79. 12. Soong HK, Mian S, Abbasi O, et al. Femtosecond laser-assisted posterior lamellar keratoplasty: initial studies of surgical technique in eye bank eyes. Ophthalmology. 2005;112:44–49. 6 | www.corneajrnl.com Cornea Volume 0, Number 0, Month 2012 13. Busin M. One-year results of the double-pass technique for ultrathin DSAEK. Paper presented at: Cornea Society/EBAA Fall Symposium; October 11, 2011; Orlando, FL. 14. Mehta JS, Parthasarthy A, Por YM, et al. Femtosecond laserassisted endothelial keratoplasty: a laboratory model. Cornea. 2008; 27:706–712. 15. Rousseau A, Bensalem A, Garnier V, et al. Interface quality of endothelial keratoplasty buttons obtained with optimised femtosecond laser settings. Br J Ophthalmol. 2012;96:122–127. 2012 Lippincott Williams & Wilkins