Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
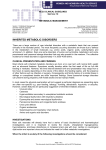
ORIGINAL ARTICLE Spectrum of Inherited Metabolic Disorders in Pakistani Children Presenting at a Tertiary Care Centre ABSTRACT Huma Arshad Cheema, Hassan Suleman Malik, Arit Parkash and Zafar Fayyaz Objective: To determine the frequency, presentation and outcome of various inherited metabolic diseases in children presenting in a tertiary care hospital, Lahore, Pakistan. Study Design: An observational study. Place and Duration of Study: Gastroenterology, Hepatology and Nutrition Department of The Children Hospital and Institute of Child Health, Lahore, from January 2011 to October 2014. Methodology: All children aged < 14 years with high suspicion of a metabolic disorder were inducted. Routine and radiological investigation were carried out at the study place. Comprehensive diagnostic testing of particular metabolic disorder was sent abroad. Those with a specific metabolic disorder were included in the study while those with normal metabolic work-up were excluded. All data was collected on preformed proforma. Results: A total of 239 patients were enrolled. Nineteen different types of inherited metabolic disorders were diagnosed in 180 patients; age ranged from 8 days to 14 years. Consanguinity was positive in 175 (97%) among the parents of the affected children, with previously affected siblings in 64 (35.5%). The most frequent disorders were inherited disorders of carbohydrate metabolism (92, 51%), lipid storage disease (59, 32.7%), organic acidemia and energy defects (18, 10%), amino acid disorder (6, 3.3%), and miscellaneous (4, 2.2%). Fifty-eight (32.2%) presented with acute metabolic crisis, 28 (15.5%) patients presented with early onset liver failure, and 24 (13.3%) with mental retardation. Out of these, 16 (8.8%) expired. Conclusion: Glycogen storage disorders being the commonest followed by Gaucher disease and Galactosemia. The associated complications resulted in high morbidity and mortality. Key Words: Metabolic disorders. Gaucher's disease. Galactosemia. Pakistan. INTRODUCTION Metabolic diseases or inborn errors of metabolism (IEM) are significant cause of mortality and morbidity among children in both the developed and developing countries. The variety and complexity of IEM along with diverse clinical pictures present a formidable challenge to the treating paediatrician. At the same time, prevention of death or severe neurological sequelae is dependent on prompt and early diagnosis. These inherited disorders are caused by genetic mutations leading to defective protein function. Most are inherited in autosomal recessive pattern and few are X-linked recessive disorders. In Pakistan, it is reported that more than half of all marriages (56%) are between first and second cousins.1 Consanguinity increases the risk of these rare genetic recessive disorders.2 The prevalence of IEM in various countries varies between 1 in 800 to 1 in 5000.3 In one study from UK, Department of Gastroenterology, Hepatology and Nutrition, The Children Hospital and Institute of Child Health, Lahore. Correspondence: Prof. Dr. Huma Arshad Cheema, Head of the Department of Gastroenterology, Hepatology and Nutrition, The Children Hospital and Institute of Child Health, Lahore. E-mail: [email protected] Received: March 09, 2015; Accepted: January 23, 2016. 498 the overall incidence of recorded IEM was 10-fold greater among Pakistanis compared to white children (1:318 vs. 1:3760). Tyrosinemia type-1, cystinosis, mucopolysaccharidosis type-1, non-ketotic hyperglycinemia and hyperchylomicronaemia, all occurred more frequently among the Pakistanis.4 There is no reported study regarding incidence of metabolic disorders from Pakistan. That may be, in large part, due to non-availability of comprehensive testing for diagnosis of these disorders. The objective of this study was to determine frequency, presentation and outcome of various inherited metabolic diseases in children presenting in a tertiary care hospital in Lahore, Pakistan. METHODOLOGY It was an observational study conducted at the Department of Paediatric Gastroenterology and Hepatology at The Children's Hospital, The Institute of Child Health, Lahore, and included all children with high suspicion of a metabolic disorder (inborn errors of metabolism) from November 2011 to October 2014. Complete history, physical examination and routine specific laboratory investigations were recorded. Routine laboratory investigations included: CBC, blood sugar, serum electrolytes, anion gap, serum calcium, PT, Journal of the College of Physicians and Surgeons Pakistan 2016, Vol. 26 (6): 498-502 Spectrum of inherited metabolic disorders in Pakistani children presenting at a tertiary care centre APTT, liver and renal function tests, arterial blood gas, serum ammonia, urinary ketones, C-reactive protein, blood, and urine culture. Specific comprehensive testing was done according to clinical suspicion. Skeletal survey was done in suspected patients of mucopolysaccharides (MPS) and Gaucher's disease. Bone marrow biopsy and eye examination was done in suspected lipid storage disorders. Liver biopsies were done in suspected cases of glycogen storage disease (GSD). All these routine, radiological and histological investigations were carried out at the study centre. As facility of comprehensive diagnostic testing of particular metabolic disorder is not available there, so these were sent abroad. Three ml each of heparinized blood, EDTA, and clotted sample for serum, dried blood spot on filter paper, and 20 ml of urine were saved before starting of management and sent abroad urgently after explaining and taking written consent from parents in clinically suspected cases. DBS for suspected Gaucher and various verities of MPS was done. Enzyme assay for galactosemia, biotinidase deficiency and other disorders was done wherever indicated. Blood tandem mass spectrometry (TMS) for amino acid and acyl carnitine levels, blood and urine amino acid levels by HPLC or chromatography, urine organic acids analysis by GCMS and urine mucopolysaccharides and oligosaccharides was carried out from abroad in clinically suspected cases. All the relevant data including demographics, clinical presentation and outcome was filled in pre-designed proforma. SPSS Statistics version 19.0 was used to analyze the data. Descriptive statistics has been used for computing frequency and percentage. On diagnosis, the specific nutritional intervention was discussed with an expert dietician before being implemented. Constant monitoring during the diet was done with frequent counselling of parents. Written information was given to parents in Urdu (local language). RESULTS disorder 6 (3.3%), and miscellaneous 4 (2.2%). Fiftyeight (32.2%) patients presented with metabolic crisis, 28 (15.5%) with neonatal cholestasis and 24 (13.3%) had mental retardation. Out of these, 16 (8.8%) expired (tyrosinemia n=5, GSD n=4, Gaucher’s disease n=4 and methyl-melonic-academia (MMA) n=3). Table I describes the etiologies of hereditary metabolic disorders with frequencies and percentages (n=180). Figure 1 describes the frequency distribution of the types of Gaucher's disease and Figure 2 describes the same of MPS. Table I: The etiologies of hereditary metabolic disorders with frequencies and percentages (n=180). Inherited metabolic disorder A-Carbohydrate disorders 1.Glycogen storage disease 2.Galactosemia 3.Fructose 1,6- bisphosphatase deficiency (FDPase) B-Lysosomal storage disease 1.Gaucher’s disease 2.Mucopolysaccharides (MPS) Sub-types MPS-1 n=8, MPS -II n=2, MPS-IV n=6 and MPS-VI n=1 3.Mucolipidosis-II 4.Niemenn pick disease 5.Sialidosis (Mucolipidosis-1) 6.Pompe disease C- Organic acid and energy metabolism defects 1.Mitrochondriopathy 2.Fatty acid oxidation defect (FAOD) 3.Methylmalonic acidemia (MMA) Number (%) 92 (51%) 62 (67.4%) 22 (24%) 8 (8.6%) 59 (32.7%) 32 (54.2%) 17 (28.8%) 3 (5%) 3 (5%) 2 (3.5%) 2 (3.5%) 18 (10%) 8 (44.5%) 4 (22.25%) 3 (16.5%) 4.Biotidinase deficiency 1 (5.5%) 6. 3-Hydroxymethylglutaryl-coa (3-hmg coa) lyase deficiency 1 (5.5%) 5.2-Methyl-2-hydroxybutyric aciduria (MHBD) D-Amino acid disorders 1 (5.5%) 6 (3.3%) 1.Hereditary Tyrosinemia 6 (100%) 1.Neonatal hemochromatosis 2 (50%) 3. Lysinuric protein intolerance 1 (25%) E- Miscellaneous 2.Bile acid synthesis defect (BASP) 4 (2.2%) 1 (25%) A total of 239 subjects were enrolled in the study, out of which 180 (75.3%) tested positive for a specific metabolic disorder while 59 (24.7%, male=38 and female=21) had normal metabolic work-up. Out of 180 subjects, who were tested positive for metabolic disease, male predominance was noted 62.2% (n=112) and females were 37.8% (n=68). Nineteen different types of inherited metabolic disorders were diagnosed. Age ranged from 1 day to 14 years. Consanguinity was positive among parents of 175 (97%) affected children. Family history of previously affected children was noted in 64 (35.5%). Inherited disorder of carbohydrate metabolism topped the list in order of frequency with n=92 (51%), followed by lipid storage disorder 59 (32.7%), organic acidemia and energy deficient defects 18 (10%), amino acid Figure 1: Types of Gaucher's disease (n=32). Journal of the College of Physicians and Surgeons Pakistan 2016, Vol. 26 (6): 498-502 499 Huma Arshad Cheema, Hassan Suleman Malik, Arit Parkash and Zafar Fayyaz screened among whom 2.65% were diagnosed to be having specific IEM.10 In this study consanguinity rate was present in 97%. This is comparable to a study from Libya where consanguinity was observed in 86.9%.9 Family history of previously affected children was noted in 35.5% in this study as compared to the Libyan study where family history of the disorder was noted in 63.5% of cases.11 In this study, GSD was the commonest disorder in the studied population followed by Gaucher’s disease, galactosemia and MPS with frequency of 34.4%, 17.7%, 12.2% and 9.4%, respectively. In contrast, frequencies of 23%, 6%, 4% and 20%, respectively have been reported of these disorders by Roy et al. from India.12 Figure 2: Types of MPS disease (n=17). DISCUSSION Metabolic disorders are group of inherited disorders that cause significant morbidity and mortality. Archibald Garrod in 1909 introduced the concept of inborn errors of metabolism (IEM).5 These are congenital metabolic disorders, caused by genetic mutations leading to defective protein function, resulting in the absence or abnormality of an enzyme or cofactor, causing either accumulation or deficiency of a specific metabolite. Outcome depends upon recognition of the signs and symptoms, timely evaluation, and transfer to facility which is familiar with the evaluation and comprehensive testing along with experience of management of these disorders. Any delay in diagnosis can lead either early death or significant morbidity in the form of neurological deficit. Majority of severe forms of metabolic disorders present in childhood. Most paediatricians have to face these disorders; hence they should have experience in diagnosing and treating these diseases. Moreover, improved and available treatments which include enzyme replacement therapy (ERT), toxic substrate inhibitors and diet restrictions have changed the prognosis of some of these diseases. Possible improved outcome increase the importance of recognizing these disorders. In this study, the authors found variety of patients of metabolic disorders including rare disorders. Individual IEM are rare disorders, most having reported incidence of less than 1 per 100,000 births. However, the incidence may approach 1 in 800 - 2500 births when considered collectively.6,7 Incidence of metabolic diseases in Pakistan is not known. In studies from Pakistan, IEMs were confirmed in 5/10 (50%)8 cases at the Shifa International Hospital, Islamabad, and in 16/62 (26%) cases at National Institute of Child Health, Karachi.9 In a study from India, 869 cases were 500 Patients from group of organic acids and energy deficient defects disorders mainly presented with metabolic crisis. We had 4 cases of falty acid oxidation defect (FAOD). Huang et al. described 8 cases of FAOD in his study in which 11,060 patients were screened.13 Biotinidase deficiency has already been reported from Pakistan, one case reported from Islamabad and 4 cases reported from Karachi.6,13 In this study, a very rare disorder 2-m Methyl-3-hydroxybutryl CoA dehydrogenasee (MHBD) was also found, which was reported previously only in less than 10 cases in literature.15,16 One case of 3-hydroxymethylglutaryl-CoA (3-hmg CoA) lyase deficiency was diagnosed, this type of organic acidemia occurs without ketogenesis. This is a very rare disorder and there are few published case reports of this disorder in literature.17,18 There was a case of lysinuric protein intolerance; approximately 140 individuals with this disorder have been reported in literature.19 In this study, 24 (13.3%) patients had mental retardation. In a recent study, 81 IEMs were described to have intellectual delay as a clinical feature.20 In a study from Libya, 87.5% of children were developmentally delayed which is higher as compared to our study.11 Children presenting with MMA and tyrosinemia had the worst prognosis even with early treatment, all 3 patients of MMA and 5 patients of tyrosinemia expired. Four patients of GSD expired who came with severe crisis and reached hospital late. Four patients of Gaucher’s disease expired; out of these 3 patients were of type-I and died of severe cachexia, bleeding and infections, while another patient of type-II died of severe neurological involvement (seres, squint, and bulbar palsy). In Pakistani population, owing to high rate of intermarriages and large family size, our assumption that these metabolic disorders including rare disorders, all are prevalent in Pakistan, seems to be true. One hundred and eighty (180) cases of 19 different disorders were found in this study. The diagnosis of inherited metabolic disorders has increased in recent years in our country. Some centres have initiated work-up and Journal of the College of Physicians and Surgeons Pakistan 2016, Vol. 26 (6): 498-502 Spectrum of inherited metabolic disorders in Pakistani children presenting at a tertiary care centre management of these disorders. But there is a lack of therapeutic and diagnostic resources, including metabolic laboratories, confirmatory DNA testing, specialist in this field, and specialized metabolic dietitians. For this study, the authors had to send samples for diagnostic work-up to a laboratory in another country. Most of diagnoses were made on the basis of enzyme assay and substrates analysis, whereas, genetic mutations are not being done. The authors were unable to gather data for the type of mutations prevalent in this population. Gene analysis has significantly improved prenatal diagnosis and identification of healthy heterozygotes, thus significantly improving importance and application of genetic counselling.21 Without knowledge of these mutations, antenatal diagnosis is not possible. In the last decade, introduction of tandem mass spectrometry has expanded newborn screening (NBS). Now, this programme is mandatory in most of the developed and developing countries as a public health strategy.22 In Pakistan, however, neonatal screening programme is not available. There is a need of creating local facilities for diagnosing these disorders and awareness of primary as well as tertiary care level for proper referral, as most cases of crisis are treated as sepsis, mental retardation and cerebral palsy, and there is no further evaluation and proper management. This study provides valuable information for future metabolic newborn screening programme, which is treatable; and most frequent metabolic disorders should be considered for screening. To treat acute and life-threatening cases in the treatment of metabolic disorders, the priority was given to manage intoxication. However, the treatment for lysosomal diseases like Gaucher's disease and MPS, where enzyme replacement therapy is available and in vogue, paediatricians should make themselves familiar with these sophisticated regimens.23 Dietary management is essential for metabolic disorders. Dietitians in association with metabolic specialists should make plans for protein restricted or modified diet for these patients and must provide adequate nutrition to them. Diets normally consist mainly of special medical milk formulas for specific disorders and selective natural foods. Cost, unavailability of drugs, poor medical and nutritional compliance reduce the efficacy of treatment in population of developing countries. Inherited metabolic disorders were not only common in first cousin marriages but also in non-cousin marriages of the same caste. Arian was the most commonly affected caste showing IEM. CONCLUSION Different types of rare disorders were diagnosed with glycogen storage disorders being the commonest, followed by Gaucher's disease and galactosemia. This study highlights the presence of various metabolic disorders in Pakistan and the need for starting a newborn screening program to include most frequent and treatable disorders such as Gaucher’s disease, galactosemia, MPS, fructose1, 6-bisphosphatase deficiency, FAOD, Pompe’s disease and biotinidase deficiency. REFERENCES 1. National Institute of Population Studies (NIPS). Pakistan demographic and health survey 2006-07. Islamabad: National Institute of Population Studies and Macro International Inc; 2008. 2. Saggar AK. Consanguinity and child health. Paediatr Child Health 2008; 18:244-9. 3. Pandey AS. Metabolic disease in Nepal: A perspective. Kathmandu Univ Med J 2010; 8:333-40. 4. Hutchesson AC, Bundey S, Preece MA, Hall SK, Green A. A comparison of disease and gene frequencies of inborn errors of metabolism. J Med Genet 1998; 35:366-70. 5. Scriver CR, Beaudet AL, Sly WS, Valle D, Childs B, Kinzler KW, et al. editors. The metabolic and molecular bases of inherited disease. 8th ed. New York; McGraw-Hill; 2001. 6. Applegarth DA, Toone JR, Lowry RB. Incidence of inborn errors of metabolism in British Columbia, 1969-1996. Pediatrics 2000; 105:e10. 7. Sanderson S, Green A, Preece MA, Burton H. The incidence of inherited metabolic disorders in the West Midlands, UK. Arch Dis Child 2006; 91:896. 8. Choudhry S, Khan M, Rao HA, Jalan A, Khan EA. Etiology and outcome of inborn errors of metabolism. J Pak Med Assoc 2013; 63:1112-6. 9. Satwani H, Raza J, Hanai J, Nomachi S. Prevalence of selected disorders of inborn errors of metabolism in suspected cases at a tertiary care hospital in Karachi. J Pak Med Assoc 2009; 59:815-9. 10. Rao AN, Kavitha J, Koch M, Kumar S. Inborn errors of metabolism: review and data from a tertiary care center. Indian J Clin Biochem 2009; 24:215-22. 11. AlObaidy H. Patterns of inborn errors of metabolism: a 12-year single-center hospital-based study in Libya. Qatar Med J 2013; 18:1-9. 12. Roy A, Samanta T, Purkait R, Mukherji A, Ganguly S. Etiology, clinical spectrum and outcome of metabolic liver diseases in children. J Coll Physicians Surg Pak 2013; 23:194-8. 13. Huang X, Yang L, Tong F, Yang R, Zhao Z. Screening for inborn errors of metabolism in high-risk children: a 3-year pilot study in Zhejiang Province, China. BMC Pediatrics 2012; 12:18. 14. Afroze B, Wasay M. Diagnosis, treatment and follow-up in four children with biotinidase deficiency from Pakistan. J Coll Physicians Surg Pak 2013; 23: 823-5. 15. Perez-Cerda C, García-Villoria J, Ofman R. 2-Methyl-3hydroxybutyryl-CoA dehydrogenase (MHBD) deficiency: an Xlinked inborn error of isoleucine metabolism that may mimic a mitochondrial disease. Pediatr Res 2006; 59:162. 16. Ensenauer R, Niederhoff H, Ruiter JP, Wanders RJ, Schwab KO, Brandis M, et al. Clinical variability in 3-hydroxy-2- Journal of the College of Physicians and Surgeons Pakistan 2016, Vol. 26 (6): 498-502 501 Huma Arshad Cheema, Hassan Suleman Malik, Arit Parkash and Zafar Fayyaz methylbutyryl-CoA dehydrogenase deficiency. Ann Neurol 2002; 51:656-9. 17. Gibson KM, Breuer J, Kaiser K, Nyhan WL, McCoy EE, Ferreira P, et al. 3-Hydroxy-3-methylglutaryl co-enzyme A lyase deficiency: report of five new patients. JInher Metab Dis 1988a; 11:76-87. 18. Gibson KM, Breuer J, Nyhan WL. 3-Hydroxy-3-methylglutaryl co-enzyme A lyase deficiency: review of 18 reported patients. Eur J Pediatr 1988a; 148:180-6. 19. Sperandeo MP, Andria G, Sebastio G. Lysinuric protein intolerance: Update and extended mutation analysis of the SLC7A7 gene. Hum Mutat 2008; 29:14-21. 502 20. Van Karnebeek CDM, Stockler S. Treatable inborn errors of metabolism causing intellectual disability: A systematic literature review. Mol Genet Metab 2012; 105:368-81. 21. Fang-Hoffmann J, Lindner M, Shahbek N, Baric I, Al Thani GF, Hoffmann G. Metabolic medicine: new developments in diagnosis and treatment of inborn errors of metabolism. World J Pediatr 2006; 3:169-76. 22. Mak CM, Lee HH, Chan AY, Lam CW. Inborn errors of metabolism and expanded newborn screening: review and update. Crit Rev Clin Lab Sci 2013; 50:142-62. 23. Schwartz IV, Souza CFM, Giugliani R. Treatment of inborn errors of metabolism. J Pediatr Rio J 2008; 84:S8-19. Journal of the College of Physicians and Surgeons Pakistan 2016, Vol. 26 (6): 498-502