Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
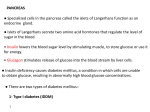
Regulation of blood glucose Endocrine regulation of blood glucose -The normal blood glucose level ranges between 80-120 mg/100 ml blood. -This level is controlled by the following hormones: 1- Pancreatic h. 2- Adrenaline. 3- Glucocorticoids. 4-Thyroxine. 5-Growth h. Importance of blood glucose regulation: !!! • Glucose is the only nutrient that normally can be used by the brain and retina. • Glucose is important source of energy for the cells. a) Pancreatic hormones -The endocrine cells of the pancreas are present in discrete groups called ‘islets of Langerhan’s’, which are more numerous in the tail than in the body and comprise 1-2% of its weight. Four groups of cells are now identified in the islets: 1.Alpha cells,( 25% of islet mass) glucagon h. 2.Beta cells,(about 60%), located in the centre of the islet. insulin h. 3.Delta or D cells, (10% of the islet mass) somatostatin h. 4.F cells, (only polypeptide h. about 5%) pancreatic I. Insulin 1-Insulin blood glucose level by: a. Glycogenesis b. Inhibition of glycogenolysis c. glucose uptake by the tissues d-gluconeogenesis 5. transformation of glucose into fat. 2-Anabolic action Insulin is an essential hormone for growth: a)In muscle, insulin stimulates the uptake of certain amino acids across the cell membrane. b)Insulin also stimulates the rate of protein synthesis. c) Anti-catabolic effects i.e. it inhibits proteolysis. 2.Insulin increases cellular uptake of potassium, phosphate and magnesium. 3.It increases the reabsorption of phosphate and sodium by renal tubules potassium, Regulation of secretion -The major regulation is the plasma glucose level (no insulin when glucose < 50 mg%). -A half maximum insulin secretion occurs at a plasma glucose level of about 150 mg% and a maximum response at 300 to 500 mg%. - GIP (glucose dependent peptide), gastrin, secretin, pancreatic glucagons insulinotropic Cholecystokinin, - Oral protein, Triglycerides and fatty acids II. Glucagon -Glucagon is a hyperglycemic polypeptide from α cells. 1.glucose:glycogenolysis andgluconeogenesis 2.lipolysis and hepatic cholesterol synthesis. 4.Natriuresis, by renal tubular Na+ reabsorption 5. myocardial contractility COP. 6.A local CNS h. for regulation of appetite. 1. Glucagon release is stimulated by: a) Hypoglycaemia 2-4 fold in glucagon level. b) Protein meal c) FFA. d) Exercise. e)Vagal stimulation or administration of acetylcholine. f)Stress, including infection, toxaemia, burns and major surgery. g) Growth hormone. 2. Glucagon release is inhibited by a)Hyperglycaemia: 50%. b) FFA. c) Somatostatin. glucagon level by B) Other hormones which regulate blood glucose level 1.Adrenaline: -glycogenolytic on liver and muscles. 2.Glucocorticoids: I- gluconeogenesis. II- glucose uptake by the tissues. 3.Growth hormone: - glucagon hormone. -Inhibits glucose uptake by tissues. 4.Thyroxin: - glucose absorption from intestine. - glycogenolysis. The net result is a rise in blood glucose level. Danger of increased blood glucose: (Diabetes Mellitus) • 2 forms of diabetes mellitus: –Type I: insulin dependent diabetes (IDDM). –Type II: non-insulin dependent diabetes (NIDDM). Diabetes Mellitus Diabetes mellitus It results from deficiency of insulin action , which leads to: 1.Hyperglycaemia: - due to absence of effects of insulin. 2.Glucosuria: i.e loss of glucose in urine. - when the blood glucose level becomes > renal threshold (180 mg%). 3.Polyuria due to: a)Excretion of glucose in urine. b) osmotic pressure of the blood drags water out of the cells towards the blood. -This causes dehydration of the tissue cells. 4.Polydepsia:intense thirst due to dehydration. 5. Acidosis: - Due to inhibition of carbohydrate metabolism. -The body depends on the fat metabolism which supplies most of the energy needed. -Uncontrolled diabetes accumulation of acetoacetic acid and beta hydroxybuteric acid acidosis. 6.Loss of weight and asthenia: -Due to mobilization of fat and proteins for supply of energy. 7. cholesterol and TG in blood: - early development of arteriosclerosis. Pituitary gland (hypophysis cerebri) -The pituitary gland is an ovoid structure weighing between 500 and 600 mg in an adult. -It is located at the base of the brain in a small cavity called 'pituitary fossa' or 'sella tursica', which is covered by an extension of the dura mater (the diaphragma sellae) through which passes the pituitary stalk connecting the gland to the hypothalamus. Growth hormone Functions of growth hormone 1-On growth: a) It has a powerful protein anabolic effect. b) It increases the length of bones. 2-On metabolism: 1) Protein metabolism. 2) CHO metabolism. 3) Lipid metabolism. Functions of growth hormone 1. On metabolism Protein metabolism Growth hormone stimulates protein synthesis by: i- AA transport through the cell membranes. ii- Increase of protein synthesis by ribosomes. iii- Increase formation of RNA. iv- Inhibition of protein catabolism. Functions of growth hormone 2- On metabolism CHO metabolism anti-insulin action: - It inhibits the hexokinase enzyme and so decreases glucose uptake by tissues. - It stimulates gluconeogenesis in the liver with more production of glucose. - It stimulates the release of glucagon hormone Functions of growth hormone 3- On metabolism lipid metabolism -It has powerful lipolytic effect thus increasing the blood level of FFA which provides energy during stress conditions particularly hypoglycaemia and starvation. Mechanism of growth hormone action: -Its growth promoting actions are mediated by a group of polypeptides called somatomedins that formed in the liver, in bone cells -They are structurally similar to proinsulin. They are, called insulin-like growth factors (IGF), of which 2 types have been identified: IGF-I and IGF-II. Control of G.H. secretion I. Hypothalamus 1.GH releasing factor which increases GH secretion. 2.GH release inhibiting factor or somatostatin which suppresses GH secretion. Physiology of growth -Body growth is a continuing process throughout childhood and adolescence. -It is exceedingly rapid in the first 2 years of life -Later there is a second phase of rapid growth in relation to puberty followed by cessation of growth when the adult height is reached. Peaks of growth Factors affecting growth 1. Hormones. 2. Extrinsic factors. 3. Genetic factors. 4. Growth-regulating peptides. Factors affecting growth 1-Hormones a)Growth hormone promotes growth in infancy. b) Thyroid hormones stimulate the process of physical, mental and sexual growth growth probably by a permissive action for somatomedins. c) Insulin is important for the formation of somatomedins. d) Androgens, and oestrogen, are responsible for second spurt of growth at puberty because of their strong anabolic effect 2. Extrinsic factors: -Balanced diet which is particularly rich in proteins and essential vitamins is important for a normal growth process particularly in children. -Exposure to stress as infections in children leads to suppression of growth. -This is followed in the recovery period, by a stage of enhanced growth rate called “catchup period”. 3. Genetic factors: -which determine: - Growth rate. - Age of puberty. - Adult height. 4. Growth-regulating peptides: I-Fibroplast growth factors. II-epidermal growth factors III-Growth promoting and growth inhibiting peptides. Disorders of adenohypophysis Disorders of GH Secretion Before union of epihhysis Gigantism After union of epihhysis Acromegaly Secretion In children In adults Dwarfism Muscle mass Broad forehead Prognathism Functions of prolactin 1.Development of breast tissue: a) During prepubertal and postpubertal: - Proliferation and branching of milk ducts. b) During pregnancy, prolactin: - development of milk alveoli. c) After parturition: -milk synthesis and secretion. 2.In women, high levels of prolactin appear to block the synthesis and release of LHRH preventing ovulation. -This accounts for the absence of menstruation (amenorrhea) during postpartum lactation. Osmoreceptors Supraoptic n. Of hypothalamus ADH 320 310 300 290 m.osm/l Osmotic control of ADH Blood vessel H2O reabsorption 2-Vasoconstriction (vasopressin) 2.When administered systemically in large doses, ADH causes contraction of the smooth muscles particularly in the blood vessels intense splanchnic vasoconstriction. -Used therapeutically in controlling persistant, serious gastrointestinal bleeding. Disorders of ADH secretion Diabetes insipidus (D.I): A clinical condition caused by ADH actions. Types and causes: 1) Central D.I: -due to deficiency of ADH release from the hypothalamus. 2) Nephrogenic D.I: -due to inability of the kidney to respond to ADH due to receptor defect. a)Polyuria:The volume of urine increased (may reach 25 liters/day) b)Polydepsia is markedly PRIH Oxytocin 1. Milk-letting effect Prolactin Oxytocin Milk secretion and ejection Suckling reflex 2. Powerful contraction in the uterus -Powerful contracting action on the uterus, -This effect is potentiated by oestrogen and inhibited by progesterone. Thyroid Gland Found at the base of the throat Consists of two lobes and a connecting isthmus Produces two hormones Thyroid hormone Calcitonin Thyroid Hormone Major metabolic hormone: increase lipolysis, blood glucose level, increase metabolic rate Composed of two active iodinecontaining hormones Thyroxine (T4) – secreted by thyroid follicles Triiodothyronine (T3) – conversion of T4 at target tissues Adrenal Glands Two glands Cortex – outer glandular region in three layers Medulla – inner neural tissue region Sits on top of the kidneys Hormones of the Adrenal Cortex Mineralocorticoids (mainly aldosterone) Produced in outer adrenal cortex Regulate mineral content in blood, water, and electrolyte balance Target organ is the kidney Stimulate Na and water reabsorption. Hormones of the Adrenal Cortex Glucocorticoids (including cortisone and cortisol) Produced in the middle layer of the adrenal cortex Promote normal cell metabolism Help resist long-term stressors Released in response to increased blood levels of ACTH Hormones of the Adrenal Cortex Sex hormones Produced in the inner layer of the adrenal cortex Androgens (male) and some estrogen (female) Hormones of the Adrenal Medulla Produces two similar hormones (catecholamines) Epinephrine Norepinephrine These hormones prepare the body to deal with short-term stress