Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
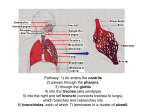
Pulmonary Ventilation and Pulmonary Circulation Chapter 27 Mechanics of Pulmonary Ventilation • The lungs can be expanded and contracted in 2 ways: – 1. Downward and upward movement of diaphragm – 2. Elevation and depression of ribs Lung movements Pressures that cause movement of air in/out of lungs • lung floats in the thoracic cavity • surrounded by thin layer of pleural fluid – lubricates Pleural pressure • Pressure of fluid in narrow space between lung pleura and chest wall pleura – slight suction of excess fluid into lymphatic channels produces negative pressure – keeps lungs in place Alveolar Pressure • Pressure inside lung alveoli • no air flowing in or out of lungs = atmospheric pressure • inspiration- alveoli pressure slightly below atm. pressure (-1) • expiration- alveoli pressure slightly above atm. pressure (+1) Compliance of the lungs • Compliance- extent to which lungs expand for each unit increase in transpulmonary pressure (pleural press. alveolar press.) • Compliance diagram-inspiratory compliance curve and expiratory compliance curve Compliance Diagram • Characteristics determined by: – elastic forces of lung tissue – elastic forces caused by surface tension of fluid that lines the inside walls of alveoli Elastic forces of lung tissue • Determined by the elastin and collagen fibers interwoven among lung parenchyma – deflated lungs- contracted and kinked – expanded lungs- stretched and unkinked (elongating) • Elastic forces caused by surface tension – “surfactant” “Surfactant”, surface tension and collapse of lungs • Inner surfaces of alveoli- water surface attempting to contract – forces air out of alveoli – net effect- causes elastic contractile force of entire lungs- “surface tension elastic force” • “Surfactant”- spreads over surface of a fluid and greatly reduces the surface tension – secreted by special epithelial cells in alveoli – reduces amt. of press. to keep lungs expanded The “work” of breathing • • • • 1. Compliance work/elastic work 2. Tissue resistance work 3. Airway resistance work Normal quiet respiration- only 3 to 5% of total work energy expended by body is for pulmonary ventilation process • heavy exercise- 50x increase • • • • • • • • 1. 2. 3. 4. 1. 2. 3. 4. Pulmonary Volumes Tidal volume Inspiratory reserve volume Expiratory reserve volume Residual volume Pulmonary capacities Inspiratory capacity Functional residual capacity Vital capacity Total lung capacity Alveolar ventilation • Rate at which new air reaches gas exchange areas of the lungs where the air is in close proximity to the pulmonary blood • new air moves from terminal bronchioles into the alveoli by diffusion The respiratory passages Rate of alveolar ventilation • VA= Freq x (VT-VD) – – – – VA- vol. of new air entering the alveoli/min freq.- no. of respirations /min. VT- tidal volume VD- dead space volume Functions of the Respiratory Passageways • Trachea- multiple cartilage rings- keeps trachea from collapsing • Bronchi- less extensive cartilage plates • Bronchi and bronchioles- walls of smooth muscle – terminal bronchioles (respiratory bronchioles)- only a few smooth muscle fibers – Sympathetic control weak- few nerve fibers there – however, norepinephrine and epinephrine cause dilation of bronchial tree – parasympathetic- Ach- mild to moderate constriction – other constriction factors: histamine, slow-reacting substance of anaphylaxis Mucus layer • Moistens respiratory passages • Secreted in part by goblet cells in epithelial lining – also traps small particles • Cough reflex- removes foreign particles – sometimes velocities as high as 75-100 mph Respiratory function of the nose • 1. Warm air • 2. Humidify air • 3. Filter air – together called air conditioning function of upper respiratory passageways Vocalization • 2 mechanized functions: – 1. Phonation- larynx- vocal cords – 2. Articulation- structures of mouth The pulmonary blood circulation • Pulmonary vessels – larger diameters than systemic arteries – very thin and distensible- large compliance-accomodates 2/3 of stroke volume output of right ventricle – lymphatics – prevent edema- remove particulate matter and leaking plasma protein Blood flow through lungs and its distribution • Lung blood flow essentially equal to cardiac output – factors controlling cardiac output also control pulmonary blood flow • blood distributed to best oxygenated alveoli – when concentration of O2 in alveoli falls below normal, vessels constrict- sends blood to areas of lungs that are better aerated • Hydrostatic pressure gradients and regional pulmonary blood flow • Pulmonary capillary dynamics • Pulmonary edema Pulmonary capillary dynamics • So many capillaries in alveolar walls that they almost touch each other • capillaries different than other capillaries – – – – 1.Cap. pressure very low-7mm vs. 17mm Hg 2 Interstitial fluid press. slightly more negative 3 Relatively leaky to protein molecules 4.Alveolar wall very thin- allows dumping of fluid fr. Interstitial spaces into alveoli • The net filtration pressure at capillary membrane causes a slight continual flow of fluid from pulmonary cap.’s- pumped back into circulation through lymphatic system • Slight negative pressure in interstitial spaces that sucks any fluid from alveoli to lymphatics – keeps alveoli “dry” except for sm. amt that moistens lining surfaces of alveoli Pulmonary edema • Most common causes: – 1.left heart failure or disease of mitral valve • inc. cap. press-floods interstitial spaces and alveoli – 2.damage to pulmonary cap. Membranes • pneumonia • breathing noxious substances (chlorine gas, sulfur dioxide gas) • Edema occurs when capillary pressure rises from negative range into positive range – death can occur within hours – acute left heart failure- capillary pressure rises as high as 50mm Hg-death within 1/2 hour The fluids in the pleural cavity • Very thin layer of mucoid fluid between parietal and visceral pleurae – allows lungs to slide back and forth within cavity during breathing • negative force on outside of lungs- keeps them expanded – neg. press. created by pumping of fluid from pleural space by lymphatics The interpleural spaces