Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
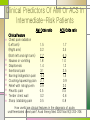
Treatment of patients with suspected UA/NSTEMI 2005년 8월 22일 응급의학과 R3 제상모 Definitions ACS UA Occurring for the first time Accelerating angina, rest angina NSTEMI Clinical syndrome of acute myocardial ischemia UA/NSTEMI/STEMI Elevation in biochemical markers STEMI(ST-segment elevation MI) Diagnostic ST elevation on ECG testing Pathopysiology Epidemiology 5-7% of total ED volume in US 6 million patients visit ED per year 70% prove not to have ACS 3 million patients are hospitalized 0.8 million patients are MI 1.5 million patients are UA/NSTEMI Chest pain Be expert! Both in diagnosis and recommended management. 0.4-4% of MI are sent home Some cases UA/NSTEMI carry a worse prognosis than STEMI UA/NSTEMI UA/NSTEMI CCU ED evaluation Risk stratification Historical and physical features ECG Cardiac biomarkers History Typical angina Risk factors Deep, poorly localized chest or arm discomfort Exertional and relieved with rest or nitrates Known coronary stenosis greater than 50% >65 years and male gender Remember atypical complaints! Missed MI are associated <66 years, female gender, non white race, normal or nondiagnostic ECGs, diabetes Physical Examination Limited value to rule out ACS Focus on ACS-related complaints Left ventricular failure Valvular abnormalities Cardiogenic shock Clinical Predictors Of AMI Or ACS In Intermediate-Risk Patients AMI Odds ratio Clinical feature Chest pain radiation (Left arm) (Right arm) (Both left and right arm) Nausea or vomiting Diaphoresis Exertional pain Burning/indigestion pain Crushing/squeezing pain Relief with nitroglycerin Pleuritic pain Tender chest wall Sharp /stabbing pain 1.5 3.2 7.7 1.8 1.4 3.1 4.0 2.1 0.9 0.5 0.2 0.5 ACS Odds ratio 1.7 2.5 6.0 1.0 1.2 2.5 1.5 0.9 2.0 0.5 0.6 0.8 How useful are clinical features in the diagnosis of acute, undifferentiated chest pain? Acad Emerg Med 2002 Mar;9(3):203-208. Electrocardiogram Predictive findings Reversible ST-segment depression in UA Symmetric T-wave inversions greater than 0.2mV in the precordial leads(V1 through V4 ) is highly specific for stenosis of the LAD coronary artery Less predictive findings ST-segment depression less than 0.05mV T-wave inversion of less than 0.2mV Existing Q waves Continuous Multi-Lead ST-segment Monitoring Useful in episodes of silent ischemia Over 24 hours, silent ischemic episodes were found 27% of patients with UA At 30 days, death and MI occurred in 5.7% of those without episodes and 19.7% of with five of more episodes The ACEP clinical policy on chest pain also supports this technology Chest X ray Most useful in eliminating alternating diagnosis Routine Laboratiory Studies Complete blood count Renal fx For drug dose reduction Serum electrolytes For r/o underlying anemia For r/o arrythmogenic abilities Coagulation studies Become less necessary Biochemical Markers Timing of the rise Elevation Return to baseline Myoglobin within 2-4 hours rapidly Troponins about 6 hours one week CK-MB about 6 hours 2 days Large trials found great sensitivity and specificity of troponins. Zimmerman J, Fromm R, Meyer D, et al. Circulation 1999 (Prospective, multicenter; 955 patients) Biochemical Markers Single isolated troponin measurement Current recommendations from ACEP Sensitivities of 37-49% Specipicities of 87%-97% Measure a first troponin on arrival Repeat level at least eight hours after continuous symptom onset. Elevation fo TnT level was independently predictive of risk across the entire spectrum of renal fuction Biochemical Markers Bed side cardiac markers Normal ECG Those with positive troponin can be consulted to cardiology minutes after arrival Accuracy is comparable to standard laboratory assays CK-MB performs less well than the cardiac troponins in terms of both sensitivity and specificity Myoglobin has very high early sensitivity. CRP elevation in UA/NSTEMI may indicate the presence of multiple unstable plaques. BNP is a relaiable predictor of death with ACS Risk Scores 7 variables that predicted increasing risk for mortality (TIMI score) Age greater than 65 years Presence of at least three risk factors for CAD Prior coronary stenosis of greater than 50% Use of aspirin within the previous seven days Presence of ST-segment deviation on admission ECG At least two anginal episodes in the prior 24 hours Elevated serum cardiac biomarkers Risk stratification High Likelihood Signs & Symptoms History : Chest or left arm discomfort as chief complaint reproducing prior documented angina; known history of CAD, including MI Examination : Transient MR, hypotension, pulmonary edema or rales ECG : New ST deviation (> 0.05 mV) or T-wave inversion (> 0.2 mV) with symptoms Biochemical markers : Elevated troponin or CK-MB American College of Cardiology/American Heart Association Task Force on Practice Guidelines Risk stratification Intermediate Likelihood History : Chest or left arm pain or discomfort as chief symptom; age > 70 years; male sex; diabetes mellitus Examination : Peripheral vascular disease ECG : Fixed Q waves; abnormal ST segments not documented to be new T-wave flattening or inversion with dominant R waves; Biochemical markers : Normal Risk stratification Low Likelihood History : Probable ischemic symptoms in absence of any of the intermediate likelihood characteristics; recent cocaine use Examination : Chest discomfort reproduced by palpation ECG : normal ECG Biochemical markers : Normal Ed treatment Risk-Based Treatment Anti-ischemic agents Antiplatelet agents Antithrombotic agents Common Anti-Anginal Therapies Oxygen Optimize oxygenation in those with or at risk for hypoxemia As needed to keep SaO2 > 90% Bed rest with continuous ECG monitoring Prevent and detect ischemia/arrhythmias Bed rest until serum biomarkers negative Nitrates Coronary dilation, pre- and after-load reduction 0.4 mg SL q 5 min x3, consider infusion titrated to relieve symptoms Beta-blockers Decreased myocardial oxygen consumption e.g., metoprolol 5 mg IV q 5 min x3, then 12.5-25.0 mg PO BID Common Anti-Anginal Therapies Morphine ACE inhibitors Analgesia, venodilation, decreased heart rate and blood pressure 1-5 mg IV Afterload reduction in those with CHF, possible myocardial remodeling benefit Many possible agents; initiate within 24 hours of MI Calcium-channel blockers Decreased myocardial oxygen consumption Diltiazem 240 mg PO or 10-15 mg IV followed by infusion Antiplatelet Therapy Aspirin Antagonists of platelet ADP receptor Initial dose 160-325 mg PO nonenteric, then 75-160 mg PO qd Clopidogrel (Plavix) Ticlopidine (Ticlid), for aspirin intolerant Glycoprotein IIb/IIIa inhibitors Eptifibatide (Integrilin) Abciximab (ReoPro) Tirofiban (Aggrastat) For high-risk patients who have not PCI planned! Antithrombotics Unfractionated heparin Bolus 60-70 U/kg (max, 5000 U), then 12-15 U/kg/min IV infusion; goal aPTT 1.5-2.5x control Fractionated heparin Enoxaparin (Lovenox) 1 mg/kg SC q 12 hours Early invasive vs. Early conservarive Treatment An early trial, VANQWISH RITA3 trial Randomized 920 patients with NSTEMI At one year, 58 deaths in the invasive group, 36 death in the conservartive group Randomized 1810 patients with NSETMI Rates of death or MI were nonsignificantly different An early invasive strategy has been recommended in patients with UA/NSTEMI without serious co-morbidity who have high risk features. Thrombolysis Don’t do it! Increse the risk of MI in UA/NSTEMI Expose patients to significant cost and bleeding resk Only to patients with STEMI who meet standard AHA inclusion criteria Disposition Disposition Noncardiac causes Chronic stable angina Appropriate treatment Exit Definite ACS Stable patients with UA/NSTEMI who have recurrent symptom, and/or ST segment deviations, or elevated cardiac markers should be admitted Hemodynamic instability or recurrent ischemic pain warrant addmision to CCU Disposition Possible ACS High risk group Hospitalization Moderate risk group Repeat ECG and biomarkers Noninvasive stress testing before discharge or shortly thereafter Low risk group Immediate ED stress testing Repeat ECG and biomarkers Noninvasive stress testing before discharge or shortly thereafter Chest pain observation units ED-based chest pain evaluation centers Become common Strict protocol to rapidly rule out cardiac ischemia Reduce hospital charges over 60%(500-1500$ per patient) Decrease time in the hospital by 10-40 hours per patient Reduce the rates of missed AMI from 4% to 0.4% Chest pain center 가 없으면? Consider outpatient provocative testing rather than admission Hamm et al. NEJM. 773 patients who had acute chest pain for less than 12hours without ST segment elevation Bed side measurement of TnT and TnI Another sample taken at least six hours after the onset of pain Only 1 with negative TnT had a cardiac event within two weeks after discharge EM physician can safely discharge patients home for urgent outpatient stress testing by using ECG and troponin level at least six hours after pain Chest pain observation units Erlanger chest pain evaluating protocol Erlanger medical center, University of Tenessee College of Medicine 1-year period, from Jan to Dec 1999 2,074 patients with chest pain Serial ECG monitor, 2-hour serum marker, selective nuclear stress testing 179 patients with AMI, 26 patients with recent AMI(decreasing curve of CKMB) 327 patients with with 30-day ACS Provocative Testing Graded Exercise Testing Simplest and least expensive form Sensitivity are low as 70% Normal test has a strong negative predictive value Eligible patient Symptom-free Normal ECG Be able to either walk on a treadmill or ride a bicycle to achieve 70-85% predicted maximal heart rate(220-age) Provocative Testing Immediate stress testing in the ED Kirk et al. Time- and cost-effective 212 low-risk patients, without evaluation biomarker None of the patients discharged from the ED had mortality at 30-day follow-up Amsterdam et al. 1000 low-risk patients with no evidence of hemodynamic instability, arrhythmias, or ECG signs of ischemia They found that immediate exercise testing are safe and accurate Provocative Testing Stress echocardiography For patients with poor exercise tolerance Dobutamine chemically drive the heart rate Inducible wall motion abnormalities are hall marker of critical CAD Sensitivities over 85% for normal or non-diagnostinc ECGs Low-risk patients with negative stress echocardiogram have a less than 1% rate for AMI and cardiac death in the subsequent year Limitation Cost, Operator dependence Provocative Testing Myocardial perfusion imaging Sensitivities for ACS greater than 90% Quantify infarct size Predict the need for revascularization Drawback After injection, patients must to be moved to a radioisotope-approved area Cost. $1000-$1600 per study Reference Evidence-Based Risk Stratification Of Patients With Suspected UA/NSTEMI, Emergency medicine practice, April 2004. Chest Pain: Diagnostic Strategies To Save Lives, Time, And Money In The ED, Emergency medicine practice, June 2003. ACLS for experienced providers, AHA, 2003. Marx: Rosen's Emergency Medicine: Concepts and Clinical Practice, 5th ed