Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
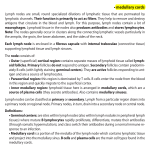
MR evaluation of normal pelvic and inguinal lymph nodes Poster No.: C-1979 Congress: ECR 2011 Type: Scientific Exhibit Authors: M. RAMIREZ-BAILLOEUIL, J.-P. Tasu; Poitiers/FR Keywords: Pelvis, MR, Imaging sequences, Metastases, Neoplasia DOI: 10.1594/ecr2011/C-1979 Any information contained in this pdf file is automatically generated from digital material submitted to EPOS by third parties in the form of scientific presentations. References to any names, marks, products, or services of third parties or hypertext links to thirdparty sites or information are provided solely as a convenience to you and do not in any way constitute or imply ECR's endorsement, sponsorship or recommendation of the third party, information, product or service. ECR is not responsible for the content of these pages and does not make any representations regarding the content or accuracy of material in this file. As per copyright regulations, any unauthorised use of the material or parts thereof as well as commercial reproduction or multiple distribution by any traditional or electronically based reproduction/publication method ist strictly prohibited. You agree to defend, indemnify, and hold ECR harmless from and against any and all claims, damages, costs, and expenses, including attorneys' fees, arising from or related to your use of these pages. Please note: Links to movies, ppt slideshows and any other multimedia files are not available in the pdf version of presentations. www.myESR.org Page 1 of 14 Purpose To estimate pelvic, mesorectal and inguinal lymph nodes (LN) normal size and to determine superior thresholds in order to differenciate benign versus malignant LN with conventional MR cross-sectional imaging. In pelvic malignancies, metastatic lymphatic spread conditions patient's prognostic. The most important criterion for LN involvement in cross-sectional imaging is still enlargement. Very few studies are about pelvic and inguinal LN normal size with MRI. # Superior thresholds used in routine for short axis are: › 8 to 10 mm for pelvic and inguinal nodes › 3 to 5 mm for mesorectal nodes Methods and Materials Patient population: Thirty six healthy volunteers aged 20 to 33 year old were included after informed consent. People who had absolute or relative MRI contraindication (included pregnancy), pelvic malignancy history, or infectious or inflammatory symptoms during the six last months were excluded from the study. MRI: Acquisitions were performed on a 1.5 Tesla superconductive magnet (Philips Intera, Nederland) using a sense body phased array coil. Images were obtained in the strict axial plane using a steady state gradient echo (balanced-FFE) sequence. Parameters were as follows: TR 5,3 ms, TE 2,7 ms, #=90°, 3 mm thick contiguous slices, matrix 512x512. Slices covered the anatomic region from aorto-iliac fork to the pubic symphysis. Imaging were read on post-treatment console Adavantage Window (General Electric). Imaging was performed without enhancement. Page 2 of 14 Each lymph node was measured in the maximal short and long axis in a perpendicular way, in order to realise tenth millimeters measures. Anatomy: Each lymph node was caracterized by laterality (right, left, median), size and anatomic territory, following vascular axis. Eight territory were defined: inguinal, external iliac, internal iliac, common iliac, obturator, mesorectum, presacral and around bladder, and described as: - Inguinal: into the Scarpa area. Upper limit inguinal ligament; lateral limit medial side of Sartorius muscle; medial limit lateral side of long adductor; anterior limit is the groin superficial fascia and posterior limit is ilio-psoas and pectine muscle. - External iliac: between common iliac fork and inguinal ligament. Posterior limit is the pelvic part of ureter and anterior limit is the femoral septum. - Internal iliac: along internal iliac artery and its visceral and parietal division. Anterior limit is the pelvic part of ureter, posterior limit is sacro-iliac joint, upper limit is iliac fork and inferior limit is levator ani muscle. - Common iliac: along common iliac artery between aortic and iliac forks. - Obturator: along obturator axis that is anterior division of internal iliac vessels, near obturator canal. - Mesorectum: fatty tissue around rectum limited by the fascia recti. - Presacral: anterior limit is the posterior fascia recti, posterior limit is the anterior part of the sacrum. - Around bladder: fatty tissue around bladder. Lymph nodes were described as oval or round images, with intermediate signal surrounded by a low signal piping. Lymph nodes were different from vascular or nervous structures that are like tubes followed on several contiguous slices. Statistical method: Size of maximal long and short axis diameter of each lymph node was analysed and their distribution was represented on graph with a histogram (empiric distribution) superimposed on a curve (theoretical distribution) Skewness and kurtosis were estimated and adequacy to normal distribution was evaluated by Shapiro-Wilk normality test. Page 3 of 14 In order to normalize data, a logarithmic transformation was performed. In a second time, patient variation sources like age or gender, and lymph node characteristics variation sources like laterality or anatomic territory were analysed by mixed models variance-covariance analysis for repeated datas. Use of mixed models is here necessary because of non-independence of collected datas for the same person and imbalance number of analysed lymph nodes. Only statistically significant variables on lymph nodes size were kept (p<0.05, F test). Transformed data variance homogeneity (or homoscedasticity) was a condition for analysis validity. Levene's test of variance comparison was applied. Considering the heterogeneity of variances and means between territories, a superior th threshold was proposed in each anatomic territory, corresponding to the 95 percentile of normal distribution. Superior thresholds were calculated first in transformed scale (logarithmic unit) then the opposite transformation was performed to obtain millimetric scale. Lim log= m+ z 95% S Lim log = superior threshold (logarithmic scale) m = arithmetical mean in logarithmic scale S = standard deviation z95% = 1,645 Images for this section: Page 4 of 14 Page 5 of 14 Fig. 1: Pelvic and inguinal lymph nodes anatomic territories Fig. 2: Balanced-FFE gradient echo axial sequence, showing natural contrast between liquids like bladder or vessels (high signal) and other tissues (intermediate or low signal) Page 6 of 14 Fig. 3: Mesorectal lymph node Fig. 4: Deep inguinal lymph node maximal short and long axis diameters Page 7 of 14 Results A total of 1147 lymph nodes were identified: 678 inguinal, 159 external iliac, 131 internal iliac, 69 common iliac, 92 in mesorectal territory, 9 presacral, 7 obturator and 2 arround bladder. Distribution of short and long axis values was represented by two different assymetrical curves before logarithmic transformation (figure 1). A normal distribution was obtained after logarithmic transformation (Gauss curve) (figure 2). A minimum of 14 and a maximum of 46 lymph nodes were measured by person on imaging of 36 volunteers, 22 women and 14 men, aged from 20 to 33 years old (mean age 24,6). Statistical study (Levene test, F test) of different parameters showed that age, gender and laterality had no significant influence whereas anatomic territory had a meaningful influence on size (p<0,05 ; F test). Presacal, obturator and around bladder territories were insufficiently represented to be included in the study. Statistic analysis showed a mean size and a upper size respectively of 2,6 and 3,9 mm; 3,3 and 4,8 mm; 2,6 and 2,9mm for short axis and 3,7 and 5,3 mm; 5,8 and 9,8 mm; 6,5 and 8,3 mm for long axis diameter. These lymph nodes were excluded of the study. A total of 1129 lymph nodes was included, and the only effect retained was the anatomic territory. Superior thresholds and mean values are reported on figures 3 and 4 in logarithmic scale and after reverse transformation in millimetric scale. Images for this section: Page 8 of 14 Fig. 1: Assymetrical curve before logarithmic transformation. Example for maximal short axis diameters. On the abscissa:size of nodes (mm); on the ordinate:number of nodes (percent) Page 9 of 14 Fig. 2: Gauss curve after logarithmic transformation. Example for maximal short axis diameters.On the abscissa:size of nodes (mm); on the ordinate:number of nodes (percent) Page 10 of 14 Fig. 3: Values for short axis diameter; g= arithmetic mean in logarithmic scale Slog= standard deviation in logarithmic scale mm= millimeter Fig. 4: Values for long axis diameters; g= arithmetic mean in logarithmic scale Slog= standard deviation in logarithmic scale mm= millimeter Page 11 of 14 Conclusion Maximal short axis diameter is more reproductible than long axis whatever the plane section and is a criterion for evaluation of LN involvement (RECIST: response evaluation criteria in solid tumours 2009). Age, gender and laterality have no influence on size. Only anatomic territory has a significant influence on size. We decided to round up short axis superior thresholds values (95 nearest millimeter to improve reproductibility between observers: External iliac 5,3 6 Internal iliac 4,4 5 Common iliac 5,3 6 Mesorectal 3,9 4 th percentile) to the Inguinal 6,3 7 Superior thresholds (millimeter) before and after rounding These values are shorter than those used in routine by radiologists and their application could improve metastatic LN detection. Steady state gradient echo sequence (balanced-FFE) with axial thin slices can be used to detect pelvic, mesorectal and inguinal lymph nodes. References [1] McMahon CJ, Rofsky NM, Pedrosa I. Lymphatic metastases from pelvic tumors: anatomic classification, characterization, and staging. Radiology, 2010 Jan;254(1):31-46. [2] Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009 Jan;45(2):228-47. Page 12 of 14 [3] Vinnicombe SJ, Norman AR, Nicolson V, Husband JE. Normal pelvic lymph nodes: evaluation with CT after bipedal lymphangiography. Radiology. 1995 Feb;194(2):349-55. [4] Grubnic S, Vinnicombe SJ, Norman AR, Husband JE. MR evaluation of normal retroperitoneal and pelvic lymph nodes. Clinical radiology. 2002 Mar;57(3):193-200; discussion 1-4. [5] Kamina P, Demondon, X, Richer, JP, Scépi, M, Faure, JP. Anatomie clinique de l'appareil génital féminin. Encyclopédie Médico-Chirurgicale: Elsevier Masson 2003. [6] Brown G, Richards CJ, Bourne MW, Newcombe RG, Radcliffe AG, Dallimore NS, et al. Morphologic predictors of lymph node status in rectal cancer with use of high-spatial-resolution MR imaging with histopathologic comparison. Radiology. 2003 May;227(2):371-7. [7] Grey AC, Carrington BM, Hulse PA, Swindell R, Yates W. Magnetic resonance appearance of normal inguinal nodes. Clinical radiology. 2000 Feb;55(2):124-30. [8] Matsuoka H, Masaki T, Kobayashi T, Sato K, Sugiyama M, Atomi Y, et al. Morphological criteria for metastatic mesorectal lymph nodes in rectal cancer. Hepatogastroenterology. 2009 Nov-Dec;56(96):1661-4. [9] Perez RO, Pereira DD, Proscurshim I, Gama-Rodrigues J, Rawet V, Sao Juliao GP, et al. Lymph node size in rectal cancer following neoadjuvant chemoradiation--can we rely on radiologic nodal staging after chemoradiation? Diseases of the colon and rectum. 2009 Jul;52(7):1278-84. [10] Oyen RH, Van Poppel HP, Ameye FE, Van de Voorde WA, Baert AL, Baert LV. Lymph node staging of localized prostatic carcinoma with CT and CT-guided fine-needle aspiration biopsy: prospective study of 285 patients. Radiology. 1994 Feb;190(2):315-22. [11] Hilton S, Herr HW, Teitcher JB, Begg CB, Castellino RA. CT detection of retroperitoneal lymph node metastases in patients with clinical stage I testicular nonseminomatous germ cell cancer: assessment of size and distribution criteria. Ajr. 1997 Aug;169(2):521-5. [12] Damin DC, Tolfo GC, Rosito MA, Spiro BL, Kliemann LM. Sentinel lymph node in patients with rectal cancer invading the anal canal. Techniques in coloproctology. 2010 Jun;14(2):133-9. [13] Lengele B, Scalliet P. Anatomical bases for the radiological delineation of lymph node areas. Part III: Pelvis and lower limbs. Radiother Oncol. 2009 Jul;92(1):22-33. [14] Mangan CE, Rubin SC, Rabin DS, Mikuta JJ. Lymph node nomenclature in gynecologic oncology. Gynecologic oncology. 1986 Feb;23(2):222-6. Page 13 of 14 [15]Morisawa N, Koyama T, Togashi K. Metastatic lymph nodes in urogenital cancers: contribution of imaging findings. Abdominal imaging. 2006 Sep-Oct;31(5):620-9. [16] Rouvière H. Anatomie des lymphatiques de l'homme: Masson 1932. [17] Poirier P, Cunéo,B, Delamere, G, ed. The lymphatics: Westminster: Archibald Constable & co. Ltd 1903. Personal Information Page 14 of 14