Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
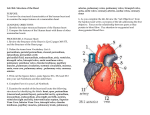
Identifying pericardial recesses on computed tomography : is it important? Poster No.: C-0954 Congress: ECR 2016 Type: Educational Exhibit Authors: S. Thakar , C. B. Kulkarni , S. moorthy , K. P. sreekumar ; 1 1 2 2 2 2 MUMBAI, Maharashtra/IN, kochi/IN Keywords: Cardiac, Anatomy, Lymph nodes, CT, Contrast agent-intravenous, Education, Normal variants, Education and training DOI: 10.1594/ecr2016/C-0954 Any information contained in this pdf file is automatically generated from digital material submitted to EPOS by third parties in the form of scientific presentations. References to any names, marks, products, or services of third parties or hypertext links to thirdparty sites or information are provided solely as a convenience to you and do not in any way constitute or imply ECR's endorsement, sponsorship or recommendation of the third party, information, product or service. ECR is not responsible for the content of these pages and does not make any representations regarding the content or accuracy of material in this file. As per copyright regulations, any unauthorised use of the material or parts thereof as well as commercial reproduction or multiple distribution by any traditional or electronically based reproduction/publication method ist strictly prohibited. You agree to defend, indemnify, and hold ECR harmless from and against any and all claims, damages, costs, and expenses, including attorneys' fees, arising from or related to your use of these pages. Please note: Links to movies, ppt slideshows and any other multimedia files are not available in the pdf version of presentations. www.myESR.org Page 1 of 15 Learning objectives This poster aims • • • • To illustrate the basic anatomy of the pericardial recesses To depict the importance to differentiate it from mediastinal lymphadenopathy To emphasize on points to differentiate between the two To emphasize the impact of pericardial recesses on onco-imagng Background The complex configuration of the pericardial cavity can be described in rather simple words as 'two interconnecting spaces surrounding the heart and the great vessels'. • • • The pericardial cavity has several recesses which can be demonstrated on CT and MR imaging. Accurate knowledge of the cross sectional anatomy of the pericardium and its recesses is essential for the differentiation of fluid filled recesses from various mediastinal lymphnodes. The capability of MDCT to obtain high resolution images results in routine visualization of pericardial recesses, even in absence of abnormal pericardial fluid accumulation. Misinterpretation of the pericardial recess as a mediastinal abnormality or lymphadenopathy or vice versa can have important clinical ramifications especially in onco-imaging. Occasional prominence of one or more recess in comparison to others increases the probability of misinterpretation Findings and procedure details The pericardium encloses the heart and the juxtacardiac parts of great vessels and consists of two components : • • Fibrous (outer) pericardium Serosal (inner) pericardium Fibrous pericardium - A complex collagenous tissue that completely surrounds the heart without being attached to it. Page 2 of 15 - Superiorly : It is continuous with the adventitia of great vessels and with the pretracheal fascia - Inferiorly : It is attached to the central tendon of the diaphragm - Anteriorly : It is attached to the sternum by the superior and the inferior pericardial ligaments and is covered by the parietal mediastinal pleura Serosal pericardium - A single layer of flat cells on a thin subserosal layer of connective tissue - A closed sac with parietal and visceral layer which are continuous with each other - The visceral layer or the epicardium, covers the heart and vessels and is reflected on to the parietal layer which lines the internal surface of the fibrous pericardium - A thin film of pericardial fluid fills up the potential space in between these two layers except at the arterial and the venous attachments where the two merge The reflections of the serosal layer are arranged as two tubes : • • • One encasing the aorta and the pulmonary trunk: The pericardial cavity proper Other encasing the superior and the inferior vena cava and the pulmonary veins : The oblique sinus The passage between the two tubes : The transverse sinus As the pericardium extends along the great vessels, the pericardial cavity proper, transverse and the oblique sinuses form recesses Transverse sinus (TS) - Located posterior to the ascending aorta and the pulmonary trunk and superior to the left atrium Superior aortic recess (SAR) - Transverse sinus extends upwards along the ascending aorta to form the superior aortic recess which is further divided into • • • Posterior portion (P-SAR) Anterior portion (A-SAR) Lateral portion (L-SAR) Page 3 of 15 Posterior portion (P-SAR) - A well defined crescent shaped collection adjacent to the posterior wall of ascending aorta at the level of left pulmonary artery - It is closely related to and thus mimics : • • Pre carinal lymph nodes Sub carinal lymph nodes - It may extend cephalad along the right para tracheal region and thus mimics: • • Paratracheal lymphnode Bronchogenic cyst Anterior portion (A-SAR) - Present anterior to ascending aorta and the pulmonary artery insinuating between them with a characteristic triangular shape. - It may extend superiorly and mimics : • • Aortopulmonary window lymphnode Para aortic lymphnode - It may extend downwards upto the right atrium where it is closely related to the thymus and thus mimics : • Pre vascular lymphnodes Lateral portion (L-SAR) - Insinuates itself between ascending aorta and the SVC - It is closely related to and mimics : • • Para aortic lymph node Pre vascular lymph nodes Inferior aortic recess (IAR) - Transverse sinus extends caudally in between the lateral aspect of the ascending aorta and the inferior SVC or the right atrium to form the inferior aortic recess - It extends inferiorly upto the aortic valve annulus Pulmonic recesses Page 4 of 15 - Transverse sinus extends laterally to form the right and the left pulmonic recesses Right pulmonic recess - Inferior to the right pulmonary artery and superior to the left atrium Left pulmonic recess - Bounded superiorly by left pulmonary artery, inferiorly by the left superior pulmonary vein and medially by the ligament of marshall (vestigial remnant of left SVC) - It is closely related to and mimics • Inferior tracheobronchial lymphnodes Transverse (TS) # Pre carinal lymph nodes # Sub carinal lymph nodes # Paratracheal lymph nodes # Bronchogenic cyst sinus Superior aortic Posterior SAR recess (SAR) (p SAR) # AP window lymph nodes # Para-aortic lymph nodes # Prevascular lymph nodes Anterior SAR (a SAR) Right lateral SAR (r SAR) Transverse sinus (TS) Left pulmonic recess # Para-aortic lymph nodes # Prevascular lymph nodes # Inferior tracheobronchial lymph nodes Oblique sinus - The oblique sinus is postero-superior to the left atrium and posteromedial to the left superior pulmonary vein Page 5 of 15 Posterior pericardial recess - The right superolateral extension of oblique sinus is the posterior pericardial recess - It is closely related to and mimics • • Subcarinal lymph nodes Tracheo-bronchial lymph nodes Oblique sinus (OS) Posterior pericardial recess # Subcarinal lymph nodes # Tracheo-bronchial lymph nodes Pericardial cavity proper - The recesses arising from the pericardial cavity proper are • • Right and left pulmonary venous recesses Post caval recess. Pulmonary venous recesses - Formed by the pericardium investing the pulmonary veins as they penetrate the fibrous pericardium to enter the left atrium - Located between the superior and inferior pulmonary veins along the lateral cardiac borders - Closely related to and mimic • Bronchopulmonary lymph nodes Post caval recess - Lies posterior to the SVC towards the right Pericardial cavity proper Pulmonary recesses venous # Bronchopulmonary lymph nodes Images for this section: Page 6 of 15 Fig. 2: Classification of Pericardial recesses © Department of Radiology, Amrita Institute of Medical sciences and Research centre, Kochi / India 2015 Page 7 of 15 Fig. 3: Anatomy of pericardial sinuses and recesses © Department of Radiology, Amrita Institute of Medical sciences and Research centre, Kochi / India 2015 Page 8 of 15 Fig. 4: Anatomy of pericardial sinuses and recesses © Department of Radiology, Amrita Institute of Medical sciences and Research centre, Kochi / India 2015 Page 9 of 15 Fig. 5: r-SAR & a-SAR mimicking pre vascular & para-aortic lymph node © Department of Radiology, Amrita Institute of Medical sciences and Research centre, Kochi / India 2015 Page 10 of 15 Fig. 6: Posterior-Superior aortic recess mimicking : Paratracheal lymph node (when cranially extended) and Pre-carinal lymph node © Department of Radiology, Amrita Institute of Medical sciences and Research centre, Kochi / India 2015 Page 11 of 15 Fig. 7: Left pulmonic recess mimicking AP window lymphnode © Department of Radiology, Amrita Institute of Medical sciences and Research centre, Kochi / India 2015 Page 12 of 15 Fig. 8: Oblique sinus & its posterior pericardial recess mimicking sub-carinal lymphnodes © Department of Radiology, Amrita Institute of Medical sciences and Research centre, Kochi / India 2015 Page 13 of 15 Conclusion # Pericardial recesses mimic various mediastinal lymphnodes # Following are the differentiating features on cross sectional imaging Pericardial recess Lymphnodes # Beaking, sharp margins # Rounded margins # Spread along the vessels # Indent the vessels # No post contrast enhancement # Post contrast enhancement (except necrotic lymphnodes) #Multiplanar reformatting and thin slice reconstruction helps to better differentiate recesses from lymphnodes Personal information Dr Saket Thakar MD Radiology Maharashtra, India Email: [email protected] References 1.Mylene T. Truong, Jeremy J. Erasmus, Gregory W. Gladish, Bradley S. Sabloff, Edith M. Marom, Jhon E. Madewell, Marvin H. Chasen, Reginald F. Mundane. Anatomy of Page 14 of 15 Pericardial Recesses on Multidetector CT : Implications for Oncologic Imaging. AJR 2003;181:1109-1113 0361-803X/03/1814-1109. 2.Reinhard Groell, MD. Gottfried J Schaffler, MD. Rainer Reinmueller, MD. Pericardial Sinuses and Recesses : Findings at Electrocardiographically Triggered Electron-Beam CT. Radiology 1999; 212:69-73. 3.Lynn S. Broderick, MD . Gregory N. Brooks, MD, PhD . Fanet E. Kuhlman, MD, MS. Anatomic Pitfalls of Heart and Pericardium. RadioGraphics 2005; 25:441-453. 4.S M O'Leary, P L Williams, M P Williams, A J Edwards, C A Roobottom, G J Morganhughes, N E Manghat. Imaging the pericardium : appearences on ECG-gated 64detectorrow cardiac computed tomography. The British Journal of Radiology, 83 (2010), 194-205. Page 15 of 15