Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
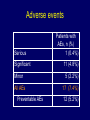
Involving Patients and Families in Patient Safety III Simposio Internacional de Seguridad del Paciente Centro Medico Imbanaco 16 de marco de 2012 Cali, Colombia Saul N. Weingart, MD, PhD Dana-Farber Cancer Institute and Harvard Medical School Boston, Massachusetts, USA The patient safety epidemic • 1999 Institute of Medicine (IOM) reports 44-98,000 excess deaths/year. • Calls for research, education, and improvement. 3 Two views Consumer patient safety recommendations • Learn to recognize liquid medications by smell. • Ask for a copy of your hospital MAR. Check it for accuracy. • Keep the lights on so you don’t accidentally take the wrong drug. • Keep people medicine separate from pet medicine. Objectives • What is the patient’s experience and understanding of medical error? • Can patients play a role in identifying medical error and preventing harm? Conditions for patients to prevent medical errors… Ability to behave safely Ability to communicate errors Ability to identify errors Can patients identify and communicate errors? Inpatient adverse event reporting study Weingart et al. JGIM 2005; 20: 837-41 • Do you believe that there have been any problems with your care during this hospitalization? • Do you believe that you were hurt or stayed in the hospital longer than necessary because of problems with your care? • Do you believe that anyone made a mistake that affected your care during this hospitalization? Serious adverse event “I had a PIC [percutaneous intravenous catheter] line put in and I got an abscess. They took me down to get surgery. I had a blood clot and they removed part of my vein.” Significant adverse event “My blood sugar went sky high because they did not give me my diabetes medication.” Life-threatening near miss “The doctor came in and suggested that I get a flu shot. I am allergic to it. It would kill me. Do the doctors not check patient charts?” Adverse events Serious Significant Minor All AEs Preventable AEs Patients with AEs, n (%) 1 (0.4%) 11 (4.8%) 5 (2.2%) 17 (7.4%) 12 (5.2%) • Design – Med/surg patients at 16 Massachusetts hospitals • Sample – 2,582 (62%) completed a post-discharge telephone survey – 998 also agreed to medical record review • Analysis – MD panel classified reports What do patients know that hospitals don’t? (n=998) Patient Reports 23% Both Patient Reports & Chart Review 5% Chart Review 11% Weissman, et al., Ann Intern Med. 2008; 149:100-108. In sum, many patients can identify and report “safety” events. Some screening may be necessary. Behaving safely Patients' Comfort Level in Performing Error Prevention Behaviors % Very Error Prevention Behavior N Comfortable Ask RN purpose of medication 948 91 Ask RN to confirm patient's ID 900 84 Have family/friend watch for errors 966 76 Helping health care staff mark surgical site 518 72 Ask medical personnel if they washed their hands 924 46 Waterman et al. JGIM 2006; 21: 367-70. Patients' Comfort Level in Performing Error Prevention Behaviors % Very Error Prevention Behavior N Comfortable % Who Took Action Ask RN purpose of medication 948 91 75 Ask RN to confirm patient's ID 900 84 38 Have family/friend watch for errors 966 76 39 Helping health care staff mark surgical site 518 72 17 Ask medical personnel if they washed their hands 924 46 5 Waterman et al. JGIM 2006; 21: 367-70. Factors that affect patient taking action • • • • • • Gravity of perceived threat Preventability Effectiveness of action Consequences of speaking up Self-efficacy Staff members’ instructions and expectations How can we promote engagement? Medication Reconciliation “Accurately and completely reconcile medications across the continuum of care” TJC National Patient Safety Goal Preliminary Findings No. of patients 338 No. of drugs 2146 Corrected 102 5% D/C’d drugs 510 24% Missing drugs 585 27% Total changes 1197 56% Patient-Identified Medication Updates • Corrected – Oxycontin – Mycophenolate mofetil – Gabapentin – Keppra – Warfarin • D/C’d – Antibiotics (various) – Antiemetics • Missing – – – – – – – – – Heparin Warfarin Imatinib Oxcarbazepine Erlotinib Testosterone Dexamethasone Thalidomide Celecoxib Medication Reconciliation Protocol CAs Prep Charts Collect & Evaluate Providers or Pharmacists Update EMR Patients Update Med Lists CAs Provide Med Lists Medication Reconciliation Monthly Totals 2500 2000 1500 Implement Sustain 1000 Develop 500 '07 M ar M ay Ju ly '0 7 Se pt No v Ja n '08 M ar ch Ja n No v Ju l '0 6 Se pt ay M ar M '06 Ja n '0 5 0 No v Medication sheets reconciled November 2005 - March 2008 Sheets reconciled 95% CI Reconciled Medication Lists Med List Updates Reconciliation Usual Care N=42 N=47 P-value Any 38 (90%) 1 (2%) <0.001 Mean no. of updates (s.d.) 4.3 (4.1) 0.1 (0.4) <0.001 A story MRI OF THE BRAIN WITHOUT AND WITH CONTRAST CLINICAL HISTORY: Headaches awakening the patient from sleep. TECHNIQUE: Multiplanar pre- and post-contrast T1-weighted images, axial T2weighted, susceptibility and FLAIR images were obtained. FINDINGS: There is an enhancing extra-axial mass at the anterior aspect of the right middle cranial fossa, broadly contiguous with the greater wing of the sphenoid bone and extending superiorly and projecting over the lesser wing of the sphenoid bone. The mass measures approximately 3.5 cm in anterior/posterior dimension by 4.5 cm in transverse dimension x as much as 4.4 cm in superior/inferior dimension. There is an enhancing dural tail and the appearance of the mass is most consistent with a meningioma. There is considerable right temporal edema and there is effacement of the right temporal sulci and the right temporal horn. The right lateral ventricle is smaller than the left and the septum pellucidum is shifted slightly towards the left. Superiorly, the frontal and parietal sulci are also smaller on the right than the left. There is some protrusion of the uncus medially and indentation of the right mid-brain without tourqing of it. No other masses are seen. The brain parenchyma is otherwise normal. The paranasal sinuses are essentially clear with minimal soft tissue thickening noted in the right maxillary sinus. IMPRESSION: There is a 4.5 cm, intensely enhancing, extra-axial mass at the anterior aspect of the right middle cranial fossa with an associated dural tail most consistent with a meningioma. There is extensive edema in the right temporal lobe, extending posteriorly and superiorly to involve the posterior aspects of the internal and external capsules. There is diffuse asymmetry of the right cerebral sulci and early right uncal herniation. The results were e-mailed to Dr. ##### at approximately 9:30 p.m. on 3/13/03. Teamwork training Teamwork training • Promising application in ICU, OR, ER, L&D • Key principles: – Appropriate assertiveness – Briefing – Close-loop communication – Situational awareness “I lift, you grab. Was that concept just a little too complex, Carl?” Revised approach • Campaign rather than education or research • Focus on hazards rather than skills – Wrong chemo, last-minute change, hand hygiene • Bringing messages to the patient • Empowerment without obligation – “You CAN… check, ask, notify” DANA-FARBER ADMITS DRUG OVERDOSE CAUSED DEATH OF GLOBE COLUMNIST, DAMAGE TO SECOND WOMAN 3/23/1995 When 39-year-old Betsy A. Lehman died suddenly last Dec. 3 at Boston's Dana-Farber Cancer Institute, near the end of a grueling three-month treatment for breast cancer, it seemed a tragic reminder of the risks and limits of high-stakes cancer care. In fact, it was something very different. The death of Lehman, a Boston Globe health columnist, was due to a horrendous mistake: a massive overdose of a powerful anticancer drug that ravaged her heart, causing it to fail suddenly…. In 2012, we proudly celebrate Adult Council for 14 years Pediatric Council for 11 years What can you do? • Educate: brochures, posters, etc. • Encourage patient reporting: problems, errors, “negative events” • Empower: Condition H • Engage: medication reconciliation • Use technology: portals • Use teamwork tools Questions… • How much can (and should) we rely on patients to ensure their own safe care? • Does patient participation signal a failure of our systems to prevent or trap errors? • Can we customize the approach for different patients with different capacities? • What safety behaviors (for patients) hold the most promise? Hollywood ending • 2002 national telephone survey of 1,207 patients • 42% of patients reported medical errors in their own or a family members’ care Blendon et al. NEJM 2002; 347: 1933-40