Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
History of invasive and interventional cardiology wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Jatene procedure wikipedia , lookup
Cardiac surgery wikipedia , lookup
Myocardial infarction wikipedia , lookup
Coronary artery disease wikipedia , lookup
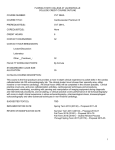
JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY VOL. 67, NO. 5, 2016 ª 2016 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 0735-1097/$36.00 PUBLISHED BY ELSEVIER http://dx.doi.org/10.1016/j.jacc.2015.10.090 U.S. Hospital Use of Echocardiography Insights From the Nationwide Inpatient Sample Alexander Papolos, MD, Jagat Narula, MD, PHD, Chirag Bavishi, MD, MPH, Farooq A. Chaudhry, MD, Partho P. Sengupta, MD, DM ABSTRACT BACKGROUND Increased use of echocardiography (echo) raises questions of whether echo is an overused diagnostic procedure in the United States. OBJECTIVES This study investigated national trends, practice patterns, and patient outcomes associated with inpatient echo use reported in the Nationwide Inpatient Sample (NIS). METHODS We identified admission diagnoses most commonly associated with echo use and performed multivariate logistic regression within each diagnosis cohort to assess whether echo use was associated with all-cause inpatient mortality. Secondary analysis was performed within our institution to validate use trends identified in the NIS database. RESULTS Between 2001 and 2011, the absolute volume and incidence of echo steadily increased at average annual rates of 3.41% and 3.04%, respectively. In 2010, the use of echo was associated with lower odds of inpatient mortality among hospitalizations for acute myocardial infarction (adjusted odds ratio [OR]: 0.74; 95% confidence interval [CI]: 0.63 to 0.86; p < 0.001), cardiac dysrhythmia (adjusted OR: 0.72; 95% CI: 0.55 to 0.94; p ¼ 0.02), acute cerebrovascular disease (adjusted OR: 0.36; 95% CI: 0.31 to 0.42; p < 0.001), congestive heart failure (adjusted OR: 0.82; 95% CI: 0.72 to 0.94; p ¼ 0.005), and sepsis (adjusted OR: 0.77; 95% CI: 0.70 to 0.85; p < 0.001). In 2010, these 5 diagnoses accounted for 3.7 million hospital admissions (9% of all hospitalizations); however, echo was reported in only 8% of cases. Secondary analysis of imaging practices at our institution confirmed underuse of echo among patients who died during hospitalization for indications identified in the NIS database. CONCLUSIONS Despite increasing rates of performance, echo may be underused during critical cardiovascular hospitalizations. (J Am Coll Cardiol 2016;67:502–11) © 2016 by the American College of Cardiology Foundation. E chocardiography (echo) is the most ubiqui- showed that the use of echo (transthoracic echocardi- tous, versatile, and cost-effective cardiac ography [TTE] and transesophageal echocardiogra- imaging These phy [TEE]) increased by 7.7% per year from 1999 to attributes, in combination with an infinitesimal risk- 2004 (5), and it nearly doubled from 1999 to 2008 to-benefit ratio, explain why echo has become a (6). Reports from the Veterans Healthcare Adminis- mainstay of the cardiovascular evaluation. Wide- tration also demonstrated an annual increase in total spread reliance on echo has fostered growing concern echo volume of 3.9% from 2000 to 2007, but this for its overuse and has led to the formation of appro- finding was primarily driven by population expansion priate use criteria (1). Although several studies have rather than by a change in imaging practices (7). demonstrated adherence to these guidelines in Given the paucity of data, this study was conducted clinical practice (2–4), national trends in the use of to describe trends, practice patterns, and patient echo have not been fully described. The closest ap- outcomes associated with the use of echo through proximations are from Medicare literature, which a comprehensive assessment of hospitalizations modality available (1–5). Listen to this manuscript’s audio summary by JACC Editor-in-Chief Dr. Valentin Fuster. From the Mount Sinai Medical Center, New York, New York. Dr. Narula has received research grants to the institution from Philips Healthcare and GE Healthcare in the form of equipment. Dr. Sengupta is an advisor to Saffron Technology Hearts Labs; and is a consultant to Edwards Lifesciences. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose. Brian Griffin, MD, served as Guest Editor for this paper. Manuscript received August 28, 2015; revised manuscript received October 7, 2015, accepted October 8, 2015. Papolos et al. JACC VOL. 67, NO. 5, 2016 FEBRUARY 9, 2016:502–11 503 Echocardiography Use in U.S. Hospitals available in the Nationwide Inpatient Sample (NIS) artery disease (CAD), sepsis, valvular disease, ABBREVIATIONS database (8). and nonspecific chest pain (CCS diagnoses AND ACRONYMS codes: 2, 96, 100, 102, 101, 106, 108, and 109). METHODS We subsequently applied 3 criteria to the We first queried the NIS to quantify temporal trends in inpatient echo use between 2001 and 2011. Next we explored the 2010 database to investigate whether echo use was associated with all-cause in-hospital mortality among the diagnoses for which echo is most commonly performed. sample: 1) non–emergency department ad- AMI = acute myocardial infarction APR-DRG = All Patient missions were excluded to control for con- Refined–Diagnosis Related founding hospital-to-hospital transfers; 2) Group Severity Score hospitalizations lasting <24 h were excluded CAD = coronary artery disease to counter bias created by critically ill patients CCS = Clinical Classification in whom a fatal outcome occurred without Software sufficient lead time to obtain an echo exami- CHF = congestive heart failure DATA SOURCE. The NIS is the largest, publicly nation if clinically indicated; and 3) neonatal echo = echocardiography available, all-payer inpatient database in the United patients were excluded. The final sample ICD-9-CM = International included an estimated 3,651,503 hospitaliza- Classification of Disease-9th States (8). Annually, the NIS is composed of discharge-level data from roughly 8 million hospi- tions and contained 31% of all estimated talizations and approximates a stratified sample of inpatient echo examinations performed in 20% of community hospitals in the United States. The 2010. State-specific rates of inpatient echo use sampling methodology of the NIS permits the appli- were derived by dividing estimated statewide cation of weighting variables that allow for the echo volume by the corresponding volume of calculation of national estimates, which have been estimated hospitalizations, as recorded in the validated against other U.S. hospital registries (9). 2010 NIS. edition-Clinical Modification NIS = Nationwide Inpatient Sample OR = odds ratio TEE = transesophageal echocardiography TTE = transthoracic echocardiography Each hospitalization within the database contains Patients’ PATIENT-RELATED AND HOSPITAL CHARACTERISTICS. diagnoses are documented in parallel, as both Inter- To assess for association between echo performance national Classification of Disease-9th edition-Clinical and diagnosis-specific hospital mortality rates, we clinical and resource-use information. Modification (ICD-9-CM) and clinically meaningful stratified the sample by primary CCS diagnosis code clusters of ICD-9-CM’s, termed Clinical Classification (admission diagnosis). Available independent vari- Software (CCS) codes. ables for analyses included the patient’s age, race, sex, insurance status, number of comorbidities, SEE PAGE 512 median household income by zip code, illness severity score, and admission day (weekend vs. TEMPORAL TRENDS IN ECHO USE. The Healthcare weekday). Information on race was categorized as Cost and Utilization Project online NIS registry white, black, Hispanic, and other (Asian, Pacific (HCUPnet) (10) was queried by the ICD-9-CM for echo Islander, Native American, and unknown). Insurance (procedure code 88.72). This provided national esti- status was classified based on the expected primary mates of hospitalizations in which echo was per- payer and included Medicare, Medicaid, private in- formed from 2001 through 2011. The ICD-9-CM 88.72 surance, and other insurance types, including pa- is used for coding of all forms of echo. Therefore the tients who were uninsured. The number of comorbid database cannot differentiate admissions in which conditions was a sum of all listed diagnoses. Median TTE examinations or other forms of echo such as TEE household were performed. However, this limitation is likely to divided into income quartiles defined as follows: be insignificant given that the approximate ratio of 1) $1 to $40,999; 2) $41,000 to $50,999; 3) $51,000 TTE use to TEE use is close to 100:1 (6), as well as the income per patient’s zip code was to 66,999; and 4) $$67,000. Illness severity was clinical insight that few patients receive TEE without based on All Patient Refined–Diagnosis Related first undergoing TTE. Group (APR-DRG) severity score, a validated clini- STUDY POPULATION. The 2010 NIS was used to eval- uate for an association between echo use and diagnosis specific all-cause hospital mortality. The dataset was first confined to admission diagnoses associated with the greatest proportion of echo use (representing one-half of all estimated inpatient echo studies in cally coherent set of illness severity and risk of mortality subclasses that adjust for the interactions between a patient’s primary diagnosis, comorbidities, age, and procedures occurring during hospitalization, defined as: 1) minor; 2) moderate; 3) major; and 4) extreme (11). 2010) (10). This included acute myocardial infarction HOSPITALIZATION (AMI), cardiac dysrhythmia, acute cerebrovascular point was in-hospital mortality and was analyzed OUTCOME. The disease, congestive heart failure (CHF), coronary using multivariate regression, as described later. primary end- 504 Papolos et al. JACC VOL. 67, NO. 5, 2016 FEBRUARY 9, 2016:502–11 Echocardiography Use in U.S. Hospitals STATISTICAL ANALYSIS. Temporal trends in the distribution of the NIS study sample. We attempted to incidence of national echo use per hospitalization correct for this disparity and more closely emulate the between 2001 and 2011 were obtained by dividing the NIS study sample by including only patients who estimated annual volume of studies performed by the were $60 years of age. We then performed both estimated total number of annual hospitalizations. univariate analysis and multivariate logistic regres- Use growth (absolute and per hospitalization) was sion adjusting for patients’ sex, race, insurance type, analyzed by calculating the average annual percent- number of chronic diseases, administration of diag- age change from 2001 to 2011. nostic cardiac catheterization or cardiac stress test, The 2010 sample was dichotomized into hospitali- admission day, and APR-DRG severity index among zations in which echo was or was not performed, and each admission-diagnosis cohort to assess for an as- descriptive statistics were generated on frequencies sociation between echo performance and hospital and proportions for categorical variables (age, sex, mortality rates. race, insurance, income quartile by zip code, number Results were reported as adjusted odds ratios (ORs) of chronic diseases, administration of diagnostic car- with 95% confidence intervals (CIs). All statistical diac catheterization, administration of cardiac stress analyses incorporated primary sampling units and test [exercise and pharmacologic], admission day, clusters to obtain national estimates and were per- and APR-DRG severity score). Means with standard formed using Statistical Analysis Software (SAS, Cary, error were reported for continuously coded variables North Carolina) version 9.3 with a 2-sided significance (age and number of chronic diseases). Student t tests level set at p < 0.05. and the chi-square tests were used to evaluate This study was considered to be exempt research demographic features among groups. To assess with respect to the requirement for informed con- for an association between echo performance and sent, as assessed by the Mount Sinai Medical diagnosis-specific hospital mortality rates, we strati- Center Institutional Review Board. All authors vouch fied the sample by admission diagnosis (primary for the accuracy and completeness of the data CCS diagnosis code). Within each subpopulation presented. multivariate logistic regression was conducted on weighted numbers and was adjusted for patients’ age, sex, race, insurance, income quartile by zip code, number of chronic diseases, administration of diagnostic cardiac catheterization, administration of cardiac stress test, admission day, and APR-DRG severity score. Diagnostic catheterization was adjusted for, despite no significant difference observed between the sample arms, because it could potentially portend a mortality bias. RESULTS ANALYSIS OF TRENDS. An estimated 7,669,000 echo examinations were performed in U.S. hospitals from 2001 to 2011. During this period, echo use grew at an average annual rate of 3.41% (Central Illustration, panel A). An evaluation of resource use and patients’ outcomes found that hospitalizations in which echo was coded as the primary procedure had declining rates of hospital mortality and length of stay. How- SINGLE-CENTER VALIDATION ANALYSIS. To vali- date our analysis of the NIS we evaluated all hospitalizations that occurred during the calendar year 2014 within our home institution, a large tertiary academic medical center in New York City. The ICD-9-CM procedure code 88.72 was reported by ever, these trends were associated with rising hospitalization charges (Central Illustration, panels B to D). These trends motivated us to undertake a detailed analysis for investigating whether underuse of echo may be related with hospital outcomes and thus serve as a marker of clinical care. Mount Sinai hospital for reportable inpatient TTE GEOGRAPHIC ECHO DISTRIBUTION. The highest rates performed before October 1, 2015. The calendar year of echo use per hospitalization were observed 2014 hospitalizations, throughout the East Coast (Figure 1). On a state-by-state among which we gated on the 8 admission diagnoses basis, Rhode Island, New York, and Montana were of interest and applied the same inclusion criteria as the leading inpatient echo users, whereas the lowest described earlier. The population was dichotomized rates were observed in Wyoming, Alaska, and by the performance or lack thereof inpatient echo, New Mexico. and demographic features were compared using 2010 NATIONWIDE INPATIENT SAMPLE AND SAMPLE sample contained 57,547 Student t tests and chi-square tests as appropriate. DEMOGRAPHICS. Table 1 displays the 2010 NIS and the We observed that the average age in the echo group study population stratified by echo use and categor- was advanced 11 years beyond that of the nonecho ical variables. An estimated 816,500 echo exami- group; this was markedly different from the age nations were performed nationally in 2010, Papolos et al. JACC VOL. 67, NO. 5, 2016 FEBRUARY 9, 2016:502–11 CENTRAL I LLU ST RAT ION Echocardiography Use in U.S. Hospitals U.S. Hospital Trends in Echo Use: 2001 to 2011 Papolos, A. et al. J Am Coll Cardiol. 2016; 67(5):502–11. (A) Annual national volume (shaded area) and incidence (dashed line) of echocardiography (echo) use per hospitalization. (B) Average charge of hospitalization in which echo was coded as the principal procedure performed versus the national average. (C) Average length of hospitalization in which echo was coded as the principal procedure performed versus the national average. (D) Incidence of inpatient mortality of hospitalizations in which echo was coded as the principal procedure performed versus the national average. LOS ¼ length of stay. corresponding to 2.09% of all hospital admissions for morbidity (p < 0.001), and had more chronic medical that year. As expected, the proportion of hospi- problems (p < 0.001) (Table 1). talizations in which echo was performed was signifi- SAMPLE ECHO RATES. The prevalence of echo use in cantly higher within our sample (7.01%; p < 0.001). the admission-diagnosis cohorts was as follows: The distributions observed within categorical vari- valvular disease (22%), acute cerebrovascular disease ables were similar between the echo and nonecho (12%), cardiac dysrhythmia (10%), CHF (7%), AMI arms of our study population. However, significant (6%), CAD (6%), sepsis (5%), and nonspecific chest differences were observed across all domains, barring pain (4%) (Figure 2). To explore the surprising low use of diagnostic cardiac catheterization. In a com- echo rates reported in patients with AMI and CAD, we parison of the 2 sample arms, patients undergoing scrutinized the uses of parallel imaging modalities echo were younger (p < 0.001), received more cardiac capable of providing a determination of ventricular stress tests (p < 0.001), resided in higher-income zip function. Rates of both cardiac stress testing and codes (p < 0.001), were at higher risk of death and cardiac magnetic resonance imaging were negligibly 505 506 Papolos et al. JACC VOL. 67, NO. 5, 2016 FEBRUARY 9, 2016:502–11 Echocardiography Use in U.S. Hospitals F I G U R E 1 Echo Use per 100,000 Hospitalizations by State, 2010 Ontario North Dakota Idaho New Hampshire Massachusetts Rhode Island Delaware New Jersey District of Columbia Alabama MEXICO The highest inpatient echocardiography (echo) use was seen in Rhode Island, New York, and Montana, whereas the lowest rates were observed in Wyoming, Alaska, and New Mexico. low, and cardiac computed tomography documenta- SINGLE-CENTER VALIDATION ANALYSIS. Between tion was variable. However, as expected, a large 2003 and 2014, the incidence of echo use per hospi- proportion of the AMI and CAD cohorts underwent talization at the Mount Sinai Medical Center steadily diagnostic coronary catheterization (64% and 62%, increased at an average annual rate of 4.75%. Echo respectively) (Figure 2). was performed during 14.6% of the 57,547 hospitalizations in 2014. Of these hospitalizations, 18,401 were MORTALITY ANALYSIS. Multivariate logistic regres- for 1 of the 8 admission diagnoses of interest and met sion adjusting for key variables (age, sex, race, in- the inclusion criteria previously described. Within surance, income quartile by zip code, number of this population we observed that the patients un- chronic diseases, administration of diagnostic cardiac dergoing echo were older (p < 0.001), more likely to catheterization, and administration of cardiac stress receive diagnostic coronary catheterization or stress testing, admission day, and APR-DRG severity score) testing (p < 0.001), and more critically ill (p < 0.001) within each admission-diagnosis cohort was per- (Online Table 1). formed to evaluate for association between echo use In our analysis of imaging practices in our home and the odds of a patient’s death. We found that the institution we observed underuse of echo for in- use of echo was associated with significantly lower dications identified in the NIS database (Table 2), odds of all-cause hospital mortality in AMI (adjusted most notably among patients with AMI, 25% of whom OR: 0.74; 95% CI: 0.63 to 0.86; p < 0.001), cardiac were discharged without echo evaluation and 17% of dysrhythmia (adjusted OR: 0.72; 95% CI: 0.55 to 0.94; whom were discharged without any form of cardiac p ¼ 0.02), acute cerebrovascular disease (adjusted OR: imaging. Death occurred in 9.4% of patients admitted 0.36; 95% CI: 0.31 to 0.42; p < 0.001), CHF (OR: 0.82; for AMI, and the mortality rate was marginally higher 95% CI: 0.72 to 0.94; p ¼ 0.005), and sepsis (adjusted in those patients in which echo was not performed OR: 0.77; 95% CI: 0.70 to 0.85; p < 0.001). Significance (10.1% vs. 9.1%), although this difference was not was not observed in the subsamples for CAD (adjusted statistically significant (p ¼ 0.14). OR: 0.66; 95% CI: 0.40 to 1.08; p ¼ 0.09), valvular The association between echo performance and the disease (adjusted OR: 0.71; 95% CI: 0.40 to 1.25; odds of inpatient mortality did not reach significance p ¼ 0.24), or nonspecific chest pain (adjusted OR: 0.75; in 6 of the remaining 7 admission diagnoses. Notably, 95% CI: 0.18 to 3.15; p ¼ 0.7) (Figure 3). however, 42% of patients who died during Hospitalizations Age, yrs Sample Without Echo Echo 39,008,298 38,191,759 816,539 48.36 0.37 48.07 0.38 62.22 0.64 p Value <0.001 Total Without Echo Echo 3,651,503 3,395,355 256,148 68.18 0.19 68.34 0.18 66.43 0.49 p Value <0.001 Sex Male 16,485,595 (42) 16,057,035 (42) 428,560 (52) <0.001 1,825,729 (50) 1,689,377 (50) 136,352 (53) <0.001 Female 22,436,406 (58) 22,048,547 (58) 387,859 (48) <0.001 1,824,942 (50) 1,705,188 (50) 119,755 (47) <0.001 White 22,564,721 (65) 22,116,303 (65) 448,417 (62) 0.0269 2,316,389 (69) 2,168,212 (70) 148,177 (63) 0.013 Black 5,577,833 (16) 5,428,059 (16) 149,774 (21) 562,055 (17) 513,749 (17) 48,306 (21) Hispanic 4,219,597 (12) 4,148,024 (12) 71,574 (10) 287,797 (9) 264,819 (9) 22,977 (10) Other 2,245,104 (6) 2,196,558 (6) 48,547 (7) 82,241 (2) 76,836 (2) 5,405 (2) JACC VOL. 67, NO. 5, 2016 2010 NIS Total FEBRUARY 9, 2016:502–11 T A B L E 1 2010 NIS and Study-Sample Demographics* Race Payer <0.001 Medicare 14,544,759 (37) 14,113,915 (37) 430,844 (53) 2,265,956 (62) 2,121,589 (63) 144,367 (56) Medicaid 8,272,829 (21) 8,167,081 (21) 105,749 (13) 347,149 (10) 319,843 (9) 27,307 (11) Private 1,2454,459 (32) 12,254,377 (32) 200,082 (25) 739,257 (20) 681,129 (20) 58,127 (23) 2,131,556 (5) 2,076,304 (5) 55,253 (7) 189,649 (5) 170,769 (5) 18,880 (7) 209,751 (1) 205,171 (1) 4,580 (1) 19,307 (1) 17,679 (1) 1,628 (1) 1,300,605 (3) 1,281,727 (3) 18,877 (2) 82,241 (2) 76,836 (2) 5,405 (2) No 37,725,470 (97) 37,003,688 (97) 721,782 (88.4) 3,041,068 (83) 2,826,660 (83.2) 214,408 (83.7) Yes 1,282,828 (3) 1,188,071 (3) 94,757 (11.6) 610,435 (17) 568,696 (16.8) 41,740 (16.3) No 38,917,418 (99.8) 38,127,941 (99.8) 789,476 (96.7) 3,603,854 (99) 3,361,029 (99) 242,825 (94.8) Yes 90,880 (0.2) 63,818 (0.2) 27,063 (3.3) 47,650 (1) 34,327 (1) 13,323 (5.2) 1–40,999 11,275,123 (30) 11,051,276 (30) 223,847 (29) 1,043,876 (29) 977,149 (30) 66,727 (27) 41,000–50,999 9,670,553 (25) 9,501,298 (26) 169,255 (22) 898,297 (25) 848,776 (26) 49,522 (20) 51,000–66,999 9,120,533 (24) 8,949,167 (24) 171,366 (22) 863,755 (24) 809,683 (24) 54,072 (22) 67,000þ 7,907,969 (21) 7,690,712 (21) 217,257 (28) 751,136 (21) 675,928 (20) 75,208 (31) No 31,320,829 (80) 30,675,493 (80) 645,336 (79) 2,693,958 (74) 2,501,627 (74) 192,331 (75) Yes 7,676,673 (20) 7,505,470 (20) 171,203 (21) 957,545 (26) 893,729 (26) 63,816 (25) Self No charge Other <0.001 Imaging Diagnostic catheterization <0.001 0.576 Stress test† <0.001 <0.001 Income quartile, U.S. $ 0.0027 <0.001 <0.001 <0.001 Severity index‡ <0.001 57,911 (0) 57,592 (0) 319 (0) 257 (0) 246 (0) 11 (0) 13,278,231 (34) 13,176,047 (34) 102,184 (13) 572,391 (16) 537,942 (16) 34,449 (13) 2 14,144,527 (36) 13,885,989 (36) 258,538 (32) 1,285,850 (35) 1,197,068 (35) 88,783 (35) 3 8,815,466 (23) 8,517,016 (22) 298,449 (37) 1,185,136 (32) 1,097,150 (32) 87,986 (34) 4 Number of chronic diseases 2,712,163 (7) 25,55,114 (7) 157,049 (19) 3.84 0.042 3.79 0.043 6.20 0.101 <0.001 607,868 (17) 562,949 (17) 44,919 (18) 6.4 0.053 6.38 0.054 6.72 0.107 <0.001 <0.001 Papolos et al. 0 1 Echocardiography Use in U.S. Hospitals Weekend admission Values are n, mean SE, or n (%). *p values comparing categorical variables between the echocardiography and nonechocardiography arms of each population were derived from Student t tests or chi-square test as appropriate. †Exercise and pharmacological cardiac stress test. ‡All Patient Refined–Diagnosis Related Group severity score. 507 Echo ¼ echocardiography; NIS ¼ Nationwide Inpatient Sample. 508 Papolos et al. JACC VOL. 67, NO. 5, 2016 FEBRUARY 9, 2016:502–11 Echocardiography Use in U.S. Hospitals F I G U R E 2 Sample Rates of Diagnostic Cardiac Catheterization and Echo by Admission Diagnosis 70% Cath Echo 60% 50% 40% 30% 20% 10% 0% AMI CAD Nonspecific chest pain CHF Dysrhythmia Sepsis Acute Valvular heart cerebrovascular disease disease AMI ¼ acute myocardial infarction; CAD ¼ coronary artery disease; Cath ¼ cardiac catheterization; CHF ¼ congestive heart failure; Echo ¼ echocardiography. hospitalization with reasons related to their primary available all-payer inpatient database in the United diagnosis did not undergo an echo examination States suggests that echo maybe underused for com- before death (Table 2). mon and appropriate indications. The cumulative use of parallel imaging modalities capable of providing an assessment of cardiac function NATIONAL ECHO USE. Between 2001 and 2011, the other than echo (contrast ventriculogram, cardiac absolute volume and incidence of echo per hospital- computed tomography, radionuclide ventriculogram, ization steadily increased at average annual rates of cardiac magnetic resonance imaging, pharmacological 3.41% and 3.04%, respectively, less than one-half the and nonpharmacological stress testing) per diagnosis average annual growth rate described among Medi- cohort were similar to our findings nationally (Online care beneficiaries from 1999 to 2004 by Pearlman Table 2). The reason for the lack of echo in these pa- et al. (5). This discrepancy likely reflects differences tients, however, could not be established during the in study populations because our demographic was analysis. specific to the inpatient setting and pertained to an all-payer population. This finding implies high rates of echo use among Medicare beneficiaries in the DISCUSSION outpatient domain. Widespread availability and familiarity with echo performance per hospitalization was 2.09% in 2010, have led to concern for its potential overuse. which is consistent with an independent assessment Recently, investigators have reported that echo use of the NIS database reported previously (12). The nearly doubled between 1999 and 2008 (6), consti- geographic distribution of echo use was heteroge- tuting approximately one-half of all cardiac imaging neous, with the highest rates observed on the East services among Medicare beneficiaries (5). Interest- Coast. These results are consistent with previous re- ingly, however, our analysis of the largest publicly ports of echo use among Medicare beneficiaries in Overall, the estimated national incidence of echo Papolos et al. JACC VOL. 67, NO. 5, 2016 FEBRUARY 9, 2016:502–11 Echocardiography Use in U.S. Hospitals 1995 by Lucas et al (13). Although our analysis did not lead to a definitive explanation for regional variation F I G U R E 3 Adjusted Odds Ratio (95% CI) of In-Hospital Death in Patients Who Underwent Echo by CCS Admission Diagnosis in echo use, we speculate that this variation may reflect geoeconomic disparities in access to health Diagnosis care, previously described geographic variation in Cardiac Dysrhythmia diagnostic practices, and elevated age-adjusted major cardiovascular death rates in the region (14,15). Acute Cerebrovascular Disease CHF MORTALITY RATES IN PATIENTS UNDERGOING ECHO. In 2010, approximately one-half of all inpa- tient echo examinations could be identified in the NIS database during hospital admissions for AMI, cardiac CAD Sepsis AMI dysrhythmia, acute cerebrovascular disease, CHF, CAD, sepsis, valvular disease, and nonspecific chest pain. Adjusting for key variables, we observed that Heart Valve Diseases Nonspecific Chest Pain the use of echo was associated with lower odds of hospital mortality among 5 of these disease pro0.0 cesses. As the least expensive and lowest-risk cardiac 0.5 1.0 3.0 imaging modality available (16), echo is a first-tier diagnostic tool that routinely leads to the initiation Results control for age, sex, race, insurance, income quartile by zip code, number of of various therapeutic interventions such as heart chronic diseases, All Patient Refined–Diagnosis Related Group (APR-DRG) severity index, failure regimens, use of implantable devices, surgery, and revascularization, all of which have been shown administration of cardiac catheterization and/or cardiac stress test, and admission day. Cath ¼ coronary catheterization; CCS ¼ Clinical Classification Software (codes); CI ¼ confidence interval; other abbreviations as in Figure 2. to improve mortality rates in the appropriate clinical setting (17). Although this study was not designed to determine a causal link between echo and patients’ outcomes, we believe that the association observed here is the product of information provided by echo that assists physicians in management decisions and patient risk stratification. This hypothesis is supported by a study conducted in a major academic medical center, which found that 32% of inpatient echo examinations led to an active change in medical care (3). Extrapolation of this intervention rate could explain the positive association observed in our analysis. The argument could be made that patients treated in larger medical centers equipped with comprehen- catheterization, and assuming that ejection fraction was approximated by contrast ventriculography, an assessment of cardiac function could not be substantiated in roughly 30% of this group. Although low rates of echo use in the NIS database may reflect underreporting because echo may not be required for reimbursement by DRG assignments (non-DRG procedures), the data continue to highlight underuse of functional cardiac assessment, as reported in previous investigations. A population-based study of 2,317 patients hospitalized with myocardial infarction from the Mayo Clinic in Minnesota reported that the sive ancillary and diagnostic services would be more likely to receive an echo examination and perhaps T A B L E 2 Single-Center Echo Use Rates* have access to more expert physicians. This position would impose a significant bias toward echo use and improved patient outcomes. For this reason we find it Diagnosis Echo Use Echo Use in Patients With Death Related to Primary Diagnosis important to convey that there was no difference in CAD 1,287/3,439 (37) 79/131 (60) the distribution of echo use among hospitalizations in Dysrhythmia 1,587/3,704 (43) 115/208 (55) small, medium, or large medical centers for the CHF 927/1,744 (53) 58/81 (72) Sepsis 514/1,467 (35) 108/220 (49) 16/29 (55) admission diagnoses studied. Acute cerebrovascular disease 380/734 (52) DIAGNOSIS-SPECIFIC ECHO RATES. The use of echo for NSCP 309/655 (47) the initial evaluation and re-evaluation of ventricular Valvular heart disease 525/1,011 (52) 35/52 (67) function after acute coronary syndrome is in accor- AMI 208/277 (75) 19/26 (73) dance with current standards of care and is supported by appropriate use criteria (1). However in 2010, echo was identified in only 6.2% of our AMI cohort. Within this cohort, 64% underwent diagnostic coronary 7/7 (100) Values are n/N (%). *Admission diagnosis–specific rates of echo use within our single-center sample and among the subpopulation of admissions in which inpatient death occurred. AMI ¼ acute myocardial infarction; CAD ¼ coronary artery disease; CHF ¼ congestive heart failure; Echo ¼ echocardiography; NSCP ¼ nonspecific chest pain. 509 510 Papolos et al. JACC VOL. 67, NO. 5, 2016 FEBRUARY 9, 2016:502–11 Echocardiography Use in U.S. Hospitals use of echo within the first 30 days after AMI database, the NIS data are subject to potential over- increased from 14% in 1979 to 65% by 1986 (18). sights in documentation and coding. The low use of Another study from Olmsted County, Minnesota echo in the NIS database may simply represent insti- compiled features of 791 patients who developed tutional underreporting of ICD-9-CM procedure cod- heart failure after AMI and reported that left ven- ing in the inpatient claim data. Because the database tricular function was not assessed after the diagnosis comprises survey-level data of de-identified dis- of heart failure in 38% of patients (19). More recently, charge information, coding inaccuracy, coding preci- data from the Worcester Heart Attack Study reported sion, and readmission data cannot be corrected for. that in 2003, echo was used in slightly more than 50% Indications for echo administration are not recorded of patients hospitalized for AMI and that ejection in the NIS, so admission diagnosis was used as a fraction was not assessed among 27% of patients surrogate. The NIS does not provide information before discharge (20). about survival beyond the inpatient period; hence, We attempted to investigate AMI-related cardiac longer-term outcomes are unknown. Finally, the imaging practices in our home institution. In our sample size of our single-center validation cohort was sample of 277 admissions to the Mount Sinai Medical underpowered to demonstrate a significance associ- Center in 2014 for AMI, we found that 75% of these ation between echo and mortality; larger prospective patients studies are needed. underwent echo, and 41% underwent another mode of cardiac imaging, primarily coronary artery catheterization. We found that 17% of patients admitted for AMI were discharged without an assessment of cardiac function. Of these 277 hospitalizations, 26 were associated with the patient’s death (9.4%), and among those who died, cardiac imaging was not performed in 27%. Similarly, the appropriate use criteria support the re-evaluation of cardiac function by echo among patients with heart failure, arrhythmia, and known valvular disease in the event of a change in clinical status without a clear precipitant (1). In our nationally representative sample, rates of echo use among patients requiring hospitalization with these admission diagnoses ranged from 7% to 22%. We confirmed our observation that echo is underused on the national level by demonstrating the underuse of echo in a tertiary care referral center located in one of the most diagnostically advanced regions in the United States. However, multivariate mortality analysis of our single-center cohort did not reach statistical significance. Low rates of echo performance observed nationally may in part be explained by the diagnostic stewardship of physicians or by cost bundling agreements between insurance companies and hospitals that place extra incentives to shift inpatient procedures CONCLUSIONS Echo use was associated with decreased odds of hospital mortality among 5 of the leading 6 admission diagnoses for which echo was most commonly reported in the 2010 NIS database. These 5 diagnoses account for approximately 3.7 million national hospitalizations annually; however, in 2010 the NIS database reported echo use in only 8% of cases. Because patient selection and appropriate echo use are key to cost efficiency, this study suggests that echo may be underused during critical cardiovascular hospitalizations, most notably in the treatment of AMI. REPRINT REQUESTS AND CORRESPONDENCE: Dr. Partho P. Sengupta, Mount Sinai’s Zena and Michael A. Wiener Cardiovascular Institute, Marie-Josée Gustave L. Levy Place, New York, New York 10029. E-mail: [email protected]. PERSPECTIVES COMPETENCY IN SYSTEMS-BASED PRACTICE: Patients hospitalized with myocardial infarction, heart failure, cardiac dysrhythmia, acute cerebrovascular into the post-discharge outpatient domain. ischemia, or sepsis who underwent echo faced a lower STUDY LIMITATIONS. Considerable caution is required in interpreting the results of the study. Information in the NIS is generated from discharge abstracts designed to facilitate hospital payment. These abstracts customarily are prepared by trained coding specialists after reviewing inpatient medical records to capture provider care and services that warrant reimbursement. Just as in any other administrative and Henry R. Kravis Center for Cardiovascular Health, One likelihood of inpatient mortality than did patients without echo. TRANSLATIONAL OUTLOOK: Further studies are required to clarify the links between access to echo and clinical outcomes among hospitalized patients in the United States. Papolos et al. JACC VOL. 67, NO. 5, 2016 FEBRUARY 9, 2016:502–11 Echocardiography Use in U.S. Hospitals REFERENCES 1. Douglas PS, Khandheria B, Stainback RF, et al. ACCF/ASE/ACEP/AHA/ASNC/SCAI/SCCT/SCMR 2008 appropriateness criteria for stress echocardiography: a report of the American College of Cardiology Foundation Appropriateness Criteria Task Force, American Society of Echocardiography, American College of Emergency Physicians, American Heart Association, American Society of Nuclear Cardiology, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, and Society for Cardiovascular Magnetic Resonance Endorsed by the Heart Rhythm Society and the Society of Critical Care Medicine. J Am Coll Cardiol 2008;51: 1127–47. 2. Ballo P, Bandini F, Capecchi I, et al. Application of 2011 American College of Cardiology Foundation/American Society of Echocardiography appropriateness use criteria in hospitalized patients referred for transthoracic echocardiography in a community setting. J Am Soc Echocardiogr 2012;25:589–98. 3. Matulevicius S, Rohatgi A, Das S, Price AL, DeLuna A, Reimold S. Appropriate use and clinical impact of transthoracic echocardiography. JAMA Intern Med 2013;173:1600–7. 4. Patil HR, Coggins TR, Kusnetzky LL, Main ML. Evaluation of appropriate use of transthoracic echocardiography in 1,820 consecutive patients using the 2011 revised appropriate use criteria for echocardiography. Am J Cardiol 2012;109:1814–7. 5. Pearlman AS, Ryan T, Picard MH, Douglas PS. Evolving trends in the use of echocardiography: a study of Medicare beneficiaries. J Am Coll Cardiol 2007;49:2283–91. 6. Andrus BW, Welch HG. Medicare services provided by cardiologists in the United States: 1999– 2008. Circ Cardiovasc Qual Outcomes 2012;5:31–6. 7. Okrah K, Vaughan-Sarrazin M, Cram P. Trends in echocardiography utilization in the Veterans Administration Healthcare System. Am Heart J 2010;159:477–83. 8. Healthcare Cost and Utilization Project. Facts and Figures: Statistics on Hospital-Based Care in the United States 2010. Available at: https://www. hcup-us.ahrq.gov/db/nation/nis/NIS_Introduction_ 14. Song Y, Skinner J, Bynum J, Sutherland J, Wennberg JE, Fisher ES. Regional variations in diagnostic practices. N Engl J Med 2010;363:45–53. 2010.jsp. Accessed September 20, 2014. 15. Go A, Mozaffarian D, Roger V, et al. Heart disease and stroke statistics—2013 update: a report from the American Heart Association. Circulation 2013;127:143–52. 9. Whalen D, Houchens R, Elixhauser A. 2004 HCUP Nationwide Inpatient Sample (NIS) Comparison Report. HCUP Methods Series Report 16. Ferrari VA, Whitman B, Blankenship JC, et al. Cardiovascular imaging payment and reimbursement systems: understanding the past and present #2007-03. Online February 2, 2007. U.S. Agency for Healthcare Research and Quality. Available at: https://www.hcup-us.ahrq.gov/db/ nation/nis/reports/2004niscomparisonrpt.jsp. Accessed September 20, 2014. in order to guide the future. J Am Coll Cardiol Img 2014;7:324–32. 10. Healthcare Cost and Utilization Project. Agency for Healthcare Research and Quality, Rockville, MD. 1999–2011. Available at: http:// hcupnet.ahrq.gov/HCUPnet.jsp?Id¼DB97390A368 039A9&Form¼SelLAY&JS¼Y&Action¼%3E%3ENext %3E%3E&_LAY¼Researcher. Accessed September 20, 2014. 11. Averill R, Goldfield N, Hughes J, et al. 3M APR-DRG Classification System Version 26.1 (effective 10/01.2008) Methodology Overview. 3M Health Information Systems. Wallingford, CT. 2008. Available at: http://www.hcup-us.ahrq. gov/db/nation/nis/v261_aprdrg_meth_ovrview.pdf. Accessed September 20, 2014. 12. Pfuntner A, Wier LM, Stocks C. Most Frequent Procedures Performed in U.S. Hospitals, 2010: Statistical Brief #149. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs [Internet]. Available at: http://www.ncbi.nlm.nih. gov/books/NBK132428/. Accessed November 8, 2015. 13. Lucas FL, Wennberg DE, Malenka DJ. Variation in the use of echocardiography. Eff Clin Pract 1999;2:71–5. 17. Yancy C, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology Foundation/ American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2013;62:1506–22. 18. Lopez-Jimenez F, Goraya TY, Hellermann JP, et al. Measurement of ejection fraction after myocardial infarction in the population. Chest 2004;125:397–403. 19. Hellermann JP, Jacobsen SJ, Redfield MM, Reeder GS, Weston SA, Roger VL. Heart failure after myocardial infarction: clinical presentation and survival. Eur J Heart Fail 2005;7: 119–25. 20. Santolucito PA, Tighe DA, Lessard D, et al. Changing trends in the evaluation of ejection fraction in patients hospitalized with acute myocardial infarction: the Worcester Heart Attack Study. Am Heart J 2008;155:485–93. KEY WORDS echocardiography, national trends A PP END IX For supplemental tables, please see the online version of this article. 511