Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Common cold wikipedia , lookup
Germ theory of disease wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Anti-nuclear antibody wikipedia , lookup
Globalization and disease wikipedia , lookup
Ebola virus disease wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Multiple sclerosis research wikipedia , lookup
Monoclonal antibody wikipedia , lookup
Autoimmune encephalitis wikipedia , lookup
Marburg virus disease wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
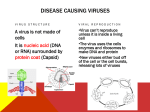
Rheumatology 2003;42:632–636 doi:10.1093/rheumatology/keg143, available online at www.rheumatology.oupjournals.org Advance Access publication 31 March 2003 The prevalence of antibodies against Sindbisrelated (Pogosta) virus in different parts of Finland M. Laine1,2, R. Vainionpää3, J. Oksi1,2, R. Luukkainen4 and A. Toivanen1 Objective. To study the occurrence of Sindbis-related (Pogosta) disease in Finland by serological means. Methods. A total of 2250 serum samples from five different areas were included in the study. Four hundred samples were collected from healthy blood donors and 1850 samples from patients who were suspected to have some viral infection. Antibodies of IgG and IgM classes against Pogosta virus were measured. Results. Eleven per cent of 2250 samples were positive for IgG and 0.6% were positive for IgM class antibodies against Pogosta virus. The antibody prevalence in Finland was almost equally distributed, being highest in western Finland (17%) and lowest in southern and northern Finland (9%). Of all samples with IgG class antibodies, 25% were taken from children under 10 yr of age. Conclusions. The prevalence of antibodies against Pogosta virus was much higher than we expected. Additionally, they were detected from all locations studied and not only in eastern Finland, which has been thought to be the main endemic area for this disease. Pogosta disease has been considered to affect mainly middle-aged persons, but our results indicate a high prevalence also among children. KEY WORDS: Pogosta virus, Sindbis-related virus, Finland. Pogosta disease, characterized by arthritis, rash and occasionally fever, was first recognized in the eastern parts of Finland in 1974 w1x. Since then there have been several outbreaks in the country and they seem to occur quite regularly every 7 years. A similar illness has been described in Sweden (Ockelbo disease) and in Russia (Karelian fever) w2, 3x. All three diseases are attributed to Sindbis-related arboviruses w4–6x. The virus causing Ockelbo disease has been isolated from pools of Culiseta, Aedes and Culex mosquitoes, and it is supposed that these late summer mosquitoes spread the Pogosta virus as well w6, 7x. The transmission cycles of arboviruses are complex w8x. Several factors, including viral, vector- and hostrelated, or environmental variations may contribute to its geographical variation w9x. Vertical transmission appears possible in the case of Ockelbo and Ross River viruses, which are close relatives to Pogosta virus w10–12x. These viruses are able to persist in the environment for a long period in desiccation-resistant mosquito eggs; therefore, a rapid onset of cases can occur if conditions become suitable w10–12x. In the case of Ross river virus, marsupials such as the western grey kangaroo, wallabies and euros (Macropus rotundus) are believed to be the major vertebrate hosts of the virus w13x. A recent study has demonstrated that migratory birds, mainly thrushes, on several continents have a high prevalence of antibodies against the mosquitoborne alphaviruses, and in Sweden almost all passerine species that were collected from forested wetlands and humid forests had antibodies against Sindbis virus w14x. Migratory birds may contribute to the spread of arthropod-borne infections in at least two ways. First, birds carrying infected ticks have been found to spread Borrelia burgdorferi efficiently over long distances w15x. Second, a latent borrelial infection may be reactivated during the migratory restlessness of the birds w16x. Departments of 1Medicine, 2Medical Microbiology and 3Virology, Turku University, Turku and 4Satalinna Hospital, Harjavalta, Finland. Submitted 24 January 2002; revised version accepted 4 September 2002. Correspondence to: A. Toivanen, Department of Medicine, Turku University, Kiinamyllynkatu 4–8, FIN-20520 Turku, Finland. E-mail: auli.toivanen@utu.fi 632 ß 2003 British Society for Rheumatology Antibodies against Pogosta virus in Finland 633 Many arthropod-borne diseases tend to occur in certain areas. Thus, Lyme disease caused by Borrelia burgdorferi is most common in the archipelago of southwestern Finland. Most cases of Ockelbo disease in Sweden have been reported to occur between the 60th and 64th parallels and Pogosta disease is thought to occur only in the eastern parts of Finland w1, 17x. We found a surprisingly high number of serologically confirmed cases of Pogosta disease also in south-western parts of Finland w18x. We also demonstrated that the disease does not have as good a prognosis as believed, but that the joint symptoms may persist for several years w18, 19x. It may, therefore, be suspected that Pogosta disease could be more common than thought at present, and that it should be considered a diagnostic alternative in patients with complaints of acute or chronic joint symptoms. In order to analyse the occurrence of this disease in Finland, we analysed samples collected from different geographical parts of the country for the presence of antibodies against Pogosta virus. Material and methods Serum specimens A total of 2250 serum samples from five different areas in Finland were analysed in this study. Of the samples, 1850 were selected to represent different parts of the country and were otherwise taken randomly from the Finnish Red Cross and the specimen libraries at the Department of Virology, University of Turku and Department of Medical Microbiology, University of Oulu. Therefore, various age groups were included and this led, by chance, to inclusion of sera obtained from very young individuals. Altogether, of these 1850 samples, 570 were from southern (Turku and Salo), 491 from eastern (Joensuu and Kuopio), 335 from western (Pori) and 454 from northern Finland (Oulu). These sera were mainly from hospitalized patients, and 90 samples were from patients who had visited health centres and were suspected to have some viral infection. The samples had been sent for serological analysis for the possible presence of antibodies against Mycoplasma pneumoniae, Chlamydia pneumoniae or Chlamydia trachomatis. There were also a few samples sent for testing of cytomegalovirus (CMV), herpes simplex (HSV), varicella zoster (VZV), enterovirus, Epstein–Barr virus, herpes virus 6 and parvovirus. Seventy-three samples were sent for testing of Pogosta virus antibodies and four of them gave positive results of Pogosta virus serology. Four hundred sera included in the study were from healthy blood donors in five cities: Kokkola (50), Joensuu (50), Rovaniemi (100), Turku (100) and Maarianhamina in the Åland Islands (100). The location of these cities is illustrated in Fig. 1. Blood donation in Finland is organized by the Finnish Red Cross. It is voluntary and strictly controlled, and blood donors must be considered healthy and socially active. All sera were stored at 2208C until tested for antibodies. Antibody determination Serum antibodies of IgG and IgM classes against Pogosta (Sindbis) virus were detected by an enzyme immunoassay method w4x. Briefly, the microtitre wells were coated with semipurified Sindbis virus antigen (strain 339). Serum dilutions FIG. 1. Map illustrating the endemic areas of Pogosta and Ockelbo diseases and Karelian fever. The cities from which samples were obtained are marked. (1:40–1:2560) were added to the wells and incubated for 2 h at 378C, after which horseradish peroxidase (HRP)-conjugated anti-human IgG or IgM antibodies at dilutions of 1:12 000 and 1:3000 (DAKO, Germany) were added. Orthophenylenediamine (OPD) was used as a colour substrate and the optical density (OD) was measured at 492 mm by a Multiskan Analyzer (Eflab OY, Helsinki, Finland). The last dilution, which gave an OD value higher than 2.5 times the OD value of negative controls, was considered positive. The sera positive for IgM were tested for rheumatoid factor (RF) by latex agglutination (RapiTex1RF, Dade Behring Marburg GmbH, Germany). If the test was found to be positive, RF was removed by absorption (GullSORB2, Gull Laboratories, Inc., SLC, UT,USA) and the antibody titre was retested. Results Altogether 2250 serum samples collected from two different sources were included in this study. The patient material was chosen not only to represent typical highrisk areas but also those thought to be at low risk of Pogosta disease. These 1850 sera were from people who had visited health centres or had been hospitalized, and in whom a viral disease was suspected. Their ages varied from 2 days to 100 yr with a mean of 35 yr; 54% of them were female and 46% male. Thirty-two per cent of the 1850 samples (594) came from persons under 20 yr (Fig. 2), and 37 samples were from infants under 1 yr. From the 400 healthy blood donors there was only general information available. In general, blood donors in Finland are healthy adults aged from 18 to 65; 51% of them are female and 49% male. We tested for IgG class antibodies against Pogosta virus from all 2250 serum samples. Eleven per cent (248) of these samples were positive for IgG class antibodies. The distribution of Pogosta cases in different parts of Finland is shown separately from the two serum donor 634 M. Laine et al. groups in Table 1 and together in Table 2. There were significant differences (P=0.002) in proportions of IgG class antibodies in different geographical areas. However, when western Finland was excluded from the analysis, the differences were not any more significant (P=0.465) (Table 2). The exact P values calculated to test the differences between the clinical and blood donor samples at each geographical location have been shown in Table 1. All IgG positive serum samples were tested for IgM class antibodies and only 20 were found to be positive. Five of them were positive for RF and they all turned out negative after retesting. Thus, after removing the RF by absorption, 15 sera were positive for Pogosta virus antibodies of IgM class. The prevalence of antibodies against Pogosta virus among the 1850 persons who were suspected to have some viral infection was highest in western Finland 15% (51) and lowest in northern Finland 6% (26). In eastern Finland 50 out of 491 samples (10%) were positive (Joensuu 12%, Kuopio 9%) and in southern Finland 43 out of 570 patients (8%) (Turku 10%, Salo 5%) had antibodies against Pogosta virus. Sera from persons aged below 10 yr were positive in 19% of cases and all sera from infants less than 1 yr old were negative. The results from the 400 samples from healthy blood donors were slightly different. The prevalence of IgG class antibodies was almost equally distributed in western (n=13, 26%), eastern (12, 24%) and in northern Finland (24, 24%). In the archipelago of Finland 11 out of 100 patients (11%) had IgG class antibodies and in southern Finland (Turku) 18 (18%) samples were positive. As a control we screened the result files of the Department of Virology, University of Turku to see which antibodies had been detected. The data of 1396 samples out of the 1850 which were included in the present study were available for this. These results are based on the tests carried out upon the request of clinicians, according to the clinical picture. Thirteen samples out of 764 tested had IgM antibodies against Chlamydia pneumoniae and 32 out of 354 tested against Mycoplasma pneumoniae. Four of them also had antibodies of IgG class against Pogosta virus. Also, 14 out of 179 tested TABLE 1. Comparison of IgG class antibodies against Pogosta virus in 1850 clinical samples and in 400 samples from blood donors collected by the Finnish Red Cross in different geographical areas in Finland Geographical area Eastern Finland Clinical samples Blood donors Western Finland Clinical samples Blood donors Southern Finland Clinical samples Blood donors Northern Finland Clinical samples Blood donors The Åland Islands Total Number of samples IgGa n (%) P valueb 491 50 50 (10) 12 (24) 0.007 335 50 51 (15) 13 (26) 0.067 570 100 43 (8) 18 (18) 0.002 454 100 100 2250 26 11 11 248 (6) (11) (11) (11) <0.001 a Positive for antibodies of IgG class. Exact P values were calculated to test differences between the clinical and blood donor samples at each location by x2-test. b TABLE 2. Numbers and percentages of sera with antibodies against Pogosta virus in all 2250 samples studied Geographical area Eastern Finland Western Finland Southern Finland Northern Finland The Åland Islands Total a Number of samples 541 385 670 554 100 2250 IgGa (%) IgMb (%) 11 17 9 9 11 11 2 1 0.4 0 0 0.6 Positive for antibodies of IgG class. Positive for antibodies of IgM class. b patients had IgM antibodies against Epstein–Barr virus, five out of 123 tested against parvovirus, two out of 38 tested against puumalavirus, three out of 227 tested against cytomegalovirus and one out of 224 tested against herpes simplex virus. None of these sera was positive for Pogosta virus. The age and sex distribution of the patients is shown in Figs 2 and 3. Discussion FIG. 2. Age and sex distribution of 1850 persons with antibodies against Pogosta virus. When we analysed the results of this study we found a few surprises. First of all, the percentage of sera positive for Pogosta virus was much higher than we expected. Second, more of the positive samples were from other parts of Finland than from eastern Finland, which is considered the main endemic area for this disease. Third, we were surprised by the high antibody prevalence among children. The critical question is whether the antibodies detected are truly against Pogosta virus or whether they are due to cross-reactivity against some other viruses. It is known that Epstein–Barr virus is a strong polyclonal activator and can cause cross-reactivity with other viruses. Still, only five out of 123 samples tested for Epstein–Barr Antibodies against Pogosta virus in Finland samples were positive and none of them was positive for Pogosta virus. There are no other known arboviruses belonging to the genus alphaviruses in Finland that cause diseases. Therefore cross-reactivity is very unlikely. We also screened the result files of 1396 samples to look for possible cross-reactivity against other viruses and bacteria (collected from the Department of Virology of Turku University). Only four samples positive for Pogosta virus IgG antibodies had antibodies against other micro-organisms. Thus, we consider the results reliable. The most common symptoms of Pogosta disease are arthralgia and polyarthritis, occurring in 93%, and rash in 88% of the patients w20x. In children joint symptoms are rare but rash is usually visible w20x. In this study 33% of positive IgG antibody tests for Pogosta virus were samples from patients younger than 20 yr. Thus, we found Pogosta disease to be common in children, which was quite striking because Pogosta disease is considered to be an illness of middle-aged patients w1, 21x. In infants aged less than 1 yr, antibodies were not detected and therefore those observed in the older children cannot be considered maternally derived. It might be that the infection in children is mild or even asymptomatic, and therefore until now neglected. Sindbis-related viruses seem to affect patients’ lives after infection and they should be considered as a differential diagnosis by doctors handling patients with chronic symptoms. It is well established that Pogosta and Ockelbo diseases can lead to chronic joint symptoms 635 lasting up to 4 yr w22x. The joint symptoms in Ockelbo disease have been reported to cause absence from work for up to 10 weeks (mean 3 weeks), being a true economic problem w23x. In an earlier study we found that 50% of patients still suffered from chronic joint and muscle pains 2.5 yr after Pogosta disease. After Ross River virus infection, chronic musculoskeletal symptoms have been reported w24x. The present study was carried out to examine the prevalence of antibodies against Pogosta virus in different parts of Finland. The serum samples were collected from 400 healthy blood donors and 1850 patients who were suspected to have a viral infection. All the clinical samples were collected in 2000, but the samples from blood donors were received in 1994. The fact that the two sets of samples were collected at different times can hardly explain the differences observed. The majority of Pogosta disease cases occur in August and September and for unknown reasons, at least in eastern Finland, the disease has been thought to have a tendency to cause outbreaks every 7 yr w1x. The reason for this variation is not known. Between the years 1989 and 2000 only one outbreak of Pogosta disease occurred. In the study conducted in 1989 by Kroneld et al. w25x, the prevalence of antibodies against Pogosta virus was 4.7% in southern Finland (Turku), 5.7% in central Finland (Jyväskylä) and 2.7% in the island of Iniö in the Finnish archipelago. Compared with these results, the antibody prevalence in our study FIG. 3. Age distribution of: (A) 335 persons with antibodies against Pogosta virus in western Finland, (B) 454 persons with antibodies against Pogosta virus in northern Finland, (C) 491 persons with antibodies against Pogosta virus in eastern Finland, (D) 570 persons with antibodies against Pogosta virus in southern Finland. 636 M. Laine et al. was higher, being 9% in southern Finland and 11% in the archipelago. This could be explained by the fact that in 1995 there was an outbreak of Pogosta disease and after that cases have been seen in southern Finland yearly (National Public Health Institute report). The epidemiology of Pogosta disease may be changing to occur not every 7 yr, but possibly every year, at least in southern Finland. Furthermore, in this study only a few patients (0.6%) had IgM antibodies against Pogosta virus, which indicates that 1994 and 2000 were inter-epidemic years. Formerly, Pogosta disease was considered to be endemic only in the eastern parts of Finland. Yet, in the light of these new results, Pogosta disease is quite common at all the locations studied. Acknowledgements We warmly thank the Department of Medical Microbiology, University of Oulu and Finnish Red Cross for providing serum samples for this study. This study was financially supported by the Scandinavian Rheumatology Research Foundation, Finnish Rheumatology Research Foundation, Turku Duodecim Foundation and the EVO Foundation of the Turku University Central Hospital. References 1. Brummer-Korvenkontio M, Kuusisto P. Onko Suomen länsiosa säästynyt ‘Pogostalta’? (Has Western Finland been spared the ‘Pogosta’?). Suom Lääkäril 1981; 32:2606–7. 2. Skogh M, Espmark Å. Ockelbo-sjukan—ett hud-och ledsyndrom troligen orsakat av myggburet alfa-arbovirus. Läkartid 1982;79:2379–80. 3. Lvov DK, Skvortsova TM, Kondrashina NG et al. Etiology of Karelian fever, a new arbovirus infection. Vopr Virusol 1982;6:690–2. 4. Calisher CH, Meurman O, Brummer-Korvenkontio M, Halonen PE, Muth DJ. Sensitive enzyme immunoassay for detecting immunoglobulin M antibodies to Sindbis virus and further evidence that Pogosta disease is caused by a Western Equine Encephalitis Complex virus. J Clin Microbiol 1985;22:566–71. 5. Calisher CH, Shope RE, Brandt W et al. Proposed antigenic classification of registered arboviruses I. Togaviridae, Alphavirus. Intervirology 1980;14:229–32. 6. Lundström JO, Vene S, Saluzzo J-F, Niklasson B. Antigenic comparison of Ockelbo virus isolates from Sweden and Russia with Sindbis virus isolates from Europe, Africa, and Australia: further evidence for variation among Alphaviruses. Am J Trop Med Hyg 1993;49:531–7. 7. Shirako Y, Niklasson B, Dalrymple JM, Strauss EG, Strauss JH. Structure of the Ockelbo virus genome and its relationship to other Sindbis viruses. Virology 1991; 182:753–64. 8. Kay BH, Aaskov JG. Ross River virus disease (epidemic polyarthritis). In: Monath TP, ed. The arboviruses: 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. epidemiology and ecology. Boca Raton FL:CRC Press, 1988:93–112. Tong S, Bi P, Hayes J, Donald K, Mackenzie J. Geographic variation of notified Ross River virus infections in Queensland, Australia, 1985–1996. Am J Trop Med Hyg 2001;65:171–6. Lindsay MDA, Broom AK, Wright AE, Johansen CA, Mackenzie JS. Ross river virus isolations from mosquitoes in arid regions of Western Australia: implication of vertical transmission as a means of persistence of the virus. Am J Trop Med Hyg 1993;49:686–96. Dhileepan K, Azuolas JK, Gibson CA. Evidence of vertical transmission of Ross river and Sindbis viruses (Togaviridae: Alphavirus) by mosquitoes (Diptera: Culicidae) in Southeastern Australia. J Med Entomol 1996;33:180–2. Francy DB, Jaenson TGT, Lundström JO et al. Ecologic studies of mosquitoes and birds as hosts of Ockelbo virus in Sweden and isolation of Inkoo and Batai viruses from mosquitoes. Am J Trop Med Hyg 1989;41:355–63. Mackenzie JS, Lindsay MD, Coelen RJ, Broom AK, Hall RA, Smith DW. Arboviruses causing human disease in the Australasian zoogeographic region. Arch Virol 1994;136:447–67. Lundström JO, Lindström KM, Olsen B, Dufva R, Krakower DS. Prevalence of Sindbis virus neutralizing antibodies among Swedish passerines indicates that thrushes are the main amplifying hosts. J Med Entomol 2001;38:289–97. Olsén B, Jaenson TGT, Noppa L, Bunikis J, Bergström S. A Lyme borreliosis cycle in seabirds and Ixodes uriae ticks. Nature 1993;362:340–2. Gylfe A, Bergström S, Lundström J, Olsen B. Reactivation of Borrelia infection in birds. Nature 2000;403:724–5. Espmark Å, Niklasson B. Ockelbo disease in Sweden: Epidemiological, clinical, and virological data from the 1982 outbreak. Am J Trop Med Hyg 1984;33:1203–11. Laine M, Luukkainen R, Jalava J, Ilonen J, Kuusisto P, Toivanen A. Prolonged arthritis associated with Sindbisrelated (Pogosta) virus infection. Rheumatology 2000; 39:1272–4. Luukkainen R, Laine M, Nirhamo J. Chronic arthritis after Sindbis-related (Pogosta) virus infection. Scand J Rheumatol 2000;29:399–400. Turunen M, Kuusisto P, Uggeldahl P-E, Toivanen A. Pogosta disease: clinical observations during an outbreak in the province of North Karelia, Finland. Br J Rheum 1998;37:1177–80. Lundström JO, Vene S, Espmark Å, Engvall M, Niklasson B. Geographical and temporal distribution of Ockelbo disease in Sweden. Epidemiol Infect 1991;106:567–74. Niklasson B, Espmark Å. Ockelbo disease: arthralgia 3–4 years after infection with a Sindbis virus related agent. Lancet 1986;i:1039–40. Vene S, Franzén C, Niklasson B. Development of specific antibody patterns and clinical symptoms following Ockelbo virus infection. Arch Virol 1994;134:61–71. Selden SM, Cameron AS. Changing epidemiology of Ross river virus disease in South Australia. Med J Aust 1996;165:313–7. Kroneld R, Meurman O, Forsén K-O, Lassenius R. The prevalence of antibodies against viruses causing Kumlinge and Pogosta diseases on the islands of Iniö on the Southwest coast of Finland. Scand J Infect Dis 1989;21:9–13.