Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Prescription costs wikipedia , lookup
Pharmacognosy wikipedia , lookup
Drug discovery wikipedia , lookup
Drug design wikipedia , lookup
Drug interaction wikipedia , lookup
Intravenous therapy wikipedia , lookup
Neuropharmacology wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Blood–brain barrier wikipedia , lookup
List of comic book drugs wikipedia , lookup
Theralizumab wikipedia , lookup
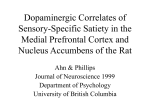
0022-3565/02/3013-1003–1011$7.00 THE JOURNAL OF PHARMACOLOGY AND EXPERIMENTAL THERAPEUTICS Copyright © 2002 by The American Society for Pharmacology and Experimental Therapeutics JPET 301:1003–1011, 2002 Vol. 301, No. 3 0/986121 Printed in U.S.A. Zidovudine Concentration in Brain Extracellular Fluid Measured by Microdialysis: Steady-State and Transient Results in Rhesus Monkey ELIZABETH FOX, PETER M. BUNGAY, JOHN BACHER, CYNTHIA L. MCCULLY, ROBERT L. DEDRICK, and FRANK M. BALIS Pharmacology and Experimental Therapeutics Section, Pediatric Oncology Branch, Center for Cancer Research, National Cancer Institute (E.F., C.L.M., F.M.B.); Drug Delivery and Kinetics Resource, Division of Bioengineering and Physical Science (P.M.B., R.L.D.); and Surgery Service, Veterinary Resources Program, Office of Research Services, National Institutes of Health, Bethesda, Maryland (J.B.) Received January 9, 2002; accepted February 11, 2002 This article is available online at http://jpet.aspetjournals.org ratio) and CSF penetration (standard sampling CSF/serum ratio) at steady state were 0.13 ⫾ 0.06 and 0.17 ⫾ 0.02, respectively. With bolus dosing the mean (⫾S.D.) zidovudine area under concentration-time curve (AUC) normalized to a dose of 80 mg/kg was 577 ⫾ 103 M 䡠 h in blood, 528 ⫾ 202 M 䡠 h in muscle, and 108 ⫾ 74 M 䡠 h in brain (brain/blood ratio of 0.18 ⫾ 0.10) by microdialysis. Serum ultrafiltrate AUC was 446 ⫾ 72 M 䡠 h and the CSF AUC was 123 ⫾ 4.7 M 䡠 h (CSF/serum ratio of 0.28 ⫾ 0.06). In conclusion, recovery was tissue-dependent. CSF and brain ECF zidovudine concentrations were comparable at steady state, and the corresponding AUCs were comparable after bolus injection. Thus, zidovudine penetration in brain ECF and CSF in nonhuman primates is limited to a similar extent, presumably by active transport, as in other species. The intensity of a drug’s pharmacological effect is determined, in part, by the free drug concentration at the effect site in tissues. Pharmacokinetic compartmental modeling may be used to simulate drug concentration in a peripheral compartment. This compartment does not correspond to a particular anatomical space. Its concentration represents appropriately averaged concentrations in all of the tissues contributing to the compartment and may not reflect the concentration in the target tissue(s). For zidovudine in the monkey, the peripheral compartment is expected to be dominated by muscle. Measuring tissue drug concentration directly by biopsy can only provide data at discrete time points and represents total drug concentration in tissue and blood perfusing the tissue. Microdialysis is a minimally invasive tissue sampling technique that can be used for continuous in vivo monitoring of free drug concentration in tissue extracellular fluid (ECF) (Muller et al., 1995; Elmquist and Sawchuk, 1997; Johansen et al., 1997; Davies, 1999). The microdialysis probe (Fig. 1), which is inserted into tissue, has a semipermeable dialysis membrane at its tip. A solution (perfusate), such as Ringer’s lactate, is continuously infused into the probe and collected from the outflow tube (dialysate). Drug sampling by microdialysis relies on diffusion of drug across the probe membrane driven by the difference in free concentration between the ECF and the dialysate flowing along the inside surface of the membrane. Transit time of the dialysate from the inlet to outlet ends of the membrane is typically too brief to permit equilibration with surrounding tissue. Thus, the drug concentration ([drug]) in the effluent dialysate is related to the [drug] in the ECF, but the concentrations are generally significantly different (Benveniste and Huttemeier, 1990; Bungay et al., 1990; Morrison et al., 1991). The relationship between ECF [drug] and [drug] in the effluent dialysate is expressed by the recovery or extraction fraction. Accurate estimation of recovery is critical to quan- ABBREVIATIONS: ECF, extracellular fluid; [drug], drug concentration; MWCO, molecular weight cutoff; BBB, blood-brain barrier; CSF, cerebrospinal fluid; HPLC, high-performance liquid chromatography; AUC, area under concentration-time curve. 1003 Downloaded from jpet.aspetjournals.org at ASPET Journals on June 18, 2017 ABSTRACT We measured zidovudine concentrations in blood, muscle, and brain extracellular fluid (ECF) by microdialysis and in serum ultrafiltrate and cerebrospinal fluid (CSF) samples during a continuous intravenous infusion (15 mg/kg/h) and after bolus dosing (50 – 80 mg/kg over 15 min) in nonhuman primates to determine whether CSF drug penetration is a valid surrogate for blood-brain barrier penetration. Recovery was estimated in vivo by zero net flux for the continuous infusion and retrodialysis for the bolus dosing. In vivo recovery was tissue-dependent and was lower in brain than in blood or muscle. Mean (⫾S.D.) steady-state blood, muscle, and brain zidovudine concentrations by microdialysis were 112 ⫾ 63.8, 105 ⫾ 51.1, and 13.8 ⫾ 10.4 M, respectively; and steady-state serum ultrafiltrate and CSF concentrations were 81.2 ⫾ 40.2 and 14.1 ⫾ 8.0 M, respectively. Brain ECF penetration (microdialysis brain/blood 1004 Fox et al. under steady-state and nonsteady-state conditions. Brain ECF concentrations were compared with CSF and muscle ECF zidovudine concentrations. To assess the accuracy of the microdialysis sampling technique, free zidovudine concentrations were also measured in blood simultaneously by microdialysis and conventional serum sampling followed by ultrafiltration of the serum sample. Materials and Methods Fig. 1. Schematic of a microdialysis probe with an inflow tube through which a physiological solution is continuously perfused, a semipermeable dialysis membrane, and an outflow tube from which the dialysate is collected. The dimensions of the membrane for the probes used in this study are 0.5 mm in diameter by 10 mm in length (surface area 15.7 mm2). Downloaded from jpet.aspetjournals.org at ASPET Journals on June 18, 2017 tifying tissue ECF [drug] (Morrison et al., 1991). Several methods have been developed to estimate microdialysis probe recovery. With the zero net flux method, the concentration of drug added to the perfusate is varied, and the change in [drug] is measured in the outflow dialysate. The inflow perfusate [drug] and outflow dialysate [drug] are presumed to be equal if there is no net exchange of drug between the tissue ECF and the perfusate in the probe (i.e., the perfusate [drug] ⫽ tissue ECF [drug]) (Lonnroth et al., 1987). In the retrodialysis method, drug is added to the perfusate before administration of drug to the subject. The fractional loss to the drug-free tissue ECF is assumed equivalent to the recovery of drug from tissue ECF into a drug-free perfusate after drug is administered to the subject (Wang et al., 1993). Microdialysis probe membrane properties, perfusate flow rate, physicochemical properties of the drug, and tissue factors determine recovery (Bungay et al., 1990; Stenken, 1999). Larger microdialysis membrane surface provides greater area for diffusion and enhanced recovery. The molecular weight cutoff (MWCO), composition, and surface charge of the dialysis membrane can also affect recovery (Hsiao et al., 1990; Zhao et al., 1995). A higher flow rate shortens the perfusate transit time and therefore decreases the difference in the concentration of drug between the inflow and outflow. Thus, recovery is inversely related to the perfusate flow rate. Molecular weight, charge, shape, and protein binding of a drug will influence recovery. Microdialysis membrane surface area, composition, and MWCO can be selected to accommodate the drug, and a flow rate can be chosen for optimal recovery. However, tissue factors that contribute to the resistance to drug diffusion, including cellularity, cellular uptake, drug catabolism, blood flow, and the ECF structure, vary among tissue types and have substantial impact on recovery. Therefore, to accurately quantify tissue ECF [drug] using microdialysis, recovery for the microdialysis probe must be measured in each tissue in vivo. Quantifying brain ECF [drug] is of particular interest because of the presence of the blood-brain barrier (BBB), which limits access of many drugs to the brain. Although drug penetration into cerebrospinal fluid (CSF) is frequently used as a surrogate for BBB penetration, the BBB and blood-CSF barrier differ in their anatomical location and function. We evaluated microdialysis as a sampling technique to study brain ECF zidovudine concentrations in nonhuman primates Animals. Adult male rhesus monkeys (Macaca mulatta), ranging in weight from 8.3 to 12.8 kg, were fed Purina Monkey Chow (Purina, St. Louis, MO) twice daily and were group housed in accordance with the Guide for the Care and Use of Laboratory Animals (National Research Council, 1996). This study was approved by the National Cancer Institute Institutional Animal Care and Use Committee. Drug Formulation and Administration. Zidovudine for intravenous infusion (GlaxoSmithKline, Uxbridge, Middlesex, UK; 10 mg/ml; molecular mass, 267 Da) was diluted with 5% dextrose to a final concentration of 4 mg/ml and infused i.v. For steady-state experiments (animals B9078, 15398, H127, D28, and H351), a 5-mg/kg loading dose was administered as an i.v. bolus, followed by a 15-mg/kg/h continuous i.v. infusion. Before conducting microdialysis sampling, this infusion schedule was administered to two animals (B9884 and B9078) and standard serum and CSF sampling was performed during the infusion to determine when steady-state concentrations are achieved in serum and CSF. For bolus experiments (animals 85Z, H090, and 9SL), 50 to 80 mg/kg was administered intravenously over 15 min. Zidovudine was infused through surgically implanted access ports that were attached to catheters in the jugular vein or through temporary peripheral intravenous catheters that were inserted before the experiment. Infusion rates were controlled with an AIM infusion pump (Abbott Laboratories, North Chicago, IL). Conventional Blood, CSF, and Tissue Samples. For serum sampling, catheters were surgically placed into the saphenous or femoral vein and attached to a subcutaneously implanted access port (vascular access port; Access Technology, Skokie IL). On the day of the microdialysis procedure, animals without vascular access ports had a peripheral intravenous catheter inserted into a vein distant from the site of zidovudine infusion. Blood samples were collected into serum separator tubes (BD Biosciences, Rutherford, NJ). After clot formation, serum was separated by centrifugation (1000g for 15 min) and stored at ⫺70°C. Before analysis, serum ultrafiltrate, which contained nonprotein-bound zidovudine, was prepared using Microcon centrifugal filter devices with MWCO 10,000 Da (Amicon YM-10; Millipore, Bedford, MA). Zidovudine protein binding in serum was 10 to 13%, similar to results published previously in rhesus monkeys (Collins et al., 1988). For CSF sampling, four animals (B9884, B9078, 15398, and 85Z) had silicone Pudenz catheters surgically placed into the fourth ventricle and attached to a subcutaneously implanted Ommaya reservoir, as described previously (McCully et al., 1990). Lumbar CSF samples were obtained from temporary lumbar catheters in three animals (H127, D28, and H351). Cerebrospinal fluid was sampled from the subarachnoid space in two animals (H090 and 9SL) (Bacher et al., 1994). All CSF samples were stored at ⫺70°C before analysis. Six excisional muscle biopsies (0.77–2.57 g) were obtained from the right hind limb of 85Z after a bolus dose of zidovudine. Muscle biopsies were obtained before drug administration and at 0.25 (end of infusion), 1.25, 2.27, 3.27, and 4.3 h after administration of the zidovudine bolus. Excess blood was blotted from the specimens and they were immediately frozen on dry ice. Specimens were stored at ⫺70°C until processed and analyzed. Before high-performance liquid chromatography (HPLC) analysis, samples were thawed and homogenized using a glass Dounce and centrifuged at 1000g for 15 min at Zidovudine Tissue and Brain Penetration by Microdialysis lactated Ringers) maintained at 38°C. This solution represents the in vitro ECF. The brain microdialysis probe was sequentially perfused with 0, 1, 5, 10, and 25 M [14C]zidovudine (Moravek, specific activity 55 mCi/mmol) and the in vitro ECF contained 5 M [14C]zidovudine in Elliott’s B solution. Muscle and blood microdialysis perfusates contained 0 to 100 M [14C]zidovudine and 20 M [14C]zidovudine in lactated Ringers solution as the ECF. For the bolus zidovudine experiments, retrodialysis (Wang et al., 1993) was used to estimate recovery. The perfusate flow rate was 0.5 l/min and the probe membrane length was 10 mm. In vivo retrodialysis was performed before administration of the drug as a single 30-min collection after an equilibration period of at least 20 min. The retrodialysis perfusate contained 20 M zidovudine. The zidovudine concentration was measured in the perfusate ([perfusate]) and the dialysate from the outflow tube ([dialysate]). Recovery was calculated from the following equation: Recovery ⫽ 关 perfusate兴 ⫺ 关dialysate兴 关 perfusate兴 After completion of the retrodialysis collection, each microdialysis probe was equilibrated with drug-free solution (Elliott’s B solution for the brain probe and lactated Ringer’s solution for the muscle and blood probes). For monkey 85Z (bolus experiment), a single microdialysis sample was collected over the 4.3-h sampling period. For monkeys H090 and 9SL, microdialysis samples were obtained at hourly intervals (30 l) starting with the initiation of the 15-min bolus infusion and continuing for 4 h. Microdialysis samples were stored at ⫺70°C until analyzed. Tissue ECF zidovudine concentration was calculated by dividing the measured dialysate concentration by the retrodialysis-determined recovery. Serum and CSF samples were collected at the midpoint of each microdialysis collection period. As with the zero net flux method, the in vivo estimates of recovery by retrodialysis were used to calculate tissue ECF drug concentration. For in vitro retrodialysis with the brain microdialysis probe, the perfusate contained 5 M [14C]zidovudine, and well stirred Elliott’s B at 38°C was the in vitro ECF. The muscle and blood probes were perfused with 20 M [14C]zidovudine, and well stirred lactated Ringer’s solution at 38°C was the in vitro ECF. Radioactivity in the perfusate and dialysates was measured using a liquid scintillation counter (model LS 3801; Beckman Coulter, Inc., Fullerton, CA). Zidovudine Assay. Serum and CSF zidovudine concentrations were measured by a commercially available enzyme-linked immunosorbent assay method (Sigma-Aldrich, St. Louis, MO) for samples from the preliminary zidovudine infusions conducted to establish the time required to achieve steady state with the loading dose and continuous infusion schedule. All other samples were assayed with a previously reported reverse phase HPLC method (Klecker et al., 1987), which was modified to accommodate the reduced volume of microdialysis samples. All serum and muscle biopsy samples were ultrafiltered as described above. CSF and microdialysis samples were not filtered or extracted. All samples were analyzed in triplicate. The HPLC system consisted of a Spheri-5 RP-18, 5 M, 30- ⫻ 2.1-mm guard column (Brownlee Columns, PerkinElmer Instruments, Norwalk, CT) coupled with a Nova Pak C18, 60 Å, 4 m, 2- ⫻ 150-mm analytical column (Waters, Milford, MA) and a Waters model 2690 separations module. The mobile phase consisted of 90% 10 mM sodium acetate, pH 6.55, and 10% acetonitrile. Elution of zidovudine was achieved with isocratic flow at 0.5 ml/min. Analysis cycle time was 15 min. Eluant was monitored with a Waters 996 photo diode array detector at 267 nm. The retention time of zidovudine was approximately 4.5 min. The major metabolite of zidovudine, 3⬘azido-3⬘-deoxythymidine--D-glucuronide, had a retention time of approximately 1 min. The lower limit of detection was 0.1 M and the lower limit of quantification was 0.25 M. The intraday coefficient of variation was ⬍8% for 0.5 M, ⬍2% for 10 M, and ⬍1% for 100 M. The interday Downloaded from jpet.aspetjournals.org at ASPET Journals on June 18, 2017 4°C. Using 500-l aliquots of the supernatant, ultrafiltrates were prepared as described for serum specimens. Microdialysis Equipment. CMA 102 microdialysis dual syringe pumps, Exmire 2.5-ml gastight syringes, CMA 20 vascular microdialysis probes (10- ⫻ 0.5-mm polycarbonate membrane MWCO 20,000; shaft length, 14 mm) with peel away split introducers, CMA 110 manual liquid switch, FEP tubing (1.2 l/100 mm) and tubing adapters, and CMA 130 in vitro stand and probe clips were obtained from CMA/Microdialysis (North Chelmsford, MA). Equipment and probes were ethylene oxide gas-sterilized before use. Surgical Procedure. Anesthesia was maintained by inhalation of isoflurane (1 to 2%) and oxygen during the surgical and sampling procedures (approximately 6 h). Buprenorphine and ketoprofen were administered for analgesia. Intravenous hydration (normal saline 10 ml/kg/h) was maintained throughout the microdialysis procedure. Animals were positioned in ventral recumbency on the surgery table and their heads were placed in a stereotaxic unit (David Kopf Instruments, Tujunga, CA) using the eyebars and mouthpiece to position the head in a horizontal plane. The surgical area was clipped, scrubbed, and draped for aseptic surgery. A 4- to 5-cm midline incision was made over the frontal and anterior parietal bone. The periosteum was incised and retracted laterally along with the right temporalis muscle. Approximately 5 to 7 mm from the midline a 4-mm burr hole was created in the right temporal bone. A small dural incision permitted insertion of the microdialysis probe without damaging the probe membrane. The microdialysis probe was lowered into the cerebral cortex using the stereotaxic carrier. No guide probe was used. The top of the probe membrane was positioned 3 mm below the surface of the brain and extended 13 mm into the brain parenchyma. A second microdialysis probe was inserted into the left temporalis muscle by means of a peel away plastic introducer (CMA/ Microdialysis). The probe was sutured to the temporalis muscle to prevent movement during the sampling procedures. A third microdialysis probe was percutaneously placed either in the cephalic or saphenous vein using a peel away plastic introducer over a 19-gauge needle. This probe was also sutured in place. When sampling was complete all microdialysis probes were removed, and the animal was recovered from anesthesia. Buprenorphine and ketoprofen were administered for analgesia, dexamethasone was administered for 3 days, and gentamicin and penicillin G with procaine were administered for 7 days after the procedure. Microdialysis. For the continuous infusion experiments, the loading dose of zidovudine was administered and the infusion started before placement of the microdialysis probes in the brain, muscle, and blood to ensure that sampling was performed at steady state. To lessen the impact of the acute effects of probe insertion on tissue, microdialysis sampling began at least 20 min after probe insertion. Steady-state tissue ECF zidovudine concentration and recovery were determined using the zero net flux method (Wang et al., 1993) in vivo. In vitro recovery was also determined after completion of microdialysis sampling in the animal to verify probe membrane integrity. For all ZNF experiments the microdialysis probe perfusate flow rate was 1 l/min and the probe membrane length was 10 mm. The point of zero net flux was determined by sequentially perfusing four to five solutions with varying zidovudine concentrations into the microdialysis probe and measuring the zidovudine concentration in the outflow dialysate. With each perfusate zidovudine concentration, a 10-min equilibration period was followed by a collection time of 20 min (20 l of dialysate). Plotting the difference between the inflow perfusate zidovudine concentration and the outflow dialysate zidovudine concentration as a function of the perfusate concentration resulted in a line with the slope equal to the relative recovery and an x-intercept equal to the steady-state tissue ECF zidovudine concentration. The perfusate zidovudine concentrations ranged from 0 to 50 M for the brain probe and 0 to 500 M for muscle and venous blood probes. In vitro recovery was determined by submerging the probe into 10 ml of continuously stirred physiological solution (Elliott’s B or 1005 1006 Fox et al. Results Recovery. The recovery (Table 1) for each microdialysis probe was estimated in vivo by the zero net flux method during the continuous infusions or by the retrodialysis method before the bolus doses. In vitro recovery was estimated by the same method after the in vivo portion of the experiment was completed to assess the integrity of the dialysis membrane. Microdialysis probe membrane length was 10 mm in all experiments. Recovery measured in vivo was substantially lower than in vitro recovery in the same probe. In vivo recovery was also tissue-dependent (highest in blood and lowest in brain), and in vivo recovery was more variable (higher coefficient of variation) than in vitro recovery across experiments. In vivo recovery was less variable with the retrodialysis method using a lower probe perfusate flow rate (0.5 l/min). Steady-State Experiments. When administered as a loading dose (5 mg/kg) followed by a continuous infusion (15 mg/kg/h), steady-state zidovudine concentrations were achieved within 1 h in serum and by 2 h in the CSF (Fig. 2). Steady-state zidovudine concentrations in two animals were 52 and 63 M in serum and 5.3 and 4.6 M in CSF. In subsequent microdialysis experiments, sampling was initiated more than 2 h after the loading dose and start of the continuous infusion. The steady-state tissue zidovudine concentrations determined by microdialysis and using the zero net flux recovery method for each animal (n ⫽ 5) are presented in Table 2 along with the results from conventional serum ultrafiltrate and CSF sampling. Blood zidovudine concentration measured in microdialysis samples from a vein was higher than free drug concentrations in serum ultrafiltrates by a median of 39%. The mean steady-state serum ultrafiltrate zidovudine concentration was 81.2 M, and the mean steady-state blood zidovudine concentration from microdialysis samples was 112 M. The mean (⫾S.D.) free zidovudine clearance based on the steady-state serum concentrations was 0.80 ⫾ 0.28 l/h/kg. Steady-state zidovudine concentration in muscle (mean, 105 M) measured by microdialysis was equivalent to the microdialysis estimate of steady-state blood zidovudine concentration. Brain steady-state zidovudine concentration (mean, 13.8 M) from the microdialysis measurements was substantially lower than blood and muscle steady-state drug concentrations, indicating that the blood-brain barrier was functioning during the microdialysis collection period. Brain steady-state zidovudine concentrations from the microdialysis samples were similar to conventional CSF measurements (Table 2). In animal H127, the CSF zidovudine concentration and the CSF/serum ratio were substantially higher than in the other four animals and the two pilot animals in which the time to reach steady state was determined. Excluding animal H127, the mean brain steady-state zidovudine concentration (n ⫽ 4) was 14.3 M and the mean CSF steady-state zidovudine concentration was 14.1 M. The brain/blood ratio from the microdialysis measurements without animal H127 was 0.12 and the CSF/serum ultrafiltrate ratio was 0.17. Bolus Dose Experiments. The serum ultrafiltrate zidovudine concentrations were well described by the twocompartment model (Fig. 3). The fitted and derived pharma- TABLE 1 Comparison of microdialysis probe recovery measured in vivo and in vitro by the zero net flux method for the continuous zidovudine infusion studies and by the retrodialysis method for the bolus zidovudine studies The tissues (blood, muscle, and brain) represent the sites at which the probes were inserted for monitoring tissue drug concentrations in vivo. The length of the probe membrane was 10 mm. In vitro recovery was measured by the same method that was used in vivo, after completion of the in vivo experiments. The higher recoveries with the retrodialysis method are a reflection of the lower perfusate flow rate in the microdialysis probe. Recovery Method Flow Rate n Blood Muscle Brain in vitro in vivo in vitro in vivo in vitro in vivo 0.79 0.11 14 0.90 0.07 8 0.40 0.29 72 0.69 0.06 8 0.66 0.12 19 0.92 0.06 7 0.26 0.11 42 0.50 0.10 20 0.67a 0.06 9 0.90 0.05 6 0.15 0.07 46 0.29 0.10 32 l/min Zero net flux 1 5 Retrodialysis 0.5 3 Mean S.D. CV (%) Mean SD CV (%) CV, coefficient of variation. a n ⫽ 4, the outflow tube on one probe was damaged during probe removal from the brain after completion of the in vivo experiment. Downloaded from jpet.aspetjournals.org at ASPET Journals on June 18, 2017 coefficient of variation was 4, 2, and 5% for 0.5, 10, and 100 M, respectively. Pharmacokinetic Analysis. A two-compartment open model consisting of central and peripheral compartments with a first order elimination from the central compartment was fit to the serum concentration-time data from the individual bolus zidovudine experiments (85Z, H090, and 9SL). Four model parameters [Vc, volume of the central compartment; kcel, first order elimination rate constant; and kcp and kpc, first order exchange rate constants describing the movement of drug between the central (c) and peripheral (p) compartments] were estimated with a weighted (EWT function) fit using MLAB (Civilized Software, Bethesda, MD). Clearance, volume of distribution at steady state, and half-lives were derived from the model parameters. For the continuous infusion experiments, free drug clearance was calculated from the infusion rate divided by the serum ultrafiltrate steady-state concentration. Area under the concentration-time curves (AUCs) from 0 to 4 h for CSF, serum, and muscle biopsies were derived using the linear trapezoidal method (Rowland and Tozer, 1980; Gibaldi and Perrier, 1982). Microdialysis 0- to 4-h AUCs were calculated by summation of microdialysate zidovudine concentrations corrected for tissue-specific in vivo recovery and multiplied by the sampling interval. The fraction of zidovudine penetrating into the central nervous system was calculated from the ratio of steady-state CSF and serum zidovudine concentration or steady-state brain-to-blood concentrations for microdialysis sampling during the continuous zidovudine infusion. The central nervous system penetration after the bolus dose was calculated from the CSF AUC/serum AUC for conventional sampling or brain AUC/ blood AUC for microdialysis sampling. Zidovudine Tissue and Brain Penetration by Microdialysis cokinetic parameters for each animal are presented in Table 3. The blood zidovudine AUC based on the microdialysis measurements using the retrodialysis recovery method were 26 to 30% higher than the AUC calculated from the serum ultrafiltrate zidovudine concentrations (Table 4). The shape of the serum ultrafiltrate and microdialysis-determined blood zidovudine concentration-time curves were similar (Fig. 3, A, D, and G). As was observed for the concentrations from microdialysis in the steady-state experiments, the AUCs of zidovudine in muscle (mean, 528 M 䡠 h) from the microdialysis measurements were equivalent to microdialysis estimates of the AUC of zidovudine in blood (mean, 577 M 䡠 h). The results from microdialysis sampling from muscle were also compared with the simulated zidovudine concentrations and AUC in the peripheral compartment of the two-compartment model that was fit to the serum ultrafiltrate zidovudine concentrations (Fig. 3B). The mean AUC in the simulated peripheral (tissue) compartment was 474 M 䡠 h. Serial muscle biopsy specimens were obtained over 4 h in a single animal (85Z) after a bolus dose of zidovudine (80 mg/kg), and the AUC in muscle from these biopsy samples was 312 M 䡠 h compared with an AUC of 491 M 䡠 h based on the microdialysis sampling of muscle extracellular fluid. Brain ECF AUCs of zidovudine (mean, 108 M 䡠 h) from the microdialysis measurements were lower than blood and muscle AUCs, and similar to CSF AUC (mean, 123 M 䡠 h). The CSF penetration of zidovudine after a bolus dose (mean, 0.28) was similar to the value obtained at steady state (mean, 0.27) when all five animals are included but higher than the steady-state value with the outlier excluded (mean, 0.17). The brain ECF penetration based on microdialysis tissue sampling was similar at steady state (mean, 0.13) and after the bolus dose (mean, 0.18) and similar to the CSF penetration at steady state with the outlier excluded. Although the brain ECF and CSF penetration was similar based on the 0- to 4-h AUC values, there seem to have been differences in the concentration-time profiles during these transient experiments (Fig. 3, C, F, and I). The mean shape of the CSF profiles obtained by sampling from the subarachnoid space in two animals (H090 and 9SL) exhibited a rapid elevated peak. This contrasted with the broad time profile from the corresponding brain ECF mean profile from hourly microdialysis sampling in the same animals. A similar broad time profile was found in the ventricular CSF of the third animal (85Z). The difference between the subarachnoid and ventricular CSF results suggests a possible lack of equivalence in the transient response at these CSF sampling sites. Truncating the AUC after 4 h represents an approximation. As noted above, the zidovudine time profiles displayed in Fig. 3C for the CSF of animal 85Z and the ECF microdialysis of animals H090 and 9SL are relatively slow. As a consequence, these 0- to 4-h AUC values probably underestimate the complete zero to infinity AUC values to a greater degree than in the more rapidly responding blood, serum, and muscle compartments of Fig. 3. The corresponding ECF and CSF penetration values in Table 4 may likewise be somewhat underestimated. Toxicity. The microdialysis sampling was well tolerated. Animal D28, which received continuous infusion zidovudine, had a transient elevation in liver transaminases, elevated serum creatine kinase, and a single episode of hemoglobinuria after the procedure. These laboratory abnormalities were accompanied by anorexia and lassitude. These signs and symptoms were attributed to zidovudine and resolved with supportive care measures. Two animals that received bolus dosing of zidovudine were sacrificed. The euthanasia of 85Z (the animal from which the muscle biopsy specimens were obtained) was planned. H090 was euthanized 27 h after the completion of the microdialysis sampling period for multisystem organ failure. H090 recovered from anesthesia but had progressive deterioration in cardiac, respiratory, and renal function. At necropsy, a previously undiagnosed chronic cardiomyopathy was discovered. There was no evidence of hemorrhagic or ischemic changes at the site of microdialysis probe insertion in the brain. Both 85Z and H090 received 80-mg/kg i.v. bolus of zidovudine. The third animal in the bolus group (9SL) received 50 mg/kg i.v. zidovudine and tolerated the procedure well. Discussion Microdialysis is a minimally invasive sampling technique that can be used to continuously monitor drug concentrations in the ECF of tissues that are accessible to microdialysis probe placement. The free drug concentration at the site of drug action in tissues is a critical determinant of the intensity of the drug’s effect, and therefore monitoring tissue free drug concentration may be more informative than monitoring plasma drug concentrations. We compared microdialysis sampling from blood and tissues to conventional sampling methods in a nonhuman primate model at steady state during a continuous infusion of Downloaded from jpet.aspetjournals.org at ASPET Journals on June 18, 2017 Fig. 2. Serum and CSF zidovudine concentrations achieved with a 5-mg/kg loading dose, followed by a 15-mg/kg/h continuous infusion in two animals (A, animal B9884; B, animal B9078). Steady state is achieved in serum and CSF by 2 h. 1007 1008 Fox et al. TABLE 2 Steady-state zidovudine concentration in serum ultrafiltrate and CSF samples collected by conventional methods and in blood, muscle, and brain collected by microdialysis (D) during a continuous intravenous infusion of 15 mg/kg/h zidovudine Recovery was determined by the zero net flux method (Table 1). CSF/serum and brain/blood ratios represent the ratio of the steady state zidovudine concentrations at the designated sampling sites. Steady-State Zidovudine Concentration Animal Blood (D) Muscle (D) M M M 62.9 48.5 73.6 151 70.1 123 58.3 66.8 217 97.5 90.1 85.3 94.4 193 60.5 12.9 8.1 50.1 25.7 9.7 4.5 9.9 11.9 31.6 11 0.20 0.17 0.69 0.17 0.14 0.04 0.17 0.18 0.16 0.11 81.2 40.2 49.5 112 63.8 56.7 105 51.1 48.8 21.3a 17.5 82.3 13.8 10.4 56.7 0.27a 0.23 85.2 0.13 0.06 44 Serum B9078 15398 H127 D28 H351 Mean S.D. CV (%) CSF Brain (D) M M CSF/Serum Brain/Blood (D) CV, coefficient of variation. a Excluding the CSF and CSF/serum values for animal H127, which was an outlier (see text), the mean steady state CSF zidovudine concentration is 14.1 M and the CSF/serum ratio is 0.17. tion, is less time-consuming. The perfusion interval required to achieve steady state in retrodialysis varies with the tissue. Although recovery varies over time in nonsteady-state microdialysis, the steady-state recovery can be appropriately used to calculate AUC values for ECF from the dialysate measurements (Bungay et al., 2001). After bolus dosing, zidovudine concentrations in the blood measured by microdialysis paralleled the serum ultrafiltrate zidovudine concentrations, suggesting that cumulative microdialysis collections provide an estimate of drug exposure (AUC) under nonsteady-state conditions (Bungay et al., 2001). AUC or the average concentration (AUC/dosing interval) is the pharmacokinetic parameter that best correlates with drug effect for many drugs, including anticancer drugs (van den Bongard et al., 2000). Microdialysis samples from a vein and conventional serum samples were obtained simultaneously in both the steadystate and bolus experiments. Microdialysis measurements approximated the serum ultrafiltrate concentrations, but in eight of the nine experiments, the microdialysis estimate of steady-state blood concentration or AUC was higher than the serum ultrafiltrate measurement. Although this bias could be related to an underestimation of recovery, a similar degree of bias was observed with both methods used to estimate recovery. To accurately assess tissue drug penetration relative to blood levels of the drug, microdialysis measurements from the tissue should be compared with microdialysis measurements of blood rather than to conventional serum or plasma drug concentrations. Muscle ECF zidovudine steady-state concentration during the continuous infusion and the AUC in muscle after the bolus dose were measured by microdialysis and approximated the blood values. This excellent tissue penetration is consistent with the lipophilicity and low molecular weight of zidovudine. A two-compartment model was fit to the serum ultrafiltrate zidovudine concentration-time data after the bolus dose, and the zidovudine concentration profile for the peripheral (tissue) compartment was simulated from the model parameters. The shape of the peripheral compartment zidovudine concentration-time curve and the zidovudine AUC in this compartment were in agreement with the microdialysis measurements of muscle drug concentrations, indicating that the two-compartment model provides a reason- Downloaded from jpet.aspetjournals.org at ASPET Journals on June 18, 2017 zidovudine and after a bolus dose of zidovudine. The pharmacology of this nucleoside analog has been previously characterized in our animal model and the CSF penetration was 0.21 (Klecker et al., 1987; Collins et al., 1988; Balis et al., 1989). Zidovudine (mol. wt., 267) is well tolerated, lipophilic, and minimally protein bound, and a sensitive and specific assay for its detection and quantification had been developed (Klecker et al., 1987). The nonhuman primate model has also been highly predictive of human pharmacokinetics (Adamson et al., 1991; Blaney et al., 1995), and the size of the animals allowed us to use microdialysis probes with membrane dimensions that are potentially applicable to humans. For a drug with linear pharmacokinetics, the drug concentration in the dialysate that is collected from the microdialysis probe is proportional, but not equal to, the tissue ECF free drug concentration. The proportionality constant that relates dialysate drug concentration to the tissue ECF drug concentration is recovery. If the recovery is not accurately determined then the tissue ECF concentration will be inaccurate. Our experience indicates that recovery is tissue-specific and should be determined in vivo in each tissue that is being monitored. Measuring recovery with the same probe in vitro overestimated recovery and would therefore underestimate the tissue ECF drug concentration. The primary factor limiting diffusion of drug into the probe in vitro is the resistance to diffusion of the semipermeable membrane, whereas tissue resistance to drug diffusion is usually the primary determinant of recovery in vivo (Bungay et al., 1990). The variation in recovery from probes placed in the same tissue across different experiments suggests that recovery should be estimated for each probe in every experiment. We used the zero net flux method (Lonnroth et al., 1987) to estimate recovery for the steady-state (continuous infusion) experiments and retrodialysis for the bolus experiments (Lonnroth et al., 1987; Dykstra et al., 1993; Wang et al., 1993). Although the zero net flux method provides an accurate estimate of recovery, it is time-consuming. After taking into account differences in the perfusate flow rate, retrodialysis estimates of steady-state recovery in the three tissues sampled (blood, muscle, and brain) were similar to zero net flux estimates, and the retrodialysis estimates were less variable across experiments (i.e., lower coefficient of variation). Retrodialysis, which is performed before drug administra- Zidovudine Tissue and Brain Penetration by Microdialysis 1009 Downloaded from jpet.aspetjournals.org at ASPET Journals on June 18, 2017 Fig. 3. Comparison of conventional serum and CSF zidovudine concentration profiles with microdialysis measurements in blood, muscle, and brain in each animal (85Z, H090, and 9SL) after a bolus dose of zidovudine. 85Z and H090 received 80 mg/kg zidovudine, and 9SL received 50 mg/kg. A, compares serum ultrafiltrate zidovudine concentrations (open circles) with blood microdialysis concentration (bar) in animal 85Z. All microdialysis samples for 85Z were collected over a single 4-h interval. The line represents the two-compartment model fit to the serum concentration-time data. B, compares the simulated zidovudine concentration in the peripheral compartment of the two-compartment model (solid line) with the muscle biopsies (open squares) and muscle microdialysis concentration (bar) in 85Z. C, compares zidovudine concentrations in the CSF with the brain microdialysis concentration (bar) in 85Z. The closed triangles denote the intraventricular CSF concentrations in animal 85Z. D, compares serum ultrafiltrate zidovudine concentrations (open circles) with blood microdialysis concentrations (bars) in animal 9SL. All microdialysis samples from 9SL were obtained over 1-h intervals for 4 h. The line represents the two-compartment model fit to the serum concentration-time data. E, compares the simulated zidovudine concentration in the peripheral compartment of the two-compartment model (solid line) with muscle microdialysis concentrations (bars) in animal 9SL. F, compares zidovudine concentrations in the CSF to the brain microdialysis concentrations in 9SL. The open triangles present the CSF means in the subarachnoid space of animal 9SL and the solid bars indicate the ECF means in 1-h microdialysis samples. G, compares serum ultrafiltrate zidovudine concentrations (open circles) with blood microdialysis concentrations (bars) in animal H090. All microdialysis samples from H090 were obtained over 1-h intervals for 4 h. The line represents the two-compartment model fit to the serum concentration-time data. H, compares the simulated zidovudine concentration in the peripheral compartment of the two-compartment model (solid line) with muscle microdialysis concentrations (bars) in animal H090. I, compares zidovudine concentrations in the CSF with the brain microdialysis concentrations in H090. The open triangles present the CSF means in the subarachnoid space of animal H090 and the solid bars indicate the ECF means in 1-h microdialysis samples. 1010 Fox et al. TABLE 3 Pharmacokinetic parameters derived from fitting a two-compartment model with first order elimination from the central compartment to the serum ultrafiltrate zidovudine concentration-time data after the bolus dose in three animals Model fitted parameters were Vc (volume of the central compartment), kcel (first order elimination rate constant), kcp and kpc (first order exchange rate constants describing the movement of drug from the central (c) to peripheral (p) and peripheral to central compartments). Vss (steady-state volume of distribution), clearance, and half-lives were derived from the model-fitted parameters. Model Parameters Derived Parameters Animal Vc kcp kpc ⫺1 ⫺1 ⫺1 h h Clearance Vss Half-Lifea l/kg h l/kg/h l/kg 0.13 0.43 0.48 4.7 1.1 1.6 5.2 2.1 0.9 2.1 4.6 1.4 0.60 0.50 0.79 0.44 0.64 0.79 0.76 0.94 0.99 0.35 0.19 55 2.5 1.9 78 2.7 2.2 81 2.7 1.7 63 0.63 0.15 24 0.62 0.18 29 0.90 0.12 13 85Z H090 9SL Mean S.D. CV (%) kcel h CV, coefficient of variation. a Elimination () half-life. Recovery was determined by the retrodialysis method (Table 1). CSF/serum and brain/blood ratios represent the ratio of zidovudine AUCs from the designated sampling sites. Zidovudine AUC Animal 85Z H090 9SLb Mean S.D. CV (%) Serum Blood (D) Muscle (D) M 䡠 h M 䡠 h M 䡠 h M 䡠 h M 䡠 h 490 486 363 639 634 458 491a 745 347 121 119 128 191 84 50 446 72 16.2 577 103 17.9 528 202 38.2 123 4.7 3.8 108 74 68.1 CSF Brain (D) CSF/Serum Brain/Blood (D) 0.25 0.25 0.35 0.30 0.13 0.11 0.28 0.06 20.6 0.18 0.10 58.0 CV, coefficient of variation. a Zidovudine AUC in muscle derived from multiple muscle biopsies was 335 M 䡠 h. b Animal 9SL received a bolus dose of 50 mg/kg; AUCs in this animal were normalized to a dose of 80 mg/kg. able estimate of muscle drug exposure for zidovudine. The AUC in muscle derived from serial muscle biopsies over 4 h in a single animal was lower than the microdialysis estimate of muscle ECF zidovudine AUC, but these methods measure drug concentrations in different compartments within the tissue. The homogenized muscle biopsy specimens represent an average of extracellular, intracellular, and intravascular drug concentrations within the tissue, whereas the microdialysis samples specifically measure free ECF drug concentration. From pharmacokinetic theory the equilibrium free concentration of a solute in a noneliminating compartment should be equal to the free concentration in the blood or plasma; the same identity holds for the AUC from zero to infinity. These predictions are consistent with the results of this research in which the muscle microdialysis, blood microdialysis, and serum are similar based on steady state (Table 2) and transient experiments (Table 4, 0 – 4 h AUCs). Muscle biopsies determine the total solute concentration in the tissue. For small hydrophilic solutes, which are minimally bound, the ratio of total muscle concentration to the free concentration in blood, plasma, and tissue would be expected to approximate the water content of the tissue. Zakaria et al. (2000) state that the water content of rat abdominal muscle is approximately 0.75 of the total tissue volume. The 0- to 4-h AUC of zidovudine determined from muscle biopsies in Animal 85Z was 335 M 䡠 h; the 0- to 4-h AUCs in blood microdialysis, serum, and muscle microdialysis were 639, 490, and 491 M 䡠 h, respec- tively. These correspond to total-to-free ratios of 0.52, 0.68, and 0.68. Compared with the penetration of zidovudine into muscle, the penetration of the drug into brain ECF and CSF was restricted. Although the BBB and the blood-CSF barrier differ in their anatomic location (brain capillary endothelial cells versus ependymal epithelium), their physiological function, which is to tightly regulate the composition of brain extracellular fluid and CSF, respectively, is similar. Under both steady-state conditions and transient conditions, the zidovudine concentration in the CSF and brain ECF were comparable, and the CSF/serum ultrafiltrate and brain/blood ratios were similar if one outlier is excluded. The limited penetration of zidovudine in rhesus brain presumably results from active transport mechanisms similar to those that have been shown to restrict brain penetration of zidovudine in other species (Dykstra et al., 1993; Wang et al., 1997). References Adamson PC, Balis FM, Arndt CA, Holcenberg JS, Narang PK, Murphy RF, Gillespie AJ, and Poplack DG (1991) Intrathecal 6-mercaptopurine: preclinical pharmacology, phase I/II trial and pharmacokinetic study. Cancer Res 51:6079 – 6083. Bacher JD, Balis FM, McCully CL, and Godwin KS (1994) Cerebral subarachnoid sampling of cerebrospinal fluid in the rhesus monkey. Lab Animal Sci 44:148 –152. Balis FM, Pizzo PA, Murphy RF, Eddy J, Jarosinski PF, Falloon J, Broder S, and Poplack DG (1989) The pharmacokinetics of zidovudine administered by continuous infusion in children. Ann Internal Med 110:279 –285. Benveniste H and Huttemeier PC (1990) Microdialysis theory and application. Prog Neurobiol 35:195–215. Blaney S, Cole DE, Godwin K, Sung C, Poplack DG, and Balis FM (1995) Intrathecal administration of topotecan in nonhuman primates. Cancer Chemother Pharmacol 36:121–124. Downloaded from jpet.aspetjournals.org at ASPET Journals on June 18, 2017 TABLE 4 AUCs in serum ultrafiltrate and CSF collected by conventional methods and in blood, muscle, and brain collected by microdialysis (D) after a bolus dose of 50 or 80 mg/kg Zidovudine Tissue and Brain Penetration by Microdialysis (1991) Quantitative microdialysis, in Microdialysis in the Neurosciences (Robinson TE and Justice JB Jr eds) pp 47– 80, Elsevier Publishing Co., Amsterdam. Muller M, Schmid R, Georgopoulos A, Buxbau A, Wasicek C, and Eichler H-G (1995) Application of microdialysis to clinical pharmacokinetics in humans. Clin Pharmacol Ther 57:371–380. National Research Council (1996) Guide for the Care and Use of Laboratory Animals. National Academy Press, Washington, DC. Rowland M and Tozer TN (1980) Clinical Pharmackinetics: Concepts and Applications. Lea & Febiger, Philadelphia. Stenken JA (1999) Methods and issues in microdialysis calibration. Anal Chim Acta 379:337–358. van den Bongard HJ, Mathot RA, Beijnen JH, and Schellens JH (2000) Pharmacokinetically guided administration of chemotherapeutic agents. Clin Pharmacokinet 39:345–367. Wang Y, Wei Y, and Sawchuk RJ (1997) Zidovudine transport within the rabbit brain during intracerebroventricular administration and the effect of probenecid. J Pharm Sci 86:1484 –1490. Wang Y, Wong SL, and Sawchuk RJ (1993) Microdialysis calibration using retrodialysis and zero-net flux: application to a study of the distribution of zidovudine to rabbit cerebrospinal fluid and thalamus. Pharm Res 10:1411–1419. Zakaria ER, Lofthouse J, and Flessner MF (2000) Effect of intraperitoneal pressures on tissue water of the abdominal muscle. Am J Physiol Renal Physiol 278:F875– F885. Zhao Y, Liang X, and Lunte CE (1995) Comparison of recovery and delivery in vitro for calibration of microdialysis probes. Anal Chim Acta 316:403– 410. Address correspondence to: Elizabeth Fox, Pharmacology and Experimental Therapeutics Section Pediatric Oncology Branch, National Cancer Institute, 10/13C103, 10 Center Dr., MSC 1920, Bethesda, MD 20892-1920. E-mail: [email protected] Downloaded from jpet.aspetjournals.org at ASPET Journals on June 18, 2017 Bungay PM, Dedrick RL, Fox E, and Balis FM (2001) Probe calibration in transient microdialysis in vivo. Pharm Res 18:361–366. Bungay PM, Morrison PF, and Dedrick RL (1990) Steady-state theory for quantitative microdialysis of solutes and water in vivo and in vitro. Life Sci 46:105–119. Collins JM, Klecker RW, Jr, Kelley JA, Roth JS, McCully CL, Balis FM, and Poplack DG (1988) Pyrimidine dideoxyribonucleosides: selectivity of penetration into cerebrospinal fluid. J Pharmacol Exp Ther 245:466 – 470. Davies MI (1999) A review of microdialysis sampling for pharmacokinetic applications. Anal Chim Acta 379:227–249. Dykstra KH, Arya A, Arriola DM, Bungay PM, Morrison PF, and Dedrick RL (1993) Microdialysis study of zidovudine (AZT) transport in rat brain. J Pharmacol Exp Ther 267:1227–1236. Elmquist WF and Sawchuk RJ (1997) Application of microdialysis in pharmacokinetic studies. Pharm Res 14:267–288. Gibaldi M and Perrier D (1982) Pharmacokinetics. Marcel Dekker, New York. Hsiao JK, Ball BA, Morrison PF, Mefford IN, and Bungay PM (1990) Effects of different semipermeable membranes on in vitro and in vivo performance of microdialysis probes. J Neurochem 54:1449 –1452. Johansen MJ, Newman RA, and Madden T (1997) The use of microdialysis in pharmacokinetics and pharmacodynamics. Pharmacotherapy 17:464 – 480. Klecker R, Jr, Collins JM, Yarchoan R, Thomas R, Broder S, Myers CE (1987) Clinical pharmacology of 3⬘-azido-3⬘deoxythymidine: a novel pyrimidine analog with potential application for the treatment of patients with AIDS and related diseases. Clin Pharmacol Ther 41:407– 412. Lonnroth P, Jansson P-A, and Smith U (1987) A microdialysis method allowing characterization of intercellular water space in humans. Am J Physiol 253:E228 – E231. McCully CL, Balis F, Bacher J, Phillips J, and Poplack D (1990) A rhesus monkey model for continuous infusion of drugs into cerebrospinal fluid. Lab Animal Sci 40:520 –525. Morrison PF, Bungay PM, Hsiao JK, Mefford IN, Dysktra KH, and Dedrick RL 1011