Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Mental health professional wikipedia , lookup
Parkinson's disease wikipedia , lookup
History of psychiatry wikipedia , lookup
History of psychiatric institutions wikipedia , lookup
Stress management wikipedia , lookup
Child psychopathology wikipedia , lookup
Victor Skumin wikipedia , lookup
Causes of mental disorders wikipedia , lookup
Controversy surrounding psychiatry wikipedia , lookup
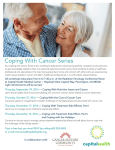
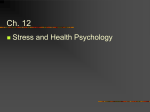
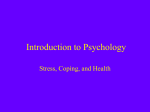
Copyright 2000 by The Gerontological Society of America The Cerontotogist Vol. 40, No. 1, 53-63 This study examines three categories of disease-related stressors (i.e., physical, cognitive, psychosocial), differential coping, and mental and physical health outcomes in individuals with Parkinson's disease (PD). Findings show that tremors, lack of mental energy, and being dependent on others were the most stressful symptoms in each category. Although there was evidence that PD patients match coping efforts to types of stressors, emotional regulation was the most common coping strategy. Hierarchical regression analyses show that disease-related variables influence every domain of quality of life, whereas the effects of coping are more selective. Specifically, the use of distancing was related to poorer mental and physical health outcomes. Findings focus attention on the disease-related stressors that create the experience of being chronically ill. Key Words: Disease-related stressors, Coping, Quality of life, Parkinson's disease Coping With Disease-Related Stressors in Parkinson's Disease Leslie D. Frazier, PhD1 Many different diseases have provided a context for research on coping and adaptation to chronic illness (see Maes, Leventhal, & de Ridder, 1996; Stone, Kennedy-Moore, & Neale, 1995). The extant literature has demonstrated the processes through which patients cope with the impact of being chronically ill or having a particular illness. However, this research tells us little about how individual patients deal with the day-to-day disease-related symptoms that create what we know generally as the stress of chronic illness. In an attempt to explore this issue, the present study examined whether different types of symptoms evoke different coping strategies and which coping strategies are related to lessened distress and higher quality of life for patients with Parkinson's disease (PD). For those diagnosed with a chronic illness, there are a variety of potentially stressful events that present unique threats and challenges. Situations or problems appraised as stressful are generally those that are perceived to tax or exceed one's available resources (Lazarus & Folkman, 1984). Regardless of disease, the impact of the illness affects many domains of functioning, which may consequently produce stress. PD was chosen as the context in which to explore disease-related stress and coping because, like other chronic conditions, the stress it produces is multidimensional and multifaceted. In addition, PD presents an ideal context for studying stress and coping because it is highly unpredictable and largely uncontrollable, and because little is known about the psychosocial aspects of this illness (Dakof & Mendelsohn, 1986; Koplas et al., 1999; Shifren, 1996). Idiopathic PD is a chronic, progressive, degenerative, neurological disorder affecting 1 % of the population older than 55 years of age (Cummings, 1999; Stern, 1988). PD patients report many troubling physical symptoms such as tremors, rigidity, and drooling. Patients also report problems with cognitive functioning such as memory impairment and confusion (Hobson & Meara, 1999). Psychosocial functioning may also be impaired, as many patients report changes in interpersonal relationships and social roles, feelings of being a burden, and loss of control over their lives (Duvoisin, 1 9 9 1 ) . The current study identifies several domains (i.e., physical, cognitive, psychosocial) comprising myriad symptoms capable of producing stress, for which different coping strategies may be differentially useful for managing the illness. Coping With Chronic Illness Coping with illness is not a monolithic process (Shifren, 1996). Although research has revealed some patterns of coping that patients often use to manage their conditions, findings remain inconclusive as to which coping strategies best facilitate positive psychological adjustment to illness (Christensen, Benotsch, Wiebe, & Lawton, 1995; Taylor & Aspinwall, 1990). Generally, coping is conceptualized as "efforts both action-oriented and intrapsychic to manage (i.e., master, tolerate, reduce, minimize) environmental and internal demands and the conflicts among them" (Lazarus This study was supported by a grant from the Florida International University Foundation. The author wishes to thank Lisa Waid, Sepidah Shams, and Wei Li for help with data collection, Drs. Paulette Johnson and V. Vishwesvaran for statistical consulting, and three anonymous reviewers for comments on earlier drafts of the manuscript. Special thanks to Drs. Kim Shifren and Bennett Schwartz for insightful feedback throughout the research project. 'Address correspondence to Leslie D. Frazier, Department of Psychology, Florida International University, University Park Campus, Miami, FL 3 3 1 9 9 . E-mail: [email protected] Vol.40, No. 1,2000 53 & Launier, 1978, p. 3 1 1 ) . These efforts are evoked when a situation is appraised as threatening or challenging. Traditionally, coping efforts have been dichotomized into strategies aimed at removing or changing the stressor (i.e., action-oriented, problem-focused due to emotional problems, energy/fatigue, emotional well-being, social functioning, pain, and self-reported general health. Although it is well documented that chronic medical problems have a strong negative impact on functional domains of quality of life, the influence of chronic medical morbidity on psychosocial strategies), or strategies that are designed to minimize the emotional impact of stress (i.e., emotional regulation, emotion-focused strategies). Several recent studies identified promising patterns of adaptation to illness. In general, with respect to chronic illness, active coping is better than avoidant and affective domains of quality of life remains inconclusive (e.g., Koplas et al., 1999; Lawton, 1 9 9 1 ; Stewart et al., 1988). More important, the strength of the influence of disease on quality of life may vary depending on whether the quality of life dimension can be modified by adaptive strategies (Kem- coping (Taylor & Aspinwall, 1990). For example, positive pen, Jelicic, & Ormel, 1997). This finding implies a critical role for coping in the relationship between disease and quality of life. outcomes were related to the use of problem-focused or active coping, cognitive restructuring, information seeking, positive reappraisal, seeking social support, and threat minimization (Affleck, Tennen, Pfieffer, & Fifield, 1987; Brenner, Melamed, & Panush, 1994; Carver et al., 1993; Dunkel-Shetter, Folkman, & Lazarus, 1987; Felton & Revenson, 1984; Stone et al., 1995; Taylor, Lichtman, & Wood, 1984). In contrast, negative outcomes such as increased distress (Carver et al., 1993; Dunkel-Shetter et al., 1 9 8 7 ; Ray, Jeffries, & Weir, 1995), anxiety, depression and poorer psychological adjustment (Felton & Revenson, 1984), poorer social adjustment (Brenner et al., 1994), poorer illness management (Frenzei, McCaul, Glasgow, & Shafer, 1988), increased pain and functional impairment (Ray et al., 1995), and decreased quality of life (Stein, Wallston, Nicassio, & Castner, 1988), were associated with coping through emotional regulation strat- egies (e.g., wishful thinking, fantasizing, expressing emotion, blaming oneself, avoidant coping, cognitive and behavioral escape/avoidance, and behavioral disengagement or distancing). Interestingly, other research shows opposite trends. For example, in a study of cancer patients, problem-focused coping and especially vigilant monitoring of information was associated with increased side effects from chemotherapy (Card, Edwards, Harris, & McCormack, 1988). Other studies with cancer patients show that positive reappraisal was helpful (Mishel & Sorenson, 1 9 9 1 ; Taylor et al., 1984), whereas escape-avoidance and self-blame bring a sense of relief (Filipp, Klauer, Freudenberg, & Ferring, 1990; Steptoe, Sutcliff, Alien, & Coombes, 1 9 9 1 ) . Still other studies show that for the chronically ill, distancing was associated with less distress (Stone et al., 1995), and may even be adaptive (Dunkel-Shetter, Feinstein, Taylor, & Falke, 1992). Chronic Illness and Quality of Life A possible shortcoming of the research on positive adjustment to illness is the diversity of the ways these outcomes have been operationalized. One method for examining the impact of disease on mental and physical health outcomes is to assess healthrelated quality of life (Ahlstrom & Sjoden, 1996; Koplas et al., 1999; Lawton, 1 9 9 1 ; Stewart, Hays, & Ware, 1988). Quality of life is a broad and multidimensional concept including physical functioning, role limitations due to physical health, role limitations 54 Coping and Positive Adjustment: The Matching Hypothesis Several inferences can be drawn from the literature on coping and positive adjustment to illness. First, flexibility in the application of coping strategies and the use of multiple strategies may be most effective in managing the stress associated with chronic illness (e.g., Dunkel-Shetter et al., 1992; Pearlin & Schooler, 1978; Strong & Large, 1995). Active strategies and emotional regulation need not, perhaps should not, be mutually exclusive for positive adaptation. As successful coping strategies, they address different needs. Problem-focused, active strategies may be best to manage pain and discomfort, whereas emotional regulation may be best for dealing with the ambiguity and unpredictability of illness (Maes et al., 1996). Active coping may be best for behavioral change, and emotional regulation may be best for psychological reactions to illness. A second and related inference is that spontaneous or active matching of coping strategies to particular stressors is essential. The matching hypothesis suggests that for coping to be effective there must be a good fit between the individual's coping efforts and situational constraints (Christensen et al., 1995; Lazarus, 1993; Lazarus & Folkman, 1984; McCrae, 1984). For example, following the matching hypothesis, positive outcomes are more likely when problem-focused strategies are used in situations perceived as controllable. Similarly, use of emotion-focused strategies or emotional regulation is more likely to lead to positive outcomes when used in situations that are outside one's direct control (e.g., Christensen, Smith, Turner, Holman, & Gregory, 1990; Taylor & Aspinwall, 1990; Vitaliano, DeWoIfe, Maiuro, Russo, & Katon, 1990). The present study is based on the premise that coping efforts are domain specific and situationally sensitive (Aldwin & Brustrom, 1997). In each of the domains of interest (i.e., physical, cognitive, psychosocial) some stressors (symptoms) will be perceived as controllable/changeable and may evoke active coping, whereas those that are not perceived as modifiable may elicit emotional regulation or distancing (see Aldwin & Brustrom, 1997; Maes et al., 1996). With respect to the three doThe Gerontologist mains, more of the physical stressors may be helped by drug treatment and behavioral modification strategies. Cognitive stressors may be aided by compensatory strategies, but more of these stressors are not directly controllable/changeable. Many of the psychosocial stressors are emotional consequences of the disease. It may be more difficult to modify an emotional response. Therefore, coping may take the form of modifying or regulating these emotions as opposed to active, problem-focused coping. Third, at present, researchers do not know whether chronically ill patients use different coping strategies selectively or in tandem. Few studies have focused on how patients deal with the day-to-day diseaserelated symptoms that create the stress of chronic illness (but see Spirito, Stark, Gil, & Tyc, 1995). Similarly, the matching hypothesis has not yet been empirically explored in the context of coping with medical morbidity. Finally, we need to successfully identify some of the coping patterns that are consistently linked to preserving and enhancing quality of life for the chronically ill (Christensen et al., 1995; Taylor & Aspinwall, 1990). Therefore, the present study was designed to explore self-reported daily disease-related stressors (symptoms) that PD patients report to be the most stressful, and the specific strategies that they use to cope with them. Of primary interest was whether certain coping strategies work most effectively with certain types of stressors, that is, whether patients match coping strategies to particular stressors. A secondary interest was to examine the relationships between patterns of coping and mental and physical health outcomes such as perceived stress and quality of life. The study examines the following hypotheses: 1. It was expected that different types of stressors (i.e., physical symptoms, cognitive symptoms, psychosocial symptoms) would be differentially associated with different coping strategies. Following the matching hypothesis, it was hypothesized that physical stressors, which may be amenable to behavioral change, would be associated with active coping strategies. Cognitive and psychosocial stressors, which may be less able to be modified actively yet create emotional distress, were hypothesized to be associated with emotional regulation. 2. It was hypothesized that coping would predict variance in the mental and physical health outcomes (i.e., perceived stress and quality of life) beyond the effects of disease-related variables (i.e., duration, severity, effectiveness of medications). interest in participating were given the questionnaires to take home, fill out, and mail back in the prepaid return envelope. The second approach was to send letters describing the study and questionnaires with prepaid return envelopes to all names on the South Florida American Parkinson's Disease Association (SFA) mailing list (N = 375). On average, about 15% of those attending support groups returned the questionnaires. Response rate for the SFA mailing list was 47%. (The difference in response rates among the support group sample with a randomly selected subset of the mailing list subjects showed no significant differences on demographic, disease-related, or psychosocial variables.) Of the mailings, six packets were returned because the recipient had died, and 21 packets were excluded because of extensive missing data. Four packets were excluded because the score on the cognitive screening instrument was beyond the cut-off, indicating potential memory impairment. Cognitive functioning was assessed with the Short Portable Mental Status Questionnaire (SPMSQ; Pfeiffer, 1975). Five errors were delineated as the exclusion criterion (McDowell & Newell, 1996). Of the participants included in the sample, the average score on the SPMSQ (after adjusting for level of education), was .35 (5D = .82; range 0-4). These scores are within the range of intact functioning, which may include mild, occasional forgetfulness (McDowell & Newell, 1996), but which would not impair participants' ability to answer the research questions. The final sample was based on data from 145 PD patients. Participants ranged in age from 48 to 91 years with a mean of 73.4 years (SO = 6.90). Approximately 65.5% of the sample were men and 34.5% were women. Ninety-six percent of the sample were White, and the remaining were Hispanic (3%) or Native American (1 %). Whereas most of the sample were married (80%) and had been for an average of 39 years (5D = 19.5; range 1-67), 12% were widowed, 4% separated or divorced, and 4% never married. The sample was well educated; 39% had graduated from high school, 27% had some college or a business/technical degree, 17% had completed college, and another 17% had earned graduate or professional degrees. Socioeconomic status (SES) as measured by the Hollingshead Index (Hollingshead, 1975) indicated that this sample was of above-average economic status. With a range from a low of 26 to a high of 66, the average SES was 47 (5D = 10). The demographic profile of this sample is similar to samples profiled in epidemiological studies of PD (Koller et al., 1986; Marttila & Rinne, 1986). Measures Method Disease-related Questions.—Following the demographic questions, participants were asked how long they had PD and who had made the diagnosis. The perceived severity of the illness was assessed with a question: "Would you say that your symptoms are: not very severe (0); mildly severe (1); moderately severe (2); quite severe (3); very severe (4). The Participants Two avenues of recruitment were used to recruit patients with PD. One approach involved visiting PD support groups in three eastern cities. At each support group meeting, individuals who expressed Vol. 40, No. 1, 2000 55 effectiveness of their medications was assessed with the following question: "Would you say your medications are: very effective (4); quite effective (3); moderately effective (2); mildly effective ( 1 ) ; not very effective (0)." Patients were asked to list the medications and dosages they were taking. ful symptoms (i.e., physical, cognitive, psychosocial), to create nine separate conditions, for which scores on the COPE scale were measured. COPE score (i.e., mean or degree of endorsement of a particular coping strategy) was treated as the dependent variable in the subsequent analysis of variance. The stressor x coping strategy dimensions and the reliability (Cronbach's alpha) of each dimension are as follows: Active-Physical (.53); Emotions-Physical (.55); Distancing-Physical (.57); Active-Cognitive (.62); Emotions-Cognitive (.62); Distancing-Cognitive (.55); Active-Psychosocial (.68); Emotions-Psycnosocial (.62); and Distancing-Psychosocial (.60). Stressful Symptoms.—The perceived stressfulness of specific symptoms and problems associated with PD were assessed by asking patients to choose the most stressful symptom from among a list of similar symptoms. Symptoms were grouped into three categories: (1) motoric or physical symptoms which included: dressing/grooming, rigidity, difficulties with sexual activity, etc.; (2) cognitive symptoms such as: forgetful ness, difficulty concentrating, lack of mental energy, etc.; and (3) symptoms of a psychosocial or emotional nature (feeling socially isolated, being dependent on others, loss of control, etc.). Groupings of symptoms were made on the basis of the domain that the symptoms primarily affected (i.e., the type of functioning impaired by the symptom), and a similar procedure used in earlier research (Brod, Mendelsohn, & Roberts, 1998). Types of stressor were treated as independent variables to predict COPE score. Participants were first presented with the list of physical symptoms and asked to circle the most stressful symptom and to answer the coping questions with that specific symptom in mind; this procedure determined which particular symptom was the most stressful within each category and what strategies participants used to manage that symptom. The process was repeated for the cognitive and the psychosocial symptom lists. Data on stressful symptoms were later coded into numeric categories for data analysis. Coping.—Coping strategies were assessed using a modified version of the COPE Scale (Carver, Scheier, & Weintraub, 1989). The questionnaire was constructed to include 12 questions, one assessing each of the following coping behaviors: (1) active coping; (2) suppression of competing activities; (3) restraint coping; (4) instrumental social support; (5) emotional social support; (6) positive reinterpretation; (7) acceptance; (8) venting emotions; (9) turning to religion; (10) denial; ( 1 1 ) behavioral disengagement; and ( 1 2 ) mental disengagement. The instructions asked participants to answer each question about what they usually do to manage the stress associated with the symptom that they chose as the most stressful symptom. Answers ranged on a four-point scale from not very often (1) to very often (4). The 12 questions on this modified COPE questionnaire were broken down to reflect three general coping strategies: questions 1-4 were used to assess Active coping; questions 5-8 were used to assess Emotional regulation; and questions 9-12 were used to assess Distancing. Coping strategies can then be considered independent variables, and the participants' scores on the COPE questionnaire for each coping strategy could be used as a dependent variable. Coping strategies were then crossed with stress- Perceived Stress.—A global measure of perceived stress was used to determine the degree to which PD patients experience anxiety not directly related to disease symptomatology. In this way, perceived stress was conceptualized as an outcome variable. Perceived stress was assessed using the Perceived Stress Scale (PSS; Cohen, Kamarck, & Mermelstein, 1983). This is a 10-item scale designed to determine the extent to which situations in one's life are appraised as stressful. Each question asked participants about their thoughts and feelings during the last month. Answer choices ranged from never (0); almost never (1); sometimes (2); fairly often (3); very often (4). The PSS was scored (after item-reversals) by summing scores across the 10 items. High scores indicated a greater degree of stress. This measure showed high reliability; the Cronbach's alpha in the present study was .85. Quality of Life.—Quality of life was assessed using the SF-36, a 36-item health survey developed by Ware and Sherbourne (1992; see also Stewart et al., 1988). The SF-36 covers eight health-related dimensions of quality of life. The eight dimension and the reliability indices (Cronbach's alpha) of the subscale in the present sample were: physical functioning (.63); role limitations due to physical health problems (.65); role limitations due to personal or emotional problems (.70); energy/fatigue (.66); general mental health (.53); social functioning (.70); bodily pain (.49); and general health perceptions (.57). The reliability of these subscales is consistent with standardized data (Kurtinetal., 1992; McDowell & Newell, 1996). Although this scale does not yield an overall single summary score representing quality of life, scale scores within each dimension provide a unique and detailed profile of which areas of quality of life are most affected by life events such as chronic illness. For each scale, high scores indicate more positive assessments and better functioning. Scale scoring is detailed in a test manual available through the Rand corporation (Hays, Sherbourne, & Mazel, 1993). Results A Profile of Parkinson's Disease The PD patients who participated in this study had been ill for an average of 8 years (SD = 6). The 56 The Gerontologist by 14% of the patients, whereas 13% mentioned forgetfulness and 11% reported slowed thinking processes as the most stressful. There was much more variation in the psychosociai symptoms reported as stressful (see Figure 3). Being dependent on others was reported to be the most stressful by 21% of the sample, feelings of being a burden was mentioned by 17% of the sample, feelings of depression was most stressful for 15% of the sample, feelings of loss of control was reported by 14% of the sample, and difficulty being understood was reported by 10% of the PD patients. 0.20-1 0.16- oo 0.12- 0.08- 0.04- 0.00 Coping With Disease-Related Stressors: The Matching Hypothesis In order to test the primary hypothesis (i.e., the matching hypothesis), that patients would use different coping strategies (i.e., active coping, emotion regulation, distancing) for different types of Stressors (i.e., physical, cognitive, psychosociai), a 2-way (coping strategy x Stressors) within-subject analysis of variance (ANOVA) was computed. Coping strategies and types of Stressors were treated as the independent variables. Coping strategy was operationalized as a subset of four questions on the COPE questionnaire that evaluate the coping dimension. The dependent variable (a numerical score on the COPE questionnaire) was operationalized as the mean response to each subset of 4 questions on the COPE questionnaire; the mean response represents the degree of endorsement of a particular coping strategy. The independent variable, coping strategy (i.e., active coping, emotional regulation, distancing), is conceptually different from the dependent variable (i.e., mean endorsement for each strategy). The independent variable Physical Stressors Figure 1. Mean percentages of most stressful physical symptoms. length of illness ranged from 1 year to 24 years. Most patients reported the symptoms of PD were only mildly (29%) or moderately severe (36%), and most felt that their medications were moderately (43%) or quite (29%) effective. As Figure 1 shows for physical symptoms, 1 7% reported tremors as the most stressful, 14% stated the rigidity was the most stressful, 11% found getting up from a chair was the most stressful, and 11% cited fear of falling as their most stressful symptom. Needing extra effort, difficulties with walking, swallowing, and sexual activities were reported as well. Over 26% of these PD patients found the lack of mental energy to be the most stressful cognitive symptom (see Figure 2). Difficulty sleeping was mentioned 0.28-. 0.24- 0.24- 0.20- 0.20- r \ \ \ x 0.16- 0.16 = \ \ 0.12- 0.12 0.04 0.04- 0.00 n nn - fffi \ *• ^ . / y \V • f f s _\ V y / , . \ \ . \ \ ' *f •\ A s S / \'\ \ , \' \ IX^V^N' -%T -^ \ \ <;f \ \ \ 'x M '-.'-,' • f f •v/y \\' / s '*•*'. j< s 0.08- 0.08 S N S \ \ \ s »: \ \' y / •V* _\ \ \ \ • (\ V •.'. ,,S \ \ \ s • x x \\\ '/S 1 \ s \ - N f •',"'*'• SS -SS,' •* 2 Psychosociai Stressors Cognitive Stressors Figure 3. Mean percentages of most stressful psychosociai Figure 2. Mean percentages of most stressful cognitive symptoms. Vol.40, No. 1,2000 symptoms. 57 Coping Strategies Physical Cognitive Disease-Related ——•— Active ——ft—— Emotional Regulation ——O— Distancing Psycho: Stressors Figure 4. Means on COPE Questionnaire by type of stressor and coping strategy. was created prior to examining means on the COPE questionnaire. The probability of a Type I error was maintained at .05 for this and all subsequent analyses. Results showed a significant main effect of coping strategy, f(2,290) = 22.17, p < .0001. As predicted, there was a significant interaction between coping strategy and type of stressor, F(4,580) = 3.81, p < .01. However, no significant differences emerged among types of stressor, F(2,290)= 1.95; p = . 1 5 . The main effect of coping strategy was due to the fact that across all types of stressors, distancing was used significantly less than either active coping or emotional regulation (see Figure 4). The interaction was found because across all types of stressors, the coping strategies were significantly different from one another with one exception. Based on Fisher's LSD post-hoc paired t tests, for psychosocial stressors emotional regulation was not significantly different from active coping. The results of the ANOVA provided evidence that patients use different coping strategies for different types of stressors. In order to determine if this matching of coping strategies to types of stressors was adaptive, a series of Pearson product-moment correlations and point bi-serial correlations were computed. (A table of these analyses is available from the author.) Severity was significantly correlated with active coping for physical stressors, r = .29, p = .001, and distancing from physical, r = .22, p - .01, cognitive stressors, r = .22, p = .0001, and psychosocial, r = .16, p = .05. Severity was significantly positively correlated with perceived stress, r = .41, p = .0001, and significantly negatively correlated with every dimension of quality of life (p < .01). Use of active coping for physical stressors and distancing from cognitive stressors showed the same associations with mental and physical health outcomes—both significantly increased perceived stress and decreased quality of life (p < .05). Predictors of Coping and Mental and Physical Health Outcomes Findings thus far indicated that patients use coping strategies differentially, and that severity of illness was differentially associated with coping and 58 consistently associated with mental and physical health outcomes. The next set of analyses aimed to determine the effects of coping on quality of life beyond the effects of disease. Therefore, a series of hierarchical linear multiple regressions were conducted to assess the combined role of demographic variables, disease-related factors, and coping strategies in predicting perceived stress and dimensions of quality of life separately. In order to examine the contributions of coping beyond demographic and diseaserelated variables, the potential influence of age, gender, severity, effectiveness of medications, and duration of illness (henceforth referred to as disease-related factors) was forced, as a block, to enter the equation first. The change in R2 was then isolated as the unique contribution of the combined coping strategies. Table 1 shows the results of the regression analyses, including regression coefficients for coping variables entered at Step 2. In Step 1 of the first hierarchical regression, 21% of the variance in perceived stress was attributed to the combined influence of the demographic and disease-related variables, f(5,139) = 7.38, p < .0001. In Step 2, an additional 21% of the variance in perceived stress was accounted for by adding coping style to the model, F(9,131) = 5.26, p < .0001. Clearly, disease-related characteristics alone contributed to higher perceptions of stress; combined with the use of less efficient coping strategies (such as distancing, especially for cognitive stressors), perceptions of stress were magnified. In the second regression equation, disease-related variables were entered at Step 1 into a model predicting the physical functioning dimension of quality of life. The model was significant, F(5,139) = 16.20, p < .0001, indicating that over 37% of the variance in physical functioning was predicted by severity, effectiveness of medication, duration, age, and gender. However, the contributions of coping were negligible. When entered into the equation at Step 2, the change was not significant. A similar picture emerged for the physical limitations, energy, pain, and the general health dimensions of quality of life. Each of these models was significantly predicted by disease-related variables; however, the addition of coping to the model at Step 2 did not account for significant additional variance. For these outcome measures, disease-related and demographic variables were more powerful predictors than coping strategies. Conversely, the psychosocial or emotional dimensions of quality of life were significantly affected by coping beyond the effects of disease-related variables. For example, as Table 1 shows, in the initial regression equation predicting emotional limitations, 17% of the variance was due to disease-related and demographic variables, f(5,139) = 5.79, p < .0001. However, when coping strategies were added, an additional 10% of the variance was accounted for and this change was significant, F(9,131) = 1.95, p < .05. Likewise, for the emotional well-being dimension of quality of life, the disease-related/ demographic variables claimed 18% of the variance, The Gerontologist Table 1. Summary of Hierarchical Regression Analyses Displaying the Influence of Coping Beyond the Influence of Disease-related Factors (N = 145) Regression Equation Perceived stress Step 1 K 2 (Adj. K2) AR2 Step 2 R 2 (Adj. R 21 ) .21 ****(. 18) .21**** ,42****(.36) SEb Step 2. .42 Active-physical Emot. Reg-physical Dist-physical Active-cognitive Emot. Reg-cognitive Dist-cognitive Active-psychosocial Emot. Reg-psychosocial Dist-psychosocial QoL: Emotional limit. ,17****(.14) 6.39 8.60 8.97 6.22 9.96 9.01 7.17 9.74 9.24 -.08 .15 -.04 -.13 -.02 -.27* .11 .07 .07 -3.69 2.46 -2.38 -3.37 7.21 -8.54 5.93 -2.06 -4.43 3.10' 4.17 4.35 3.02 4.83 4.37 3.47 4.72 4.48 -.12 .07 -.06 -.11 .22 -.22* .19 -.06 -.12 -5.10 4.00 -2.93 4.18 -10.78 -7.66 2.78 3.92 -2.57 3.63 4.89 5.10 3.54 5.66 5.12 4.07 5.54 5.25 -.14 .10 -.07 .11 -.28 -.17 .07 -4.53 9.94 -3.10 -7.80 -1.03 -20.1 7.08 4.23 5.08 .18****(.15) .16*** ,34****(.26) Step 2 Active-physical Emot. Reg-physical Dist-physical Active-cognitive Emot. Reg-cognitive Dist-cognitive Active-psychosocial Emot. Reg-psychosocial Dist-psychosocial QoL: Social funct. Step 2 .04 .07 .12 .07 -.07 .28** -.16 -.18 .17 . 1 0 * .27****(.19) Step 2 Active-physical Emot. Reg-physical Dist-physical Active-cognitive Emot. Reg-cognitive Dist-cognitive Active-psychosocial Emot. Reg-psychosocial Dist-psychosocial QoL: Emot. well-being .98 1.32 1.38 .96 1.53 1.39 1.10 1.50 1.42 .76 1.49 .79 -.78 3.68 -1.73 -1.96 2.13 .28****(.25) .09* Active-physical Emot. Reg-physical Dist-physicai Active-cognitive Emot. Reg-cognitive Dist-cognitive Active-psychosocial Emot. Reg-psychosocial Dist-psychosocial .37****(.30) .10 -.06 Note: In each hierarchical regression at Step 1, Age, Gender, Duration, Severity, Effectiveness of medications were entered as a block. At Step 2, the nine (9) coping dimensions were entered as a block. Active-physical = active coping for physical stressors; Emot. Reg-physical = emotional regufation for physical stressors; Dist-physical = distancing for physical stressors; Active-cognitive = active coping for cognitive stressors; Emot. Reg-cognitive = emotional regulation for cognitive stressors; Dist-cognitive = distancing for cognitive stressors; Active-psychosocial = active coping for psychosocial stressors; Emot. Reg-psychosocial = emotional regulation for psychosocial stressors; Dist-psychosocial = distancing for psychosocial stressors. *p = .05; **p = .01; ***p = .001; ****p = .0001. f(5,139) = 6.13, p < .0001. Coping strategies explained an additional 16% of the variance in wellbeing. Together, disease characteristics and coping strategies predicted 34% of the variance in emotional well-being, f(9,131) = 3.37, p < .001. The social dimension of quality of life was also affected by both disease-related factors and coping. Age, gender, severity, and medical effectiveness conVol. 40, No. 1, 2000 59 tributed 28% of the variance in the social functioning, f(5,139) = 10.79, p < .0001. Coping strategies significantly improved the predictive ability of the model, f(9,131) = 2.12, p < .03, and contributed an additional 9% to the variance of the social functioning domain of quality of life. The regression analyses showed that beyond the influence of the disease itself, coping has a selective influence on mental and physical health outcomes. Severe symptoms combined with the use of distancing increased perceived stress and decreased quality of life in domains that were emotional rather than physical in nature. Conversely, quality of life was elevated when there was less use of distancing, especially for cognitive stressors or symptoms. Discussion The present study is unique for several reasons. First, it is the first examination of the differential relationships between three categories of disease-related stressors (i.e., physical, cognitive, psychosocial) and the strategies used to cope with them. Second, this study is novel in its use of the matching hypothesis within the context of coping with chronic disease. Third, this study shows the selective influence of coping beyond the impact of disease in adjustment to PD. Finally, several interesting and unexpected findings emerged that shed light on factors influencing individual differences in the experience of chronic illness and have potential for applied interventions designed to maximize quality of life for the chronically ill. Summary of Findings Of the symptoms PD patients found stressful, rigidity and tremor were most stressful in the physical domain, lack of mental energy was the most stressful in the cognitive domain, and dependency, fear of being a burden, depression, and feelings of loss of control were the most stressful in the psychosocial domain. For these stressful symptoms, patients in this study were most likely to use emotional regulation and least likely to use distancing as coping mechanisms. Severity of disease was associated with greater use of active coping for physical stressors, and greater use of distancing across all stressors; this had a negative impact on mental and physical well-being. As expected, disease-related variables were consistently strong predictors of perceived stress in each of the eight dimensions of quality of life. However, the contribution of coping was highly selective. Coping made a difference in predicting perceived stress, emotional role limitations, overall emotional well-being, and social functioning. Specifically, less use of distancing from stressful symptoms was related to better outcomes in these areas. This finding supports earlier research on coping with other chronic illnesses (Carver et al., 1993; Cronkite & Moos, 1984; Dunkel-Shetter et al., 1987; Frenzel et al., 1988; Holohan & Moos, 1987; Ray et al., 1995; Taylor & Aspinwall, 1990; Zautra & Manne, 1992). Potential Implications This study adopted a micro-level assessment of disease severity and stressful symptomatology. The findings draw attention to the importance of diseaserelated characteristics as markers of adjustment. Con- 60 sistent with the literature that has identified selfreported health as a robust predictor of mortality and morbidity (Hays, Schoenfeld, & Blazer, 1996; Idler & Kasl, 1995; Markides, Lee, Ray, & Black, 1993; Rakowski, Fleishman, Mor, & Bryant, 1993), self-reported severity of disease and perceived effectiveness of medications were indeed robust predictors of coping, perceived stress, and quality of life in the present study. Clearly, patients make realistic appraisals of different dimensions of their health status, and those assessments are consistently related to indices of adaptation. The findings reported here fit well with the matching hypothesis (Lazarus, 1993; Lazarus & Folkman, 1984; McCrae, 1984). Patients differentially utilize alternative coping strategies to manage different stressful symptoms. In effect, they tailor their coping efforts to the symptoms that they are managing. In some cases the fit is good, and higher quality of life is achieved. In other cases, when the fit is poor due to a mismatch, less desirable outcomes arise. Accordingly, it was hypothesized that physical symptoms would be more amenable to action-oriented, problem-focused coping strategies than cognitive or psychosocial symptoms (McCrae, 1984). In addition, based on early coping research it was assumed that active coping would be more effective at relieving distress (e.g., Carver et al., 1989; Lazarus & Folkman, 1984; Pearl in & Schooler, 1978). Therefore, it was quite surprising to find that the use of active coping for physical stressors was significantly correlated with higher perceived stress and lower quality of life. Severity was significantly correlated with the use of active strategies for physical stressors. As medications became less effective there was a significant increase in distancing. Other studies on coping with chronic illness have found that active coping was useful when the context permited change. However, active coping may be futile in situations in which there is little room for control or change (Christensen et al., 1995; Felton & Revenson, 1984; Lazarus & Folkman, 1984; Taylor & Aspinwall, 1990; Vitaliano et al., 1990). PD patients in this study reported that their most stressful physical symptoms were tremor, rigidity, and difficulty getting up from a chair. These are mobility problems that are managed to some degree by effective drug treatment. Yet, they may remain largely outside the patients' direct control. Therefore, it is likely that less desirable mental and physical health outcomes arise when attempts to manage these symptoms in active ways are unsuccessful and ineffective. For situations in which active strategies are less effective or a mismatch arises and leads to increased distress and lessened quality of life, the reaction may be to cope by behaviorally or emotionally disengaging or distancing. Patients in this study used distancing less than the other coping strategies, but they did engage in distancing for physical, cognitive, and psychosocial stressors. Consistent with prior research, this study shows that distancing is a less effective coping strategy, related to poorer mental and physical health outcomes (Brenner et al., 1994; Carver et al., The Gerontologist 1993; Dunkel-Shetter et al., 1992; Frenzel et al., 1988; Ray et al., 1995; Taylor & Aspinwall, 1990). Evidence from the present study showed results consistent with the matching hypothesis: that emotional regulation is important for positive mental and physical health outcomes. Evidence from past research indicates that emotion-focused coping and emotional regulation were less effective at alleviating distress (Lazarus & Folkman, 1984). Few other studies of coping with illness have found emotional regulation to be related to positive outcomes (but see Carver et al., 1993; Dunkel-Shetter et al., 1992). However, based on the patterns of coping found in the present study, effective interventions would aim to identify patients using active problem-solving for problems not amenable to change before they become discouraged and begin to rely on disengagement. These patients could be instructed in positive emotional regulation strategies as a means for facilitating successful coping and ideal outcomes. With respect to successful outcomes, in this study all domains of quality of life were affected by disease-related factors (see also Kempen et al., 1997; Koplas et al., 1999; Stewart et al., 1988). However, when patients used less effective coping strategies such as distancing, the impact was felt selectively on the emotional or psychosocial domains of quality of life such as emotional well-being, social functioning, and role limitations due to emotional problems. Ineffective coping increased distress and decreased emotional well-being, yet it did not impact physical domains of quality of life such as physical functioning, energy/fatigue, pain, or general health. Coping may not be as critical for improving physical functioning or other physical aspects of chronic illness, although it is crucial for managing cognitive and psychosocial changes associated with illness. Coping effectively may be the buffer that preserves quality of life. Conversely, ineffective coping may have a synergistic effect with the stressful ness of chronic morbidity, contributing to greater distress and lower quality of life. Potential Limitations This study has several possible limitations. First, the study was designed to explore patterns of coping; consequently, the questions on the COPE scale were condensed to represent three basic coping strategies. Admittedly, some information on the specific actions and emotional responses is lost by combining these questions. However, as a preliminary study of the effects of coping with disease symptomatology, the methodology chosen worked best. Future work has been planned to examine coping on a more subtle level. Second, research has identified the role of anxiety, negative affectivity, and personality traits such as neuroticism, in the experience of symptoms, appraisals of stress, and use of coping strategies (Diefenbach, Leventhal, E., & Leventhal, H., & Patrick-Miller, 1996; Watson & Pennebaker, 1989). Although perVol. 40, No. 1,2000 sonality was not of interest in the present study, one cannot rule out the possible influence it might have in the relationships between disease-related stressors, coping, and quality of life. Future studies of coping with chronic illness may want to integrate personality constructs in order to control their potential effects. Third, there will always be some limitations associated with self-report, retrospective measures, and self-selected samples. The majority of participants in this study were recruited from a mailing list of the South Florida PD Association. Those who received the questionnaire in the mail and chose to respond may be different than those who did not respond. Unfortunately, it is not possible to validate this conclusion. However, given the respectable response rate, large sample size, variability on demographic and disease-related parameters, and the reliability of the measures, it is safe to assume that those limitations were kept to a minimum. A caveat is also in order regarding the use of patient samples for psychosocial research. The sample used in this study varied in the age at onset and duration of illness, and may have included both familial (inherited) and nonfamilial PD patients. A clinician's assessment would have provided useful etiological information regarding the sample, and future psychosocial research should try to include such data. However, the population of patients with PD is not homogeneous, and it was an aim of the study to be as inclusive as possible in order to examine the myriad of psychosocial factors influencing the experience of living with this disease. In conclusion, the present study is unique in its examination of the day-to-day stressors that create, in part, the stress of living with chronic illness. Successful coping for chronically ill patients happens on many levels, from managing daily fluctuations in symptomatology to dealing with the reality of never being completely well again. In order to understand overall adjustment to illness, we need to understand the micro-level efforts used to cope with illness (Stone & Neale, 1984). This study identifies important features of PD that create distress and require effective coping to preserve quality of life. Although PD is a unique chronic illness, many of its symptoms (e.g., difficulties with sexual activities, lack of mental energy, feelings of being a burden) may be shared with other medical illnesses. The findings reveal several patterns of coping that lead to optimal and less than optimal adjustment. Once revealed, these patterns provide blueprints for building effective interventions that strengthen the skills needed for facilitating quality of life in the chronically ill. References Affleck, C., Tennen, H., Pfeiffer, C, & Fifield, C. (1987). Appraisals of control and predictability in adapting to a chronic disease. Journal of Personality and Social Psychology, 53, 273-279. Ahlstrom, G., & Sjoden, P.O. (1996). Coping with illness-related problems and quality of life in adult individuals with muscular dystrophy. Journal of Psychosomatic Research, 41, 365-376. Aldwin, C. M., & Brustrom, J. (1997). Theories of coping with chronic stress: Illustrations from the health psychology and aging literatures. 61 In B. H. Gottlieb (Ed.), Coping with chronic stress (pp. 75-103). Kurtin, P. S. et al., (1992). Patient-based health status measures in outpatient dialysis: Early experiences in developing an outcomes assessment program. Medical Care, 30, 136-149. Lawton, M. P. ( 1 9 9 1 ) . A multidimensional view of quality of life in frail elders. In J. E. Birren, J. E. Lubben, J. C. Rowe, & D. E. Deutchman, New York: Plenum Press. Brenner, C. F., Melamed, B. G., & Panush, R. S. (1994). Optimism and coping as determinants of psychosocial adjustment to rheumatoid arthritis, journal of Clinical Psychology in Medical Settings, 1, US134. Brod, M., Mendelsohn, G. A., & Roberts, B. (1998). Patients' experience of Parkinson's disease, lournal of Gerontology: Psychological Sciences, 538, P213-P222. Carver, C. S., Pozo, C., Harris, S. D., Noriega, V., Scheier, M. F., Robinson, D. S., Ketcham, A. S., Moffat, F. L, & Clark, K. C. (1993). How coping mediates the effect of optimism on distress: A study of women with early stage breast cancer, lournal of Personality and (Eds.), The concept and measurement of quality of life in the frail elderly (pp. 4-23). San Diego, CA: Academic Press. Lazarus, R. S. ( 1 9 9 3 ) . Coping theory and research: Past, present, and future. Psychosomatic Medicine, 55, 234-247. Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping. New York: Springer. Lazarus, R. S., & Launier, R. (1978). Stress-related transactions between person and environment. In L. A. Pervin & M. Lewis (Eds.), Internal Social Psychology, 65, 375-390. Carver, C. S., Scheier, M. F., & Weintraub, J. K. (1989). Assessing coping strategies: A theoretically based approach, lournal of Personality and Social Psychology, 56, 267-283. Christensen, A. )., Benotsch, E. G., Wiebe, ). S., & Lawton, W. ). (1995). Coping with treatment-related stress: Effects on patient adherence in hemodialysis. Journal of Consulting and Clinical Psychology 63 454-459. Christensen, A. J., Smith, T. W., Turner, C. W., Holman, J. M., & Gregory, M. C. (1990). Type of hemodialysis and preference for behavioral involvement: Interactive effects on adherence in end-stage renal disease. Health Psychology, 9, 225-236. Cohen, S., Karmarck, T., & Mermelstein, R. ( 1 9 8 3 ) . A global measure of perceived stress, lournal of Health and Social Behavior, 24, 385-396. Cronkite, R. C., & Moos, R. H. (1984). The role of predisposing and moderating factors in the stress-illness relationship, /ournal of Health and Social Behavior, 25, 372-393. Cummings, J. L. (1999). Understanding Parkinson's disease, /ournal of the American Medical Association, 281, 376-378. Dakof, G. A., & Mendelsohn, G. A. (1986). Parkinson's disease: The and external determinants of behavior (pp. 287-327). New York: Plenum. Maes, S., Leventhal, H., & de Ridder, D. T. D. (1996). Coping with chronic diseases. In M. Zeidner & N. S. Endler (Eds.), Handbook of Coping: Theory, research, applications. New York: John Wiley & Sons, Inc. Markides, K. S., Lee, D. J., Ray, L. A., & Black, S. A. (1993). Physician's ratings of health in middle and old age: A cautionary note, journal of Gerontology: Social Sciences, 48, S24-S27. Marttila, R. J., & Rinne, U. K. (1986). Clues from epidemiology of Parkinson's disease. Advances in Neurology, 45, 285-288. McCrae, R. R. (1984). Situational determinants of coping responses: Loss, threat and challenge, lournal of Personality and Social Psychology, 46, 919-928. McDoweil, I., & Newell, C. (1996). Measuring health: A guide to rating scales and questionnaires (2nd ed.). New York: Oxford University Press. Mishel, M. H., & Sorenson, D. S. ( 1 9 9 1 ) . Uncertainty in gynecological cancer. A test for the mediating functions of mastery and coping. Nursing Research, 40, 1 6 7 - 1 7 1 . Pearlin, L. I., & Schooler, C. (1978). The structure of coping, lournal of Health and Social Behavior, T), 2-21. Pfeiffer, E. (1975). A short portable mental status questionnaire for the psychological aspects of a chronic illness. Psychological Bulletin, 99, 375-387. Diefenbach, M. A., Leventhal, E. A., Leventhal, H., & Patrick-Miller, L. (1996). Negative affect relates to cross-sectional but not longitudinal symptom reporting: Data from elderly adults. Health Psychol- assessment of organic brain deficit in elderly patients, lournal of the American Geriatrics Society, 23, 433-444. Rakowski, N., Fleishman, J. A., Mor, V., & Bryant, S. A. (1993). Selfassessments of health and mortality among older persons: Do ogy, 15, 282-288. Dunkel-Shetter, C., Feinstein, L. G., Taylor, S. E., & Falke, R. L. (1992). Patterns of coping with cancer. Health Psychology, 11, 79-87. Dunkel-Shetter, C., Folkman, S., & Lazarus, R. S., (1987). Correlates of social support receipt, lournal of Personality and Social Psychology, 53, 71-80. Duvoisin, R. C. ( 1 9 9 1 ) . Parkinson's disease: A guide for patient and family. New York: Raven Press. questions other than global self-reported health predict mortality? Ray, Research on Aging, 15, 9 2 - 1 1 6 . C., jefferies, S., & Weir, W. R. C. (1995). Coping with chronic fatigue syndrome: Illness responses and their relationship with fatigue, functional impairment and emotional status. Psychological Medicine, 25, 937-945. Felton, B. J., & Revenson, T. A. (1984). Coping with chronic illness: A Shifren, K. (1996). Individual differences in the perception of optimism and disease severity: A study among individuals with Parkinson's study of illness controllability and the influence of coping strate- gies on psychological adjustment, lournal of Consulting and Clinical Psychology, 52, 343-353. disease, lournal of Behavioral Medicine, 19, 2 4 1 - 2 7 1 . Spirito, A., Stark, L. J., Gil, K. M., & Tyc, V. L. (1995). Coping with everyday and disease-related stressors by chronically ill children and adolescents, /ournal of the American Academy of Child and Filipp, S. H., Klauer, T., Freudenberg, E., & Ferring, D. (1990). The regulation of subjective well-being in cancer patients: An analysis of coping effectiveness. Psychology and Health, 4, 305-317. Frenzel, M. P., McCaul, K. D., Glasgow, R. E., & Shafer, L. C. (1988). The relationship of stress and coping to regimen adherence and glycemic control of diabetes, lournal of Social and Clinical Psychology, 6, 77-87. Card, D., Edwards, P. W., Hams, J., & McCormack, G. (1988). Sensitizing effects of pretreatment measures on cancer chemotherapy nausea and vomiting, lournal of Consulting and Clinical Psychology, 56, 80-84. Hays, R. D., Schoenfeld, D. E., & Blazer, D. G. (1996). Determinants Adolescent Psychiatry, 34, 283-290. Stein, M. j., Wallston, K. A., Nicassio, P. M., & Castner, N. M. (1988). Correlates of a clinical classification schema for the arthritis helplessness subscale. Arthritis and Rheumatism, 31, 876-881. Steptoe, A., Sutcliffe, I., Alien, B., & Coombes, C. ( 1 9 9 1 ) . Satisfaction with communication, medical knowledge, and coping style in pa- tients with metastic cancer. Social Science & Medicine, 32, 627632. Stern, M. B. (1988). The clinical characteristics of Parkinson's disease and Parkinsonian syndromes: Diagnosis and assessment. In M. B. Stern & H. I. Hurtig (Eds.), The comprehensive management of Parkinson's disease (pp. 3-50). New York: PMA. Stewart, A. L., Hays, R. D., & Ware, J. E. (1988). The MOS short form general health survey: Reliability and validity in a patient population. Medical Care, 26, 724-735. Stone, A. A., Kennedy-Moore, E., & Neale, J. M. (1995). Association between daily coping and end-of-day mood. Health Psychology, of poor self-reported health in late life. American Journal of Geriatric Psychiatry, 4, 188-196. Hays, R. D., Sherbourne, C. D., & Mazel, R. M. ( 1 9 9 3 ) . The RAND 36item health survey 1 . 0 . Health Economics, 2, 217-227. Hobson, P., & Meara, J. (1999). The detection of dementia and cognitive impairment in a community population of elderly people with Parkinson's disease by use of the CAMCOG neuropsychological 14, 341-349. Stone, A. A., & Neale, J. M. (1984). A new measure of daily coping: Development and preliminary results, lournal of Personality and Social Psychology, 46, 892-906. tests. Age and Ageing, 28, 39. Hollingshead, A. B. (1975). A Four-Factor Index of Social Status. New Haven, CT: Yale University Press. Holohan, C. J., & Moos, R. H. (1987). Personal and contextual determinants of coping strategies, journal of Personality and Social Psychology, 52, 946-955. Idler, E. L., & Kasl, S. V. (1995). Self-ratings of health: Do they also predict change in functional abilities? lournal of Gerontology: Social Sciences, 50, S344-S353. Kempen, G. I., jelicic, M., & Ormel, J. (1997). Personality, chronic medical morbidity, and health-related quality of life among older persons. Health Psychology, 16, 539-546. Strong, )., & Large, R. C. (1995). Coping with chronic low back pain: An idiographic exploration through focus groups. International journal of Psychiatry in Medicine, 25, 371-387. Taylor, S. E., & Aspinwall, L. G. (1990). Psychosocial aspects of chronic illness. In P. T. Costa & G. R. VandenBos (Eds.), Psychological aspects of serious illness: Chronic conditions, fatal diseases, and clinical care (pp. 3-60). Washington, DC: American Psychological Association. Taylor, S. E., Lichtman, R. R., & Wood, J. V. (1984). Attributions, beliefs about control, and adjustment to breast cancer, lournal of Personality and Social Psychology, 46, 489-502. Vitaliano, P. P., DeWoIfe, D. J., Maiuro, R. D., Russo, j., & Katon, W. (1990). Appraised changeability of a stressor as a modifier of the Koller, W., O'Hara, R., Weiner, W., Lang, A., Nutt, )., Agid, Y., Bonnett, A. M., & jankovic, J. (1986). Relationship of aging to Parkinson's disease. Advances in Neurology, 45, 3 1 7 - 3 2 1 . Koplas, P. A. et al., (1999). Quality of life and Parkinson's disease. lournal of Gerontology: Medical Sciences, 54, M197-202. 62 The Gerontologist relationship between coping and depression: A test of the hypothesis of fit. Journal of Personality and Social Psychology, 59, 582-592. Ware, J. E., & Sherbourne, C. D. (1992). The MOS 36-item short-form Zautra, A. J., & Manne, S. L. (1992). Coping with rheumatoid arthritis: A review of a decade of research. Annals of Behavioral Medicine, 14, 31-39. health survey (SF-36): I. Conceptual framework and item selection. Medical Care, 30, 473-483. Watson, D. & Pennebaker, J. W. (1989). Health complaints, stress, and Received May 12, 1999 distress: Exploring the central role of negative affectivity. Psychological Review, 96, 234-264. Accepted October 5, 7999 Decision Editor: Vernon L. Creene, PhD CALL FOR PAPERS! The 53rd Annual Scientific Meeting of The Gerontological Society of America November 17-21, 2000, Washington, D.C. Abstracts due April 3, 2000. See www.geron.org for details. Vol.40, No. 1,2000 63