Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
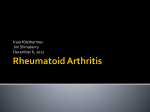
From www.bloodjournal.org by guest on June 18, 2017. For personal use only. IMMUNOBIOLOGY Allogeneic T regulatory cell–mediated transplantation tolerance in adoptive therapy depends on dominant peripheral suppression and central tolerance Dennis Adeegbe,1 Robert B. Levy,1 and Thomas R. Malek1,2 1Department of Microbiology and Immunology and 2Diabetes Research Institute, Miller School of Medicine, University of Miami, FL T regulatory cells (Tregs) represent agents to mediate tolerance to allografts so that the use of immunosuppressive drugs is avoided. In this regard, we previously demonstrated that the adoptive transfer of allogeneic Tregs into IL-2Rⴚ/ⴚ mice prevented autoimmunity and led to allograft tolerance. Here, we investigated the requirements and mechanisms that favor this long-lasting tolerance. The most potent tolerance required exact matching of all alloantigens between the adoptively transferred allogeneic Tregs and allo- geneic skin grafts, but tolerance to such allografts that lacked expression of major histocompatibility complex class I or II molecules also occurred. Thus, Tregs are not required to directly recognize major histocompatibility complex class II alloantigens to suppress skin transplant rejection. Depletion of allogeneic Tregs substantially, but not completely, abrogated this form of tolerance. However, thymocytes from allogeneic Treg adoptively transferred IL-2Rⴚ/ⴚ mice did not reject the corresponding allogeneic skin graft in secondary Scid recipients. Consistent with a requirement for a deletional mechanism in this IL-2Rⴚ/ⴚ model, a small number of wild-type T cells readily abrogated the immune tolerant state. Collectively, these findings indicate that full tolerance induction is largely dependent on substantial Treg-mediated suppression and thymic deletion of alloreactive T cells and may represent general conditions for Treg-mediated transplantation tolerance. (Blood. 2010;115:1932-1940) Introduction CD4⫹CD25⫹Foxp3⫹ T regulatory (Treg) cells inhibit a wide array of immune responses1-3 and effectively prevent the destruction of host tissue in graft-versus-host disease (GVHD).4-8 Treg cells also inhibit autoreactive and alloreactive T-cell responses in various autoimmune and transplantation studies, respectively, thus promoting tolerance.9-15 The potent suppressive activity of Treg cells has led to substantial interest in investigating their therapeutic use to facilitate tissue/organ transplantation.16-18 In most of these studies, the Treg cells infused to promote tolerance are syngeneic to the recipient. With respect to transplantation tolerance, current data support the notion that Treg cells use mainly the indirect antigen recognition pathway in the control of alloreactive immune responses.19-21 One key issue is whether adoptively transferred histoincompatible Treg cells induce transplantation tolerance without a requirement for additional immunosuppression. The use of major histocompatibility complex (MHC)–mismatched Treg cells may be required in settings in which endogenous Treg cells exhibit intrinsic defects that limit their efficacy to suppress auto- and/or alloimmunity and increase the potential donor pool for adoptive Treg cell immunotherapy. In experimental allogeneic bone marrow transplantation of mice, infusion of donor-derived allogeneic Treg cells at the time of the bone marrow transplant effectively suppresses acute GVHD.4,22,23 These preclinical findings provide the rationale for the initial Treg cell trials, which administer donor-type allogeneic Treg cells in patients undergoing human leukocyte antigen– matched allogeneic bone marrow transplantation.24 Thus, there is heightened interest in the basis by which allogeneic Treg cells mediate transplantation tolerance. In this regard, we previously reported that adoptive therapy that uses allogeneic donor Treg cells in IL-2R–deficient mice not only fully prevented their lethal systemic autoimmune disease but also resulted in long-lasting transplantation tolerance when such mice received allogeneic skin grafts that expressed the MHC type of the donor Treg cells.25 However, little is known about the T-cell receptor (TCR):MHC requirements governing Treg-cell recognition and suppression of graft rejection across MHC barriers in adoptive transfer settings in which donor Treg cells are MHC disparate from the recipient. Here we address that issue as well as more broadly investigate that mechanisms by which allo-Treg cells support skin graft tolerance by using Treg-cell transfers into IL-2R–deficient mice as a model. Methods Mice C57BL/6 (B6), BALB/c, C3H/HeJ, B6 2microglobulin-deficient (B6 2m⫺/⫺; B6.129p2-B2mtm1Unc), BALB.B (C.B10-H2b/LiMcdj), B6bm3 (B6J-H2bm3/Egj), B6bm12 (B6(C)-H-2-AB1bm12/KhEgj), and B6 MHC class II–deficient (B6 II⫺/⫺; B6.129S-H2dlAb1⫺Ea/J) mice were obtained from The Jackson Laboratory. B6 mice congenic for CD45 and expressing the CD45.1 allele (B6.SJL-Ptprc/BoAiTac), B6 Rag2/␥c double-deficient mice (B6 ⫻ C57BL/10SgSnAi-[KO]␥c-[KO]Rag2), and BALB/cscid (C.B-17 scid/scid) mice were obtained from Taconic Farms. B6 and BALB/c IL-2R⫺/⫺ mice have been previously described.12 These mice were maintained in our animal colony by breeding homozygous IL-2R⫺/⫺ pairs that were rendered autoimmune-free by neonatal adoptive transfer of purified wild-type (WT) syngeneic CD4⫹ or CD4⫹CD25⫹ T cells. All Submitted August 13, 2009; accepted December 8, 2009. Prepublished online as Blood First Edition paper, December 29, 2009; DOI 10.1182/blood-2009-08238584. payment. Therefore, and solely to indicate this fact, this article is hereby marked ‘‘advertisement’’ in accordance with 18 USC section 1734. The publication costs of this article were defrayed in part by page charge © 2010 by The American Society of Hematology 1932 BLOOD, 11 MARCH 2010 䡠 VOLUME 115, NUMBER 10 From www.bloodjournal.org by guest on June 18, 2017. For personal use only. BLOOD, 11 MARCH 2010 䡠 VOLUME 115, NUMBER 10 LONG-TERM ALLOTOLERANCE AND DONOR Treg CELLS 1933 Table 1. Summary of autoimmune status, donor engraftment, and skin graft tolerance for IL-2Rⴚ/ⴚ mice adoptively transferred with Treg cells Donor Treg strain Skin graft (MST) IL-2Rⴚ/ⴚ recipient strain Percent donor cell engraftment (ⴞ SEM) Percent CD4ⴙCD69ⴙ (ⴞ SEM) BALB/c B6 C3H n B6 B6 9.1 ⫾ 0.7 10.1 ⫾ 4.5 31 ⬎ 90 33 8 BALB/c B6 8.2 ⫾ 1.9 14.2 ⫾ 4.7 ⬎ 90 ⬎ 90 29 8 BALB/c BALB/c 8.5 ⫾ 0.9 12.5 ⫾ 3.8 ⬎ 90 29 31 8 B6 BALB/c 7.6 ⫾ 1.4 13.6 ⫾ 3.4 ⬎ 90 ⬎ 90 30 9 BALB/c 8.0 ⫾ 1.6 15.1 ⫾ 4.0 ⬎ 90 32 ⬎ 90 4 C3H B6 or BALB/c IL-2R⫺/⫺ mice were adoptively transferred at birth with Treg cells from the indicated strains of mice. The recipients were judged to be autoimmune-free. Host CD4⫹ T cells that express ⬍ 20% CD69⫹ cells represent one indicator of lack of autoimmunity. These mice received BALB/c, B6, and C3H skin grafts 8 weeks after the Treg cell transfers. Mice were monitored up to at least 90 days after skin transplantation. The percentage of donor cell engraftment was then determined as the percentage of CD4⫹ splenic T cells that were donor Treg cells, defined by expression of CD25 and/or Foxp3. The mean survival time (MST) of the skin grafts and number of recipient mice (n) are indicated. Data are a composite of previously published data19 and additional skin graft recipients. experiments were approved by the Institutional Animal Use Committee at the University of Miami. Antibodies and FACS analysis Biotin-conjugated monoclonal antibodies (mAbs) to H-2Kb (AF6-88.5), Cy-Chrome–conjugated mAbs to CD4 (H129.19), and Cy-Chrome– streptavidin, phycoerythrin (PE)–conjugated mAbs to CD25 (PC61), CD4 (GK1.5), H-2Kb (AF6-88.5), H-2Kd (SF1-1.1), PerCP-conjugated mAbs to CD4 (RM4-5), and allophycocyanin-streptavidin were all purchased from BD Biosciences. Fluorescein isothiocyanate–anti-CD4 (GK1.5), fluorescein isothiocyanate–anti-CD45.1, biotin-conjugated mAbs to CD45.1 (A20.1), and CD25 (7D4) were prepared in our laboratory. PE–anti-Foxp3 (FJK16s) was obtained from eBiosciences and was used in intracellular fluorescence-activated cell sorting (FACS) analysis by the use of a kit according to the manufacturer’s instructions. FACS analysis was performed as previously described26 with a Becton Dickinson LSR1 cytometer and CellQuest software or a BD Biosciences LSRII cytometer and Diva software. Typically 30 000 to 50 000 events were collected per sample. Purification of T-cell subsets Unfractionated or CD4⫹ T cells were isolated by the use of Thy 1.2 MACS or anti-CD4 MicroBeads, respectively, by positive selection on MS MACS separation columns (Miltenyi Biotec). CD4⫹CD25⫹ T cells were purified from the spleen as previously described12 by initial depletion of CD8⫹ T cells and B cells, followed by positive selection of Treg cells targeting CD25 with magnetic micro beads. Cell purity typically ranged from 90% to 95% as analyzed by FACS. Donor B6 (H-2b) cells were depleted by negative selection after incubating spleen cell suspensions with biotinconjugated anti-H-2kb (AF6-88.5) and streptavidin MACS MicroBeads. Donor BALB/c (H-2d) cells were depleted either by negative selection after spleen cell suspensions were incubated with PE-conjugated H-2kd (SF11.1) mAb and anti-PE MACS MicroBeads or by cell sorting by the use of a Becton Dickinson Vantage SE cell sorter. CD25⫹ cell depletion was performed by incubating spleen cells with anti-CD25 (7D4) and complement.12 The source of antigen-presenting cells (APCs) was T cell–depleted mitomycin C–treated spleen cells as previously described.12 In vivo mouse studies For experimental studies, purified CD4⫹CD25⫹ Treg cells (2 ⫻ 105) were adoptively transferred by intravenous injection into the superficial facial vein of 1- to 2-day-old neonatal IL-2R⫺/⫺ mice. At 8 to 12 weeks later, the adoptively treated mice were used for skin graft experiments and other in vitro assays. In transplantation studies that used Rag2⫺/⫺/␥c⫺/⫺ or BALB/ cscid mice, cell inoculums were injected in the tail vein of recipient mice. Skin grafting was performed as previously described.25 In brief, syngeneic, test tolerogenic allogeneic, and third-party allogeneic full-thickness tail skin from WT female donors were serially placed in tandem on separate graft beds on the tail of individual anesthetized recipients. Protective glass tubing was placed over the length of the tail bearing the grafts for 7 days. Grafts were monitored every other day and scored as rejected when greater than 75% or more of the original graft tissue had become necrotic as assessed by visual examination. Grafts were scored from 0 to 4 as follows: 0, graft is healthy and is intact; 1, graft is inflamed, but no signs of necrosis; 2, graft is inflamed, necrosis of less than 50% of graft area; 3, necrosis of up to 75% of graft area; and 4, complete loss of graft. Statistical analysis A paired 1-tailed Student t test was used to compare the mean survival time (MST) between allogeneic third-party and test tolerogenic allogeneic skin grafts and an unpaired 2-tailed Student t test was used to compare the mixed lymphocyte response (MLR) responses. Results Allogeneic donor Treg cells mediate donor-specific skin graft tolerance IL-2R⫺/⫺ mice lack mature and functional CD4⫹CD25⫹Foxp3⫹ Treg cells and consequently develop severe lethal systemic autoimmune disease that in many ways resembles GVHD.12,27 This absence of mature endogenous Treg cells provides a model to follow a defined population of transferred donor Treg cells and investigate their suppressive function and mechanisms of action in vivo. We previously demonstrated that the adoptive transfer of either syngeneic or allogeneic Treg cells into neonatal IL-2R⫺/⫺ mice fully prevented their lethal autoimmunity such that they now lived a normal life span with a normal fraction of donor Treg cells.12,25 Thus, the allo-Treg cells were not rejected by the IL-2R⫺/⫺ recipients. Remarkably, autoimmune-free IL-2R⫺/⫺ mice that received allogeneic Treg cells consistently exhibited long-term (defined typically as ⬎ 90 days) tolerance to allogeneic skin grafts that expressed the same genetic background as the donor Treg cells.25 The effectiveness of allogeneic Treg cells in this setting has been found for all 3 strain combinations that have been tested so far, that is, BALB/c (H2d) Treg cells into B6 (H2b) IL-2R⫺/⫺ recipients, B6 Treg cells into BALB/c IL-2R⫺/⫺ recipients, and C3H (H2k) Treg cells into BALB/c IL-2R⫺/⫺ recipients. A summary of all recipients to date for these strain combinations with respect to skin graft tolerance and donor Treg cell persistence is shown in Table 1. For simplicity in this report, the donor Treg cells strain into IL-2R⫺/⫺ recipient strain will be designated, for example, as B6 Treg3BALB/c⫺/⫺. Transplantation tolerance with alloantigen disparities between donor Treg cells and skin graft Past work25 also showed delayed (MST ⫽ 48 days) rejection when grafting allogeneic skin from F1 mice as long as 1 haplotype was From www.bloodjournal.org by guest on June 18, 2017. For personal use only. 1934 ADEEGBE et al BLOOD, 11 MARCH 2010 䡠 VOLUME 115, NUMBER 10 Figure 1. Skin graft survival when the donor Treg cells and allograft differ in only a single MHC class I or II alloantigen. Eight- to 12-week-old BALB/c IL-2R⫺/⫺ mice that were adoptively treated with the indicated population of Treg cells at birth (denoted as the donor Treg strain3IL-2R⫺/⫺ recipient strain) received BALB/c, C3H, and B6bm3 (B6bm3) or B6bm12 (B6bm12) skin grafts. (A) Tolerance to B6bm3 skin. (B) Tolerance to B6bm12 skin. The number of mice/group, combined from 2 independent experiments, and the MST of the allogeneic skin grafts are listed within each panel of the figure. matched with the donor allogeneic Treg cells. This finding suggested that a dominant tolerance mechanism may be operative in our system. Therefore, we more fully investigated the requirements for alloantigen similarity between the donor Treg cells and the skin graft. Accordingly, skin transplantation experiments were performed by the use of grafts that differed in only a single MHC molecule or expressed only minor alloantigenic disparities relative to the donor allogeneic Treg cells. Initially, the suppression of graft rejection to B6bm3 or B6bm12 skin grafts was examined in B6 Treg3BALB/c⫺/⫺ recipients. These skin grafts express MHC class I or class II molecules, respectively, that differ by 3 amino acids from conventional B6 MHC class I (H-2b) or class II (I-Ab).28,29 For B6 Treg3BALB/c⫺/⫺ recipients, substantial but not long-lasting tolerance was noted for B6bm3 (Figure 1A, right; P ⬍ .001) or B6bm12 (Figure 1B right; P ⬍ .001) skin grafts with MST of 64 to 69 days, whereas fully allogeneic C3H skin grafts were rejected rapidly with MST of 28 to 29 days. For B6bm3 Treg3B6⫺/⫺ (Figure 2A right) or B6 Treg3B6⫺/⫺ (Figure 2B center) recipients, B6bm12 (P ⬍ .001) or BALB.B (P ⬍ .001) skin grafts, respectively, exhibited delayed rejection. The eventual rejection of BALB.B skin grafts by B6 Treg3B6⫺/⫺ Figure 2. Skin graft survival when the donor Treg cells and allograft differ in major or minor alloantigens. Eight- to 12-week-old B6 IL-2R⫺/⫺ mice that were adoptively treated with the indicated population of Treg cells at birth (denoted as the donor Treg strain3 IL-2R⫺/⫺ recipient strain) received BALB/c, C3H, B6bm3, and B6bm12 (A) or BALB/c, BALB.B, B6, and C3H (B) skin grafts. (A) Tolerance to B6bm3 skin. (B) Tolerance to BALB.B skin. The number of mice/group from a single experiment and the MST of allogeneic skin grafts are listed within each panel of the figure. mice indicates that Treg selection and recognition of self-peptide/ MHC class II is not sufficient to mediate long-lasting tolerance. However, long-lasting (MST ⫽ ⬎90 days) tolerance for B6bm3 and BALB.B skin grafts was only observed for B6bm3 Treg3B6⫺/⫺ (Figure 2A right) or BALB.B Treg3B6⫺/⫺ (Figure 2B right) recipients, respectively. As additional controls for these experiments, when the donor Treg cells were syngeneic to the recipients, as in WT BALB/c mice (Figure 1A-B left), BALB/c Treg3 BALB/c⫺/⫺ recipients (Figure 1A-B center), WT B6 mice (Figure 2A-B left), and B6 Treg3B6⫺/⫺ recipients (Figure 2A-B center), mismatched C3H, B6bm3, B6bm12, and BALB.B skin grafts were rapidly rejected (MST ⫽ 17-30 days). We have always noted that WT mice rejected allogeneic skin grafts with more rapid kinetics than syngeneic Treg cells3IL-2R⫺/⫺ mice, and this difference is most likely accounted for by the lack of IL-2 responsiveness by the rejecting effector T cells in the latter mice. Collectively, these data indicate that tolerance is not sustained and is eventually abrogated when there is any disparity in major or minor alloantigens between the skin grafts and the donor allogeneic Treg cells. From www.bloodjournal.org by guest on June 18, 2017. For personal use only. BLOOD, 11 MARCH 2010 䡠 VOLUME 115, NUMBER 10 LONG-TERM ALLOTOLERANCE AND DONOR Treg CELLS 1935 Figure 3. Skin graft survival when the allograft lacks surface expression of MHC class I or II molecules. Eight- to 12-weekold BALB/c IL-2R⫺/⫺ mice that were adoptively treated with the indicated population of Treg cells at birth (denoted as the donor Treg strain3IL-2R⫺/⫺ recipient strain) received skin grafts from BALB/c, C3H, and B6 MHC-deficient mice. (A) Tolerance to B6 MHC class II–deficient (B6 II⫺/⫺) skin. (B) Tolerance to MHC class I–deficient (B6 2m⫺/⫺) skin. The number of mice/group from a single experiment and the MST of allogeneic skin grafts are listed within each panel of the figure. Transplantation tolerance toward allografts that lack expression of MHC class I or II molecules The preceding data demonstrate that the most effective tolerance occurs when the donor allogeneic Treg cells are identical with the allo-skin grafts. Because Treg cells express MHC class II– restricted TCRs, it was of interest to determine whether the skin graft must express MHC class II molecules because this may indicate that suppression is the result of a mechanism that depends on direct recognition of MHC class II molecules associated with the graft. To test this hypothesis, B6 Treg3BALB/c⫺/⫺ recipients received skin grafts from BALB/c, C3H, and MHC class II– deficient B6 II⫺/⫺ mice (Figure 3A right). These recipients retained BALB/c and B6 II⫺/⫺ donor skin for greater than 90 days whereas they readily rejected C3H skin (MST ⫽ 28 days). Control experiments revealed that WT BALB/c mice (Figure 3A left) and BALB/c Treg3BALB/c⫺/⫺ recipients (Figure 3A center) readily rejected C3H and B6 II⫺/⫺ skin grafts. These data indicate that tolerance is independent of class II expression by the donor skin transplants. Given the ubiquitous expression of MHC class I antigens on cells of the transplanted tissue, we also tested the requirement for graft-derived MHC class I antigens for allo-Treg cell–mediated tolerance. Similar skin graft experiments were performed with the use of B6 2m⫺/⫺ donor skin, which lacks surface expression of MHC class I molecules.30 This skin graft also was retained long-term by B6 Treg3BALB/c⫺/⫺ recipient mice (Figure 3B right), whereas it was readily rejected by WT BALB/c mice (Figure 3B left) and BALB/c Treg3BALB/c⫺/⫺ (Figure 3B center) recipients. Thus, allogeneic Treg cell–mediated tolerance also readily occurs in the absence of graft-associated MHC class I. Taken together, these data suggest that allogeneic donor Treg cells likely suppress rejection that is not critically dependent on direct recognition of graft-derived MHC molecules. The dependency of tolerance on donor allogeneic Treg cells One key feature of peripheral tolerance by Treg cells is active suppression of antigen-responsive cells.31-33 The delayed rejection of the partially matched skin grafts with the donor Treg cells is consistent with that notion. However, the more long-lasting tolerance in settings where skin grafts were completely matched to the donor allogeneic Treg cells in this and past work25 raise the possibility that additional mechanisms may also be in play. To evaluate the role of donor Treg cells for skin graft tolerance when the allogeneic Treg cells and the skin graft are fully matched, we used a secondary transfer system where spleen cells from BALB/c Treg3B6⫺/⫺ were transferred into B6 Rag2⫺/⫺/␥c⫺/⫺ mice and 2 days later these secondary recipients were grafted with skin from BALB/c, B6, and C3H mice. When unfractionated BALB/c Treg3B6⫺/⫺ spleen cells were transferred into B6 ␥c⫺/⫺Rag⫺/⫺ mice, all of these secondary recipients readily accepted syngeneic B6 and Treg cell-matched BALB/c skin grafts for greater than 90 days, whereas they readily rejected third-party C3H skin grafts (Figure 4A). The accepted BALB/c donor skin showed no visual signs of inflammation. Donor BALB/c Treg cells (3.1% ⫾ 0.4%) from the BALB/c Treg3B6⫺/⫺ spleen inoculum were readily detected 90 days later in the spleen of the B6 Rag2⫺/⫺/␥c⫺/⫺ secondary recipients. In contrast, secondary B6 Rag2⫺/⫺/␥c⫺/⫺ mice that received Treg cell–depleted BALB/c Figure 4. Skin graft survival in the absence of donor Treg cells. Eight-week-old B6 Rag2⫺/⫺/␥c⫺/⫺ mice (H-2b) received 7 ⫻ 106 unfractionated (A) or H-2d donor cell–depleted (B) spleen cells from BALB/c3B6⫺/⫺ mice. Rag2⫺/⫺/␥c⫺/⫺ recipients were then transplanted with BALB/c, C3H, and B6 (B6) skin 2 days after the cell transfer. Mice were monitored up to 90 days after which they were sacrificed to assess the presence of the donor Treg cells. MST of allogeneic skin grafts are listed within each panel of the figure. Data represent 9 mice/group, combined from 2 independent experiments. From www.bloodjournal.org by guest on June 18, 2017. For personal use only. 1936 ADEEGBE et al BLOOD, 11 MARCH 2010 䡠 VOLUME 115, NUMBER 10 Figure 5. MLR by T cells or APCs from IL-2Rⴚ/ⴚ mice that were adoptively transferred with allogeneic Treg cells. (A) MLR responses by WT and recipient-derived T cells to allogeneic APCs. The source of the responding T cells is listed below the x-axis. Unfractionated spleen cells (2 ⫻ 105) isolated from WT BALB/c and BALB/c3BALB/c⫺/⫺ mice or spleen cells depleted of H-2b⫹ donor cells (2 ⫻ 105) isolated from B63BALB/c⫺/⫺ mice were cultured with BALB/c (left), B6 (center), or C3H (right) APCs (2 ⫻ 105) for 96 hours. (B) MLR response of WT B6 T cells to APC derived from the spleen of indicated mice as listed below the x-axis. 3H-thymidine was added in the last 6 hours of culture. Data represent the mean ⫾ SEM of 2 to 3 independent experiments with the use of mice that were either tolerant skin graft recipients (B63BALB/c⫺/⫺) or mice that rejected both donor skin (BALB/c⫹/⫹ and BALB/c3BALB/c⫺/⫺). Treg3B6⫺/⫺ spleen cells rejected BALB/c skin grafts (MST ⫽ 52 days), although this tempo of rejection was significantly slower (P ⫽ .002) than found for third-party C3H skin grafts (MST ⫽ 34 days; Figure 4B). In this case very few donor Treg cells (0.45% ⫾ 0.13%) were found in the spleens of the B6 Rag2⫺/⫺/␥c⫺/⫺ secondary recipients. A delay of 7 days in rejection of BALB/c skin grafts was still noted for the 3 recipients within this group with the lowest level (⬍0.2%) of residual Treg cells, suggesting that this delay in rejection was Treg cell independent. Nevertheless, the rejection of allogeneic BALB/c skin grafts after Treg depletion establishes an important role for Treg cells for tolerance to allogeneic skin graft. T-cell anergy and defective APC function do not obviously contribute to transplantation tolerance Effective Treg cell–mediated dominant tolerance might be favorable to elicit other peripheral regulatory mechanisms, such as anergy, ignorance, or induction of tolerogenic APCs to the alloantigens of the skin graft that together with Treg cells result in long-lasting skin graft retention. To test this notion, MLRs were performed with T cells and APCs from B6 Treg cell3BALB/c⫺/⫺ mice. When spleen cells from B6 Treg3BALB/c⫺/⫺ mice were cultured with WT B6 or C3H APCs (Figure 5A), proliferative responses were detected that were comparable with that when the responding cells were obtained from BALB/c Treg3BALB/c⫺/⫺ mice. As expected, the MLRs from WT BALB/c mice to B6 or C3H APC (Figure 5A) were 2- to 3-fold greater, and this difference is attributable to the unresponsiveness of IL-2R⫺/⫺ T cells to IL-2 in vitro by T cells from the former groups of mice.34-36 These findings indicate that recipient IL-2R⫺/⫺ T cells are present that are capable of responding to the allo-skin grafts to which these mice are tolerant. These data are consistent with the idea that substantial T-cell alloantigen-specific anergy or ignorance cannot account for the skin graft tolerance. In an analogous manner, APCs from B6 Treg3BALB/c⫺/⫺ mice readily induced MLRs by WT B6 T cells that were very similar to the responses induced by APCs from WT BALB/c or BALB/c Treg3BALB/c⫺/⫺ mice (Figure 5B). In all 3 groups of mice, the frequency of CD11cdimB220⫹Ly6C⫹ plasmacytoid dendritic cells, which have been implicated in some settings to contribute to transplant tolerance,17 was similar (data not shown). Taken together, these data suggest that a prominent tolerogenic APC pool does not contribute to induction or maintenance of donor-specific transplantation tolerance in B6 Treg3BALB/c IL-2R⫺/⫺ mice. Central tolerance mechanisms are induced in allogeneic Treg-cell adoptively transferred IL-2Rⴚ/ⴚ mice When IL-2R⫺/⫺ mice are adoptively transferred with Treg cells, these cells undergo rapid homeostatic expansion to normal numbers and then are maintained at normal levels through extensive proliferation and corresponding cell death.26 In the case of allogeneic Treg cells, this process might provide a substantial and constant source of alloantigen for central tolerance. To test this notion, we evaluated the capacity of a mixture CD4⫹ and CD8⫹ single-positive (SP) thymocytes derived from B6 Treg3 BALB/c⫺/⫺ mice to reject skin grafts upon transfer into secondary lymphopenic BALB/cscid mice. Such secondary recipients containing thymocytes derived from B6 Treg3BALB/c⫺/⫺ mice readily rejected C3H but not B6 skin grafts (Figure 6A right). These B6 grafts exhibited some signs of immune attack, as evident by the somewhat-elevated rejection scores (Figure 6B), but this response did not progress to complete loss of the graft 90 days after thymocyte transfer. Spleen cells from these recipient BALB/cscid mice essentially lacked Foxp3⫹ Treg cells (Figure 6C-D), indicating that this tolerance is not the result of residual donor B6 Treg cells. As controls and in marked contrast, the transfer of SP thymocytes from WT BALB/c (Figure 6A left) or BALB/c Treg3BALB/c⫺/⫺ (Figure 6A center) mice into BALB/cscid secondary recipients resulted in complete rejection of B6 and C3H skin grafts with high rejection scores (Figure 6B). The spleens of these latter 2 groups of BALB/cscid mice contained Treg cells from the thymocyte inoculums (Figure 6C-D), but these cells did not affect rejection of the allogeneic skin grafts. The presence of Treg cells in these 2 latter groups was expected because it was not possible to excluded the syngeneic WT Treg cells during the sorting of the SP thymocytes. Treg cells represent approximately 4% of CD4 SP thymocytes in WT mice. WT donor syngeneic or allogeneic Treg cells are found in the thymus of adoptively transferred IL-2R⫺/⫺ mice at a low frequency (0.1%-0.2%). These cells are available to engraft and persist after thymocytes were transferred into BALB/cscid recipients. This issue was avoided in the B6 Treg3BALB/c⫺/⫺ thymocyte group because H-2b⫹ cells were specifically excluded during the cell sorting. Thus, the tolerance in secondary recipients of thymocytes from B6 Treg3BALB/c⫺/⫺ mice is consistent with the notion that the allogeneic Treg cells that are present primarily in From www.bloodjournal.org by guest on June 18, 2017. For personal use only. BLOOD, 11 MARCH 2010 䡠 VOLUME 115, NUMBER 10 LONG-TERM ALLOTOLERANCE AND DONOR Treg CELLS 1937 Figure 6. Central tolerance in IL-2Rⴚ/ⴚ mice that were adoptively transferred with allogeneic Treg cells. Eight-week-old BALB/cscid mice (H-2d) received a 4:1 mixture of FACS-sorted SP CD4⫹ and CD8⫹ cells (0.5 ⫻ 106 total) isolated from the thymus of WT BALB/c, BALB/c3BALB/c⫺/⫺, or B63BALB/c⫺/⫺ mice, the latter of which were further sorted to exclude any donor H-2b⫹ cells. BALB/cscid recipients were then transplanted with BALB/c, C3H, and B6 donor skin 2 days later. Mice were monitored up to 90 days, after which they were sacrificed to assess the presence of Treg cells. (A). Skin graft survival in BALB/cscid recipients that received the indicated donor thymocytes. The number of mice in each group of recipients and the MST of allogeneic skin grafts are listed within each the panel. (B) Rejection score of B6 skin grafts. (C) Percentage of CD4⫹Foxp3⫹ Treg cells in the whole spleen of individual recipient mice. (D) Percentage of Treg cells within the splenic CD4⫹ T-cell subset. Staining for MHC class Id and Ib confirmed that all CD4⫹ Foxp3⫹ T cells were of H-2d origin. Data are 4 to 5 mice/group from a single experiment. the periphery of IL-2R–deficient mice led to substantial central tolerance to the alloantigens expressed by the Treg cells. T cells from naive mice readily abrogate transplantation tolerance The preceding experiments demonstrate that dominant Treg cellmediated suppressive and central thymic tolerance mechanisms contribute to long-lasting skin graft acceptance when there is complete genetic matching between the allogeneic Treg cells and the allografts. To further investigate the resiliency of these mechanisms, we assessed whether such tolerance is maintained in the presence of an exogenous source of T cells from naive WT or autoimmune-free IL-2R⫺/⫺ mice. For these experiments, we performed another set of secondary adoptive transfers where spleen cells from BALB/c Treg3B6⫺/⫺ mice were transferred into B6 Rag2⫺/⫺/␥c⫺/⫺ recipients, which exhibit potent tolerance to BALB/c skin graft (see Figure 4), but now defined numbers of T cells were added to these spleen cell inoculums. In these transfers, all cells are syngeneic to the recipient with the exception of the BALB/c Treg cells present in the spleen cells from BALB/c Treg3B6⫺/⫺ mice. When the cotransferred T cells were derived from autoimmune-free B6 IL-2R⫺/⫺ mice (Figure 7A), tolerance to BALB/c skin was maintained in the presence of 2 ⫻ 105 of cotransferred IL-2R⫺/⫺ T cells, whereas delayed rejection occurred when 2 ⫻ 106 cells were cotransferred. In contrast, cotransferred WT T cells resulted in efficient rejection of BALB/c skin grafts at both doses of WT T cells (Figure 7B) that was largely comparable with the rejection of third-party C3H skin grafts (Figure 7B). We also noted (data not shown) rapid rejection (MST ⫽ 24 days) of long-term tolerant C57BL/6 skin grafts after the tolerant B6 Treg3BALB/c⫺/⫺ mice (n ⫽ 4) received BALB/c T cells (2 ⫻ 106). Figure 7. Ability of naive T cells to break skin graft tolerance of IL-2Rⴚ/ⴚ mice that were adoptively transferred with allogeneic Treg cells. Eight-weekold Rag2⫺/⫺/␥c⫺/⫺ mice (H-2b) received 7 ⫻ 106 unfractionated spleen (SP) cells isolated from BALB/c3B6⫺/⫺ mice along with the indicated numbers of unfractionated (A-B) or CD25-depleted (C) naive T cells isolated from IL-2R⫺/⫺ (A) or WT CD45.1 B6 congenic (B-C) mice. The naive T cells were from autoimmune-free IL-2R⫺/⫺ mice due to the transfer of syngeneic Treg cells at birth. Rag2⫺/⫺/ ␥c⫺/⫺ recipients were then transplanted with BALB/c, C3H, and B6 skin 2 days later. The number of mice in each group of recipients, combined from 2 independent experiments, and the MST of skin grafts are listed within each the panel. From www.bloodjournal.org by guest on June 18, 2017. For personal use only. 1938 ADEEGBE et al Upon further analysis, BALB/c Treg cells from the BALB/c Treg3 B6⫺/⫺ spleen cells were only detected in the secondary recipients that received 2 ⫻ 105 IL-2R⫺/⫺ T cells, which retained the BALB/c skin grafts (Figure 7A top), whereas such Treg cells were absent in all other B6 Rag2⫺/⫺/␥c⫺/⫺ secondary recipients (data not shown). Reducing Treg cells in the WT T cells before cotransfer by depletion of CD25⫹ T cells did not alter the time course of rejection of the BALB/c skin grafts (Figure 7C) nor promoted the persistence of the BALB/c Treg cells (data not shown). These data suggest that T cells from naive mice eliminate the allograft suppressive BALB/c Treg cells. Taken together, these data provide direct evidence that the Treg cells from the tolerogenic BALB/c Treg3B6⫺/⫺ spleen cells do not suppress WT T cells, although the alloreactive response by new input IL-2R⫺/⫺ T cells is more readily susceptible to suppression. Discussion The induction of effective tolerance to allogeneic skin in IL-2R⫺/⫺ mice is relatively straightforward, that is, resulting from singular transfer of small numbers of allogeneic Treg cells into neonatal IL-2R⫺/⫺ mice. This finding and the application of donor allogeneic Treg cells in clinical trials to suppress GVHD has led us to further investigate the basis by which allogeneic Treg cells mediate transplantation tolerance.24 Although tolerance induction is efficient and highly reproducible, complex events ensue for allograft acceptance. This study clarifies key requirements with respect to alloantigen recognition and suppressive mechanisms by which adoptively transferred allogeneic Treg cells mediated skin graft tolerance in IL-2R–deficient mice. We provide direct data for 2 mechanisms for this skin graft tolerance. First, much of the tolerance between allogeneic Treg cells and alloantigen-matched skin grafts is accounted for by donor Treg cells. When secondary adoptive transfer experiments were used, tolerance was largely abrogated upon depletion of the donor Treg cells. Thus, there is a requirement for continued presence of the donor Treg cells to mediate tolerance, consistent with active suppression by these cells as shown by others.13,37,38 Nevertheless, Treg-mediated suppression did not fully account for tolerance because some delay in graft rejection remained upon depletion of the donor Treg cells. Second, we found that central tolerance was also induced to alloantigens associated with the donor Treg cells because thymocytes from such mice did not efficiently reject skin grafts that expressed these alloantigens when transferred into secondary immunodeficient recipients. Such central tolerance provides a mechanism to further reduce the number of potential alloreactive T cells that require active suppression by Treg cells. These 2 mechanisms work in tandem to establish a finely balanced setting in which tolerance is maintained to the skin graft and the allogeneic donor Treg cells. Consistent with this notion, the addition of a few WT T cells to tolerogenic BALB/c Treg3B6⫺/⫺ spleen cells that were transferred to secondary Rag2⫺/⫺/␥c⫺/⫺ recipients readily broke transplantation tolerance to BALB/c skin grafts and the donor Treg cells. Our findings from in vitro MLR experiments suggest that peripheral T-cell anergy or the development of tolerogenic APC does not substantially account for allograft tolerance in IL-2R⫺/⫺ mice that are engrafted with allogeneic Treg cells, although some subtle contribution by these inhibitory mechanisms cannot be excluded. We believe it is noteworthy that MLR responses were readily evident by recipient T cells toward B6 APCs when the BLOOD, 11 MARCH 2010 䡠 VOLUME 115, NUMBER 10 responding cells were derived from B6 Treg3BALB/c⫺/⫺ mice. This finding indicates that there is a substantial population of T cells that directly recognize B6 or BALB/c MHC alloantigens by these tolerant recipients and are suppressed by Treg cells. This result strongly suggests that central tolerance is geared to primarily eliminate alloreactive CD4⫹ and CD8⫹ T cells that recognize indirectly presented donor-related antigens on host APCs. This MLR experiment also rules out the remote possibility that our highly purified donor Treg cells contained a rare progenitor cell that support donor APC that directly mediated thymic-negative selection. The Treg cells themselves provide a substantial source of alloantigens that is available for indirect antigen-presentation/ donor antigen uptake by host APC. Adoptively transferred syngeneic or allogeneic Treg cells are maintained at normal numbers life-long for autoimmune-free IL-2R⫺/⫺ recipients, whereas these Treg cells undergo substantial homeostatic growth and death.39 Thus, the efficient long-term engraftment of Treg cells not only results in a population of suppressive Treg cells but yield substantial chimerism to provide alloantigens to support long-term central tolerance mechanisms. Such indirectly presented alloantigens may mediate central tolerance though trafficking of host APC from the periphery into the thymus. Support for this idea comes from recent work that showed that approximately 50% of dendritic cells in the adult thymus are derived from a circulating pool of dendritic cells of peripheral origin.40,41 Furthermore, a few donor Treg cells are found in the thymus of adoptively transferred IL-2R⫺/⫺ mice (D.A. and T.R.M., unpublished data, August 2006). These cells provide another source of donor alloantigens for transfer to resident thymic APCs to mediate negative selection of T cells. With respect to alloantigen recognition, our results demonstrated that there must be an exact genetic match between the transferred donor Treg cells and the skin graft for the most long-lasting allograft retention. As illustrated by the use of B6bm3, B6bm12, and BALB.B skin grafts or donor Treg cells, any mismatch in a single class I or class II molecule or in minor non-MHC alloantigens between the donor Treg cells and skin graft ultimately resulted in graft rejection. Nevertheless, in all these aforementioned settings, where there was substantial but not complete matching between the donor Treg cells and the skin allografts, there was a significant delay in rejection of these grafts in comparison with third-party C3H allografts. This finding is consistent with an important dominant suppressive mechanism by Treg cells in skin graft tolerance. This “partial” tolerance may reflect suppressive mechanisms by donor Treg cells that recognize the shared alloantigens of the allograft or represent a cross-reaction to the mismatched alloantigens of the graft. Treg cells need to be activated via the TCR to exert suppression.42 Thus, the observation that long-lasting allogeneic Treg cells mediated skin graft tolerance by the use of skin from MHC class II–deficient mice indicates that there is not an absolute requirement for the Treg cells to become activated within the graft by skin-derived APCs for the immune tolerance observed. Furthermore, tolerance to MHC class II–deficient skin cannot be the result of failed direct class II recognition by alloreactive effector cells because B6 class II⫺/⫺ skin was readily rejected by controls, particularly BALB/c Treg3BALB/c⫺/⫺. Efficient tolerance to allogeneic class II⫺/⫺ skin grafts further points to the importance of indirect antigen presentation not only for central deletion of potential graft rejecting cells but for activation of the suppressive Treg cells. This finding, however, does not rule out that direct recognition of donor class II by Treg cells may be operative in class II–sufficient skin grafts, which may complement the activity of From www.bloodjournal.org by guest on June 18, 2017. For personal use only. BLOOD, 11 MARCH 2010 䡠 VOLUME 115, NUMBER 10 LONG-TERM ALLOTOLERANCE AND DONOR Treg CELLS those Treg cells that indirectly recognized donor antigens. Furthermore, tolerance to B6 class II⫺/⫺ allografts indicates that the requirement for exact matching between the allogeneic Treg cells and allo-skin grafts cannot be attributable to the Treg cells simply “remembering” the MHC class II molecules on which they were initially selected during their thymic development before adoptive transfer. Thus, it is likely that indirect presentation of Treg cell-derived allopeptides from donor Treg cells not only function for inducing negative selection in the thymus but also to select/ activate at least a subset of the adoptively transferred engrafting donor Treg cells. In summary, our findings to date indicate that long-lasting allograft tolerance by allogeneic Treg cells in IL-2R⫺/⫺ mice depends on the following factors: (1) a substantial empty niche to promote engraftment of the transferred Treg cells; (2) indirect presentation of donor Treg cell–derived alloantigens that promote some thymic negative selection of developing alloreactive T cells and peripheral selection of suppressive Treg cells with TCRs directed to such alloantigens; and (3) genetic identity between the donor allogeneic Treg cells and the skin allografts. Besides these points, there are several additional issues to consider. First, the impaired T effector and perhaps memory responses associated with the IL-2R–deficient genetic background34-36 dampen the allograft rejection response, which may facilitate Treg cell-mediated tolerance. Second, all Treg cell-adoptive transfers, by necessity to prevent autoimmunity, were performed by the use of neonatal IL-2R⫺/⫺ recipients. The neonatal environment is particular permissive to induce immune tolerance43-45 and represents a setting related to early post–hematopoietic stem cell (HSC) transfers. Finally, IL-2R–deficient mice lack natural killer (NK) and NK T cells.34 The lack of these cells, especially NK cells, diminishes the potential to eliminate transplanted allogeneic donor Treg cells and rejection of MHC class-I negative allografts.46,47 These findings raise the intriguing possibility that clinical scenarios that emulate the IL-2R–deficient model may enable engraftment of allogeneic Treg cells and tolerance toward solid tissues or HSC allografts. Identical genetic matching between donor Treg cells and the transplanted tissues is readily accomplished simply by isolating Treg cells from the peripheral blood of the same donor of the transplanted organ or tissue, such as progenitor cell allografts. Meeting the other key factors may require conditioning of the recipient to facilitate Treg cell engraftment. For example, reduction of recipient Treg cells after conditioning/chemotherapy before organ or HSC transfer, together with intentional deletion of residual Treg cells, may provide a niche for 1939 the allogeneic Treg cell infusion. Application of less-vigorous generalized immunosuppression, perhaps analogous to IL-2R deficiency, to dampen rejection responses to allogeneic-Treg cells and the allografts also may be beneficial. Inhibiting the IL-2R in effector cells should not prevent immune responses against infectious agents because effective immunity occurs in the absence of IL-2/IL-2R.35,48 Thus, immunosuppression in conjunction with Treg cells may not need to be as robust as currently practiced. On the basis of our data, once substantial stable allogeneic Treg cell chimerism is achieved, graft-specific peripheral and central tolerance is vigorously promoted, which may permit suspension of drug-mediated immunosuppression. Several of the favorable conditions facilitating tolerance in the IL-2R–deficient model also appear to be operative in suppression of GVHD by allogeneic Treg cells. Not only does exact matching of the allo-Treg cells to the bone marrow transplant occur, but the lymphopenic setting during marrow reconstitution leads to an environment that favors donor Treg engraftment and persistence to readily suppress autoaggressive donor-derived T cells. Furthermore, the immunosuppressive drug rapamycin synergizes with allo-Treg cells to enhance inhibition of alloresponses after HSC transplantation.49,50 These similarities emphasize the value of elaborating the mechanisms for the robust immune tolerance in Treg cell transferred IL-2R⫺/⫺ mice as such understanding should help better define the conditions required for successful adoptive immunotherapy. Acknowledgments This work was supported by National Institutes of Health grant R01AI055815. Authorship Contribution: D.A. designed and performed experiments, analyzed data, and wrote the paper; R.B.L. analyzed the data and edited the paper; and T.R.M. designed experiments, analyzed data, and wrote the paper. Conflict-of-interest disclosure: The authors declare no competing financial interests. Correspondence: Dr Thomas Malek, Department of Microbiology and Immunology (R138), Miller School of Medicine, University of Miami, 1600 NW 10th Ave, Miami, FL 33136; e-mail: [email protected]. References 1. Sakaguchi S, Ono M, Setoguchi R, et al. Foxp3⫹ CD25⫹ CD4⫹ natural regulatory T cells in dominant self-tolerance and autoimmune disease. Immunol Rev. 2006;212:8-27. 2. Beyer M, Schultze JL. Regulatory T cells in cancer. Blood. 2006;108(3):804-811. 3. Belkaid Y. Regulatory T cells and infection: a dangerous necessity. Nat Rev Immunol. 2007;7(11): 875-888. 4. Hoffmann P, Ermann J, Edinger M, Fathman CG, Strober S. Donor-type CD4⫹CD25⫹ regulatory T cells suppress lethal acute graft-versus-host disease after allogeneic bone marrow transplantation. J Exp Med. 2002;196(3):389-399. 5. Cohen JL, Trenado A, Vasey D, Klatzmann D, Salomon BL. CD4⫹CD25⫹ immunoregulatory T cells: new therapeutics for graft-versus-host disease. J Exp Med. 2002;196(3):401-406. 6. Edinger M, Hoffmann P, Ermann J, et al. CD4⫹CD25⫹ regulatory T cells preserve graftversus-tumor activity while inhibiting graft-versushost disease after bone marrow transplantation. Nat Med. 2003;9(9):1144-1150. 7. Trenado A, Charlotte F, Fisson S, et al. Recipienttype specific CD4⫹CD25⫹ regulatory T cells favor immune reconstitution and control graft-versushost disease while maintaining graft-versusleukemia. J Clin Invest. 2003;112(11):1688-1696. 8. Hanash AM, Levy RB. Donor CD4⫹CD25⫹ T cells promote engraftment and tolerance following MHC-mismatched hematopoietic cell transplantation. Blood. 2005;105(4):1828-1836. 9. Sakaguchi S, Sakaguchi N, Asano M, Itoh M, Toda M. Immunologic self-tolerance maintained by activated T cells expressing IL-2 receptor ␣ -chains (CD25). Breakdown of a single mechanism of self-tolerance causes various autoim- mune diseases. J Immunol. 1995;155(3):11511164. 10. Almeida AR, Legrand N, Papiernik M, Freitas AA. Homeostasis of peripheral CD4⫹ T cells: IL-2R␣ and IL-2 shape a population of regulatory cells that controls CD4⫹ T-cell numbers. J Immunol. 2002;169(9):4850-4860. 11. Wolf M, Schimpl A, Hunig T. Control of T-cell hyperactivation in IL-2-deficient mice by CD4⫹CD25⫺ and CD4⫹CD25⫹ T cells: evidence for two distinct regulatory mechanisms. Eur J Immunol. 2001;31(6):1637-1645. 12. Malek TR, Yu A, Vincek V, Scibelli P, Kong L. CD4 regulatory T cells prevent lethal autoimmunity in IL-2R-deficient mice. Implications for the nonredundant function of IL-2. Immunity. 2002;17(2): 167-178. 13. Joffre O, Santolaria T, Calise D, et al. Prevention From www.bloodjournal.org by guest on June 18, 2017. For personal use only. 1940 BLOOD, 11 MARCH 2010 䡠 VOLUME 115, NUMBER 10 ADEEGBE et al of acute and chronic allograft rejection with CD4⫹CD25⫹Foxp3⫹ regulatory T lymphocytes. Nat Med. 2008;14(1):88-92. 14. Kingsley CI, Karim M, Bushell AR, Wood KJ. CD25⫹CD4⫹ regulatory T cells prevent graft rejection: CTLA-4– and IL-10–dependent immunoregulation of alloresponses. J Immunol. 2002; 168(3):1080-1086. 15. Bluestone JA, Tang Q, Sedwick CE. T regulatory cells in autoimmune diabetes: past challenges, future prospects. J Clin Immunol. 2008;28(6): 677-684. 16. Wood KJ, Sakaguchi S. Regulatory T cells in transplantation tolerance. Nat Rev Immunol. 2003;3(3):199-210. 17. Ochando JC, Homma C, Yang Y, et al. Alloantigenpresenting plasmacytoid dendritic cells mediate tolerance to vascularized grafts. Nat Immunol. 2006;7(6): 652-662. 18. Waldmann H, Chen TC, Graca L, et al. Regulatory T cells in transplantation. Semin Immunol. 2006;18(2):111-119. 19. Sánchez-Fueyo A, Domenig CM, Mariat C, Alexopoulos S, Zheng XX, Strom TB. Influence of direct and indirect allorecognition pathways on CD4⫹CD25⫹ regulatory T-cell function in transplantation. Transpl Int. 2007;20(6):534-541. 20. Gökmen MR, Lombardi G, Lechler RI. The importance of the indirect pathway of allorecognition in clinical transplantation. Curr Opin Immunol. 2008; 20(5):568-574. 21. Tsang JY, Tanriver Y, Jiang S, et al. Conferring indirect allospecificity on CD4⫹CD25⫹ Tregs by TCR gene transfer favors transplantation tolerance in mice. J Clin Invest. 2008;118(11):36193628. 22. Nguyen VH, Zeiser R, Negrin RS. Role of naturally arising regulatory T cells in hematopoietic cell transplantation. Biol Blood Marrow Transplant. 2006;12(10):995-1009. 23. Taylor PA, Lees CJ, Blazar BR. The infusion of ex vivo activated and expanded CD4⫹CD25⫹ immune regulatory cells inhibits graft-versus-host disease lethality. Blood. 2002;99(10):3493-3499. 24. Riley JL, June CH, Blazar BR. Human T regulatory cell therapy: take a billion or so and call me in the morning. Immunity. 2009;30(5):656-665. 25. Adeegbe D, Bayer AL, Levy RB, Malek TR. Cutting edge: allogeneic CD4⫹CD25⫹Foxp3⫹ T regulatory cells suppress autoimmunity while establishing transplantation tolerance. J Immunol. 2006;176(12):7149-7153. 26. Bayer AL, Yu A, Adeegbe D, Malek TR. Essential role for interleukin-2 for CD4⫹CD25⫹ T regulatory cell development during the neonatal period. J Exp Med. 2005;201(5):769-777. 27. Suzuki H, Kundig TM, Furlonger C, et al. Deregulated T-cell activation and autoimmunity in mice lacking interleukin-2 receptor . Science. 1995; 268(5216):1472-1476. 28. Isakov N, Bach FH. Thyroid graft rejection between C57BL/6 and H-2Kb mutant mice. Differences in the immunogenic expression of the mutated molecule on thyroids of six different mutants. Transplantation. 1983;36(5):571-577. 29. McIntyre KR, Seidman JG. Nucleotide sequence of mutant I-A bm12 gene is evidence for genetic exchange between mouse immune response genes. Nature. 1984;308(5959):551-553. 30. Koller BH, Marrack P, Kappler JW, Smithies O. Normal development of mice deficient in  2M, MHC class I proteins, and CD8⫹ T cells. Science. 1990;248(4960):1227-1230. 31. Kohm AP, Carpentier PA, Anger HA, Miller SD. Cutting edge: CD4⫹CD25⫹ regulatory T cells suppress antigen-specific autoreactive immune responses and central nervous system inflammation during active experimental autoimmune encephalomyelitis. J Immunol. 2002;169(9):47124716. 32. Lee MKt Moore DJ, Jarrett BP, et al. Promotion of allograft survival by CD4⫹CD25⫹ regulatory T cells: evidence for in vivo inhibition of effector cell proliferation. J Immunol. 2004;172(11):65396544. 33. Zwar TD, Read S, van Driel IR, Gleeson PA. CD4⫹CD25⫹ regulatory T cells inhibit the antigen-dependent expansion of self-reactive T cells in vivo. J Immunol. 2006;176(3):16091617. 34. Malek TR, Porter BO, Codias EK, Scibelli P, Yu A. Normal lymphoid homeostasis and lack of lethal autoimmunity in mice containing mature T cells with severely impaired IL-2 receptors. J Immunol. 2000;164(6):2905-2914. 35. Yu A, Zhou J, Marten N, et al. Efficient induction of primary and secondary T cell-dependent immune responses in vivo in the absence of functional IL-2 and IL-15 receptors. J Immunol. 2003; 170(1):236-242. 36. Malek TR, Yu A, Scibelli P, Lichtenheld MG, Codias EK. Broad programming by IL-2 receptor signaling for extended growth to multiple cytokines and functional maturation of antigenactivated T cells. J Immunol. 2001;166(3):16751683. 37. Nishimura E, Sakihama T, Setoguchi R, Tanaka K, Sakaguchi S. Induction of antigen-specific immunologic tolerance by in vivo and in vitro antigen-specific expansion of naturally arising Foxp3⫹CD25⫹CD4⫹ regulatory T cells. Int Immunol. 2004;16(8):1189-1201. 38. Golshayan D, Jiang S, Tsang J, Garin MI, Mottet C, Lechler RI. In vitro-expanded donor alloantigen-specific CD4⫹CD25⫹ regulatory T cells promote experimental transplantation tolerance. Blood. 2007;109(2):827-835. 39. Bayer AL, Yu A, Malek TR. Function of the IL-2R for thymic and peripheral CD4⫹CD25⫹ Foxp3⫹ T regulatory cells. J Immunol. 2007;178(7):40624071. 40. Bonasio R, Scimone ML, Schaerli P, Grabie N, Lichtman AH, von Andrian UH. Clonal deletion of thymocytes by circulating dendritic cells homing to the thymus. Nat Immunol. 2006;7(10):10921100. 41. Li J, Park J, Foss D, Goldschneider I. Thymushoming peripheral dendritic cells constitute two of the three major subsets of dendritic cells in the steady-state thymus. J Exp Med. 2009;206(3): 607-622. 42. Thornton AM, Shevach EM. CD4⫹CD25⫹ immunoregulatory T cells suppress polyclonal T-cell activation in vitro by inhibiting interleukin 2 production. J Exp Med. 1998;188(2):287-296. 43. Donckier V, Wissing M, Bruyns C, et al. Critical role of interleukin 4 in the induction of neonatal transplantation tolerance. Transplantation. 1995; 59(11):1571-1576. 44. Gao Q, Chen N, Rouse TM, Field EH. The role of interleukin-4 in the induction phase of allogeneic neonatal tolerance. Transplantation. 1996;62(12): 1847-1854. 45. Adkins B, Leclerc C, Marshall-Clarke S. Neonatal adaptive immunity comes of age. Nat Rev Immunol. 2004;4(7):553-564. 46. Ito A, Shimura H, Nitahara A, et al. NK cells contribute to the skin graft rejection promoted by CD4⫹ T cells activated through the indirect allorecognition pathway. Int Immunol. 2008;20(10): 1343-1349. 47. Hsieh CL, Obara H, Ogura Y, Martinez OM, Krams SM. NK cells and transplantation. Transpl Immunol. 2002;9(2-4):111-114. 48. Malek TR, Bayer AL. Tolerance, not immunity, crucially depends on IL-2. Nat Rev Immunol. 2004;4(9):665-674. 49. Steiner D, Brunicki N, Bachar-Lustig E, Taylor PA, Blazar BR, Reisner Y. Overcoming T-cell– mediated rejection of bone marrow allografts by T-regulatory cells: synergism with veto cells and rapamycin. Exp Hematol. 2006;34(6):802-808. 50. Zeiser R, Leveson-Gower DB, Zambricki EA, et al. Differential impact of mammalian target of rapamycin inhibition on CD4⫹CD25⫹Foxp3⫹ regulatory T cells compared with conventional CD4⫹ T cells. Blood. 2008;111(1):453-462. From www.bloodjournal.org by guest on June 18, 2017. For personal use only. 2010 115: 1932-1940 doi:10.1182/blood-2009-08-238584 originally published online December 29, 2009 Allogeneic T regulatory cell−mediated transplantation tolerance in adoptive therapy depends on dominant peripheral suppression and central tolerance Dennis Adeegbe, Robert B. Levy and Thomas R. Malek Updated information and services can be found at: http://www.bloodjournal.org/content/115/10/1932.full.html Articles on similar topics can be found in the following Blood collections Immunobiology (5489 articles) Information about reproducing this article in parts or in its entirety may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests Information about ordering reprints may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#reprints Information about subscriptions and ASH membership may be found online at: http://www.bloodjournal.org/site/subscriptions/index.xhtml Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036. Copyright 2011 by The American Society of Hematology; all rights reserved.