Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
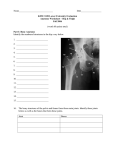
HIP ANATOMY The Joint The hip or coxafemoral joint includes the concave acetabulum of the innominate of the pelvis and the convex head of the femur (1) (Table 12.1). Structurally, the hip is a very stable joint, supported by one of the strongest ligament systems in the body and a very deep acetabulum. Further stability is added by the contribution of the fibrocartilaginous acetabular labrum (1), which deepens the acetabulum for greater congruency. The semi-circular–shaped acetabular labrum is a fibrocartilaginous rim that attaches to the outer border of the acetabulum, an element that decreases the friction of the joint surfaces (2). The transverse ligament completes the ‘circle’ of the labrum and functions as an attachment site for the ligamentum teres. The labrum is much thicker medially, superiorly, and posteriorly than anteriorly, thus predisposing the anterior labrum to tears. The joint capsule attaches to the labrum, is integrated with the ligamentous structures, and has an attachment to the rectus femoris muscle (2). Table 12.1: General Information Regarding the Hip Region. Concept Information Bones Composed of 4 bones: 3 from the innominate (the ilium, ischium, and pubis), which integrates to form the acetabulum and the single femur Lumbopelvic rhythm • • Femur • • • • Ipsilateral lumbopelvic rhythm—the L/S and the pelvis rotate in the same direction, as in forward bending from the waist Contralateral lumbopelvic rhythm—the L/S and the pelvis rotate in opposite directions. The supralumbar trunk (the body above L1) can remain stationary as the pelvis rotates over the femurs. This occurs with walking or other activities where the head and eyes need to be held fixed in space independent of the rotation of the pelvis The femur is the longest and strongest bone in the body and has a slight anterior convexity (bowing) to allow greater loading The femur has a thick shell of dense, compact bone, which is able to resist large external loads and a core of cancellous bone that absorbs external loads The femoral head forms 2/3 of a perfect sphere and is covered by articular cartilage, which is thickest anterior and above the fovea. There is approximately 125° or femoral head inclination and 15° of normal anteversion Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ Acetabulum The acetabulum has a 20° anterior orientation. There is an acetabular ring of fibrocartilage. The acetabular cartilage is thickest along the superior-anterior margin Theoretical resting position Theoretical close-pack position Theoretical capsular pattern Resting position = 30° flexion, 30° abduction, and slight external rotation Close-pack position = extension, internal Rotation, and abduction Capsular pattern = internal rotation, flexion, abduction, and external rotation The hip is unlike the shoulder in the fact that the amount of accessory motion outside of distraction is minimal (3). Normal arthrokinematic movements such as those associated with glide and slide are finite, a consequence of structure and function. Osseous Structures Four bones make up the coxafemoral joint; 1) the femur, 2) the pubis, 3) the ischium, and 4) the ilium. The innominate bones are composed of the ilium, the pubis, and the ischium. The ilium is the superior-most osseous structure of the innominate that forms the articulation with the sacrum and two-fifths of the surface of the acetabulum (4). The pubis is the inferomedial aspect of the innominate and constitutes one-fifth of the articulation with the acetabulum of the hip. The ischium is the inferolateral aspect of the innominate that provides the floor of the acetabulum and the posterior two-fifths of the articular surface of the acetabulum rim. The acetabulum is covered in hyaline cartilage. The femur is a very large and stable long bone that is further subdivided into the head, neck, and trochanteric regions. The spherical head is directed cranially and medially, and slightly anterior. The surface of the head of the femur is covered with hyaline cartilage for smooth contact with the acetabulum. The neck of the femur connects the head of the femur with the shaft and is angled about 125 degrees in an adult. Over time during growth, the angle decreases and varies greatly among individuals. The trochanteric region includes the greater and lesser trochanters, attachment sites for several muscles of the hip region. The greater trochanter is situated lateral and posterior and is Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ caudal to the neck of the femur. The tendons of the gluteus medius, and to some extent the gluteus maximus, insert on the lateral aspect of the greater trochanter, which also serves as the location for the intertrochanteric bursae. The medial aspect is the attachment site for the tendons of the obturator externus, the obturator internus, the gemelli, the gluteus minimus, and the piriformis. The inferior aspect of the medial greater trochanter gives origin to the upper part of the vastus lateralis. The lesser trochanter serves as the insertion site for the iliacus and the psoas major (5). Ligaments and Capsule There are several major ligaments of the hip, the most prominent being the Y ligament of Bigelow. The Y ligament of Bigelow provides anterior ligamentous support. The Y ligament of Bigelow originates from the anterior inferior iliac spine of the pelvis and attaches to the intertrochanteric line of the femur. The ligament was given the name “Y” because the bifurcation of the two ligaments looks like an inverted Y. The ligaments support the anterior aspect of the capsule and provide stabilization against excessive extension-based movements. The Y ligament of Bigelow is considered the strongest single ligament within the body. The pubofemoral ligament connects the pubic ramus to the intertrochanteric line and limits abduction while providing some extension support (6). The ligament extends across the antero-inferior aspect of the joint to blend with the iliolumbar ligament. Because of the orientation of the fibers, the ligament also assists in preventing excess abduction (6). This ligament reinforces the hip capsule and adds to the strength during end-range movements. The ischiofemoral ligament, the thinnest of the hip ligaments, extends from the posterior acetabular rim to the inner surface of the greater trochanter of the femur (6). Primarily, the ligament stabilizes the hip in full extension. Similar to the iliolumbar ligament and the pubofemoral ligament, the ischiofemoral ligament is tightened during internal rotation and reinforces the hip capsule. Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ The ligamentum teres is a flat, triangular-shaped ligament that arises from the base of the transverse acetabular ligament of the acetabulum and inserts into the head of the femur. In conjunction with the hip capsule, the ligamentum teres limits functional distraction of the hip joint and may have some stabilizing effect. The ligament is tensioned when the thigh is semi-flexed, adducted, or externally rotated and is relaxed when the limb is abducted. The teres ligament provides a conduit for the medial and lateral circumflex arteries and supplies the femur with blood and nutrients. Figure 12.1: The Ligaments of the Hip The hip capsule is fibrous and encloses the hip joint. The anterior attachment sites include the acetabulum and the neck of the femur at the intertrochanteric line. Posteriorly, the lateral aspect of the femoral neck is extracapsular and medial. The posterior capsule is attached to the acetabulum and pubic ramis. The anterior ligament, which arises above the anterior superior iliac spine (ASIS) and adjacent to the acetabulum, reinforces the capsule with a component of the iliofemoral ligament and the aforementioned ischiofemoral and pubofemoral ligaments. The contribution of the ligaments to the capsule often tightens the ligament during extension and occasionally during internal rotation. Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ Muscles The largest forces at the hip are a result of muscular contraction (7), specifically those required during single-leg stance (Table 12.2). Crowninshield and Brand (8) report that an activity such as the single-leg stance, in which the ipsilateral gluteus medius is forced to contract to stabilize the pelvis, leads to compression forces three to four times the body weight. Others have projected the force at six times the person’s body weight (1). Table 12.2: The Muscles of the Hip. Location Anterior Posterior Medial Lateral Muscle Sartorius Rectus femoris Psoas major Iliacus Gluteus maximus Hamstrings Gracilis Hip adductor group Gluteus medius Gluteus minimus Function Hip flexion, abduction and external rotation Hip flexion and knee extension Hip flexion and lumbar compression Hip flexion Hip extension Hip extension and knee flexion Primarily hip adduction Hip adduction Hip abduction and pelvic stabilization during unilateral stance Hip abduction Dividing the muscle into regions more effectively aids in describing the multiple muscles of the hip. The regions are subdivided into the anterior, medial, lateral, and posterior musculature. The anterior musculature includes the rectus femoris, sartorius, and the iliopsoas group. Medially, the musculature consists of the adductor group, including the pectineus and the gracilis. Numerous muscles comprise the lateral musculature of the hip including the gluteus medius, tensor fasciae latae (TFL), piriformis, quadratus femoris, obturator internus, obturator externus, gemellus superior, and gemellus inferior. Lastly, the posterior muscles include the primary muscle group responsible for hip extension such as the gluteus maximus and hamstrings. Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ Bursae There are four primary bursae at the hip. Two bursae are of special interest because they are commonly involved in pathology. The trochanteric bursa is located on the side of the hip near the posterior aspect of the greater tubercle. The trochanteric bursa normally functions to increase lubrication of the hip abductors, but when pathological, may cause a dull, burning pain on the outer hip that is worsened with abduction or squatting. The ischial bursa (not pictured) is located in the posterior buttock region and lies over the ischial tuberosity. The ischial bursa may cause dull pain in the buttock region that is most noticeable climbing up hill and is generally worsened during sitting, specifically in firm-seated chairs (5). Figure 12.2: Anterior and Lateral Bursae of the Hip Summary • • • • The hip joint consists of the femur, the three bones that make up the innominate, and the surrounding ligaments and muscles. The hip joint is a deep-set ball-and-socket joint that sacrifices mobility for stability. The capsular-ligamentous system of the hip creates the most stable synovial joint system within the body. Of the numerous muscles that surround the hip, two primary stabilizers, the gluteus medius and the gluteus maximus, play a considerable role during gait and function. Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ BIOMECHANICS Cyriax (11) and Kaltenborn (12) outlined the existence of a capsular pattern during early stages of osteoarthritis and other forms of hip capsule trauma. Cyriax (11) proposed the loss of internal rotation typically proceeded flexion, abduction, then extension, and that external rotation loss was rare. He (11) and Kaltenborn (12), as well as other manual therapy disciplines, have advocated the use of capsular patterns for both examination and treatment. These theories were based on clinical experience and ‘perception’ versus experimental analyses. Recently, two experimental studies (13,14) have refuted the existence of a definable hip capsular pattern, suggesting that the existence of a single capsular pattern in patients with early or progressive stages of osteoarthritis does not exist. Others have also reported gross range-ofmotion losses, nonpatterned in external and internal rotation, as well as abduction in osteoarthritis conditions (15). Based on these findings, examination and treatment based on capsular pattern could provide inconsistent, unreliable, and subsequently invalid results. Although the use of a capsular pattern has been documented as helpful in a series of case studies, the use of this method in examination is excluded as a component of this chapter because it appears highly variable. Additionally, even though occasional range-of-motion variations (i.e., internal range-ofmotion loss with osteoarthritis) provide some benefit during examination for selected pathologies, this pattern appears to lack reliability to overlay all like-type disorders. Using a nationwide database, Roach and Miles (16) reported normative values for the combined age groups of 25 through 74. The following values of 121 degrees of hip flexion, 19 degrees of hip extension, 42 degrees of hip abduction, 32 degrees of internal rotation, and 32 degrees of external rotation closely reflect those of Hoppenfeld (17) but differ from those of Kendall et al. (18) and Daniels and Worthingham (19). What was interesting regarding the findings was that the values associated with all ranges declined with age, although those with hip flexion declined only minimally. Along with planar movements, the hip can also move in combined motions of circumduction, which is a movement combination of variations of plane-based motions (Table Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ 12.3). The benefit of combined motions during examination and treatment is that the structures assume a more compromised and tightened position and may provide more discriminatory results. Specifically, combined movements should be examined if no mechanically based painful findings are extracted from the initial examination. Table 12.3: Hip Range-of-Motion Movements and Methods of Limiting Movement. Motion Movement Restricting Elements Flexion Abduction 80° with knee extended 120° with knee flexed 20° with knee extended 0° with knee flexed 40° Adduction 25° IR ER 35° 45° Hamstrings and gracilis Ischiofemoral ligament and inferior capsule Iliofemoral ligament and anterior capsule Rectus femoris Pubofemoral ligament, inferior capsule, adductor, and hamstrings Ischiofemoral ligament, IT band, and abductor muscles Ischiofemoral ligament and ER muscles Iliofemoral ligament, IT band, and IR muscles Extension Summary • • Little evidence exists to support Cyriax’s theory of capsular pattern. To date, there are no studies that have verified a consistent pattern of range-of-motion loss at the hip. Roach and Miles outlined the following normative values for range of motion at the hip: 121 degrees of hip flexion, 19 degrees of hip extension, 42 degrees of hip abduction, 32 degrees of internal rotation, and 32 degrees of external rotation. Online References 1. 2. 3. 4. 5. 6. 7. 8. Anderson, MK; Hall, SJ; Martin M. Sports injury management. Philadelphia; Lippincott Williams & Wilkins: 2000. Starkey C, Ryan J. Evaluation of orthopedic and athletic injuries. Philadelphia; F.A. Davis Company: 1996. Williams P, Bannister L. In: Berry M, Collins P. Dyson M, Dussek J, Ferguson M (eds.) Gray’s anatomy, 38th ed. Edinburgh; Churchill Livingstone: 1995. Lee D. The pelvic girdle. An approach to the examination and treatment of the lumbopelvic-hip region. Edinburgh; Churchill Livingstone: 1989. Gross J. Musculoskeletal examination. Malden, Mass; Blackwell Pub: 2002. Nicholas J, Hershman E. The lower extremity and spine in sports medicine. Vol 2. St. Louis; Mosby Co: 1986. Sims K. Assessment and treatment of hip osteoarthritis. Man Ther. 1999;4:136–144. Crowninshield R, Brand R, A physiologically based criterion of muscle force prediction in locomotion. J Biomechanics. 1981;14:793–801. Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. Bogduk N, Macintosh JE, Pearcy MJ. A universal model of the lumbar back muscles in the upright position. Spine. 1992;17(8):897–913. Delp S, Hess W, Hungerford D, Jones L. Variation of rotation moment arms with hip flexion. J Biomech. 1999;32:493–501. th Cyriax J. Textbook of orthopaedic medicine. 7 ed. Vol. 1. London; Baillierre Tindall: 1978. th Kaltenborn F. Manual mobilization of the extremity joints. 4 ed. Olaf Norlis Bokhandel; Oslo: 1989. Klassbo M, Harms-Ringdahl K, Larsson G. Examination of passive ROM and capsular patterns in the hip. Physiother Res Int. 2003;8(1):1–12. Bijl D, Dekker J, van Baar ME, Oostendorp RA, Lemmens AM, Bijlsma JW, Voorn TB. Validity of Cyriax’s concept capsular pattern for the diagnosis of osteoarthritis of hip and/or knee. Scand J Rheumatol. 1998;27(5):347–351. Arokoski MH, Haara M, Helminen HJ, Arokoski JP. Physical function in men with and without hip osteoarthritis. Arch Phys Med Rehabil. 2004;85(4):574–581. Roach K, Miles T. Normal hip and knee active range of motion: The relationship to age. Phys Ther.1991;71:656–665. Hoppenfeld S. Physical examination of the spine and extremities. New York; AppletonCentury-Crofts: 1976. nd Kendall H, Kendall F, Wadsworth G. Muscles: testing and function. 2 ed. Baltimore; Williams & Wilkins: 1971. rd Daniels L, Worthingham C. Muscle testing techniques of manual examination. 3 ed. Philadelphia; WB Saunders: 1972. Cook, Orthopedic Manual Therapy: An Evidence-Based Approach, 2/E © 2012 by Pearson Education, Inc., Upper Saddle River, NJ