Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Electrocardiography wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Cardiac arrest wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
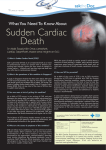
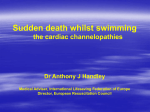
UvA-DARE (Digital Academic Repository) Subtle killers and sudden death: Genetic variants modulating ventricular fibrillation in the setting of myocardial infarction Pazoki, R. Link to publication Citation for published version (APA): Pazoki, R. (2015). Subtle killers and sudden death: Genetic variants modulating ventricular fibrillation in the setting of myocardial infarction General rights It is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons). Disclaimer/Complaints regulations If you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, stating your reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Ask the Library: http://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam, The Netherlands. You will be contacted as soon as possible. UvA-DARE is a service provided by the library of the University of Amsterdam (http://dare.uva.nl) Download date: 18 Jun 2017 Chapter 3 Complex inheritance for susceptibility to sudden cardiac death Curr Pharm Des. 2013;19(39):6864-72. Raha Pazoki, Michael W.T. Tanck, Arthur A.M. Wilde, Connie R. Bezzina 34 Chapter 3 Abstract Sudden cardiac death (SCD) from ventricular fibrillation during myocardial infarction is a leading cause of total and cardiovascular mortality. It has a multifactorial, complex nature and aggregates in families, implicating the involvement of heritable factors in the determination of risk. During the last few years, genome-wide association studies have uncovered common genetic variants modulating risk of SCD. We here review the current insight on genetic determinants of SCD in the community and describe the genome-wide association approaches undertaken thus far in uncovering genetic determinants of SCD risk. Complex inheritance for susceptibility to sudden cardiac death 35 Sudden death (SD) is defined as natural, unexpected death within an hour of the onset of symptoms and can be due to cardiac or non-cardiac causes (e.g. stroke or aneurysm) 1. The annual incidence of SD in the general population (20-75 years of age) is 1 per 1000 individuals, accounting for 18.5% of total mortality 1,2. SD is a rare event in young individuals 3,4; the incidence is 1.3-8.5 per 100,000 individuals younger than 40 years of age 1,3. The major proportion of SD is considered to be sudden cardiac death (SCD). In Europe and North America, SCD accounts for 50-100 deaths each year per 100,000 individuals in the general population 5,6. The incidence of SCD is 1 in 100,000 individuals in the young population (age < 35-40) and 1 in 1,000 in the older segment (age > 35-40) of the population 6. Overall mortality of patients with sudden cardiac arrest, even in regions of the world with an advanced first responder system and resuscitation methodology, is more than 95% 6,7 Survival to hospital discharge for those cases who present with witnessed ventricular fibrillation (VF) or ventricular tachycardia (VT) is around 29% 8. SCD accounts for a major proportion of all cardiovascular deaths (up to 50%) 9. In fact, SCD is the fatal manifestation of a group of cardiac arrhythmias including VT, VF or severe bradyarrhythmia 7. The most common electrophysiological disorder underlying SCD is VF (Figure 1), which subsequently and ultimately degenerates to asystole 10. Ventricular arrhythmia present with various symptoms including palpitations, chest pain, or syncope and can lead to SCD within a few minutes 7. The underlying cardiac disorder is often not diagnosed before the event and in 40-50% of all SCD cases no symptoms precede the death 7,8,11. SCD may occur in a broad range of pathological settings such as coronary artery disease (CAD), cardiomyopathy, congenital heart disease, inflammatory myocardial Figure 1 | Three lead ECG (II, I and III) displaying acute ischemia-related VF. The patient concerned Figure 1 | Three-lead ECG (II, I and III) displaying acute ischemia-related VF. The patient conhas an acute inferior wall MI (ST elevation in leads II and III). An R-on-T extrasystole in the third ST-T cerned has anrise acute inferior wall segment gives to immediate VF.MI (ST elevation in leads II and III). An R-on-T extrasystole in the third ST-T segment gives rise to immediate VF. SCD may occur in a broad range of pathological settings such as coronary artery disease (CAD), cardiomyopathy, congenital heart disease, inflammatory myocardial disease, or even, sudden unexplained death, in the structurally normal heart. However, the Chapter 3 Introduction 3 36 Chapter 3 • LVEF <30–35% • LVH • Aortic stenosis Non-modifiable factors Modifiable factors • HTN • Diabetes • Prolonged QT interval SCD • Structural disorders of the heart (HCM, ARVC, etc.) • Primary electrical disorders (LQTs,BrS, SSS, etc.) Mendelian Inheritance Complex Inheritance • CVD/CAD/ MI • Family history of SCD Figure 2 | Predisposing factors to sudden cardiac death. SCD, sudden cardiac death; LVH, left ventricular hypertrophy; LVEF, left ventricular ejection fraction; HTN, hypertension; HCM, hyperthrophic cardiomyopathy; ARVC, arrhythmogenic right ventricular cardiomyopathy; LQTS, long QT syndrome; BrS, Brugada syndrome; SSS, sick sinus syndrome; CVD, cardiovascular diseases; CAD, coronary artery disease; MI, myocardial infarction. disease, or even, sudden unexplained death, in the structurally normal heart. However, the overwhelming majority (~80%) 11 of SCDs occur in older individuals and are largely caused by sequela of CAD, namely in the setting of acute or previous myocardial ischemia / infarction and heart failure 12. Acute myocardial infarction (MI) is the most important source for ventricular arrhythmias 13 including VF, VT, and ventricular premature depolarization. Several factors have been mentioned to be associated with SCD in the setting of CAD (Figure 2). These factors include left ventricular ejection fraction (LVEF), left ventricular hypertrophy, prolonged QTc interval, Diabetes, and hypertension 7. Up until now, LVEF is the only factor that is used for risk stratification of SCD. Patients with LVEF of less than 30–35% are considered to be at high risk for SCD and eligible for prophylactic implantation of a cardiac defibrillator 7,14. Mechanism of arrhythmia in the setting of acute myocardial ischemia In animal models, ventricular arrhythmias mainly occur during the first 30 minutes of the experimental ischemia and in two distinct periods 13. The early phase (phase 1a) occurs from 2 to 10 minutes after the coronary occlusion and the delayed phase (phase 1b) occurs between the minutes 12 and 30. There is no information whether this bimodal distribution of ischemia-induced arrhythmias during the first 30 min- utes of occlusion also occurs in human, but it is considered likely to be with a retarded time course. It has been proposed that during phase 1a, two different mechanisms are involved in development of arrhythmias. A reentrant excitation causes VF and VT while a non-reentrant mechanism causes premature ventricular depolarizations which subsequently lead to generation of reentry 13. Different factors influence the induction of arrhythmias during the acute phase of myocardial ischemia. One such factor is the current flow across the ischemic and normal myocardial tissue (i.e. the ‘injury current’). The membrane potential is different for ischemic myocardium (less negative) compared with the normal cells. This intercellular electrical imbalance causes current to flow between the depolarized and polarized muscle fibers and induce abnormal activity 13. Another important factor which facilitates VF during acute regional ischemia is the cardiac subendocardial Purkinje fibers 15. During the early phase of acute myocardial ischemia, the electrophysiological properties of the cardiac Purkinje fibers are changed 13. In patients with MI and rapid polymorphic ventricular tachycardia, premature depolarizations and arrhythmias could be suppressed by ablation of Purkinje regions 16. It is suggested that early or delayed afterdepolarizations, sub threshold depolarizations caused by injury currents and the stretch caused by loss of contractility and systolic bulging of the ischemic myocardium could initiate reentry in the Purkinje network 13. During acute myocardial ischemia, the mechanical stretch due to left ventricular malfunction reduces the maximal diastolic potential of the Purkinje fibers and therefore, abnormal activity is induced or accelerated. Stretch can additionally trigger early or delayed afterdepolarizations. The ischemia and injury in the anterior wall seems to play a more prominent role than in the inferior wall in producing stretch and initiation of arrhythmias. Ischemia in the anterior wall causes a greater excursion than ischemia in the inferior wall and thus produces more stretch in the fibers neighboring the ischemic border 13. Heart rate is another important parameter for arrhythmia induction during the acute phase of MI. Changes in heart rate precede the onset of arrhythmia and patients with increased heart rate tend to have higher risk to develop VF during myocardial ischemia. Sequentially, increased heart rate gives rise to severity of ischemic damage and the size of ischemic area 13. Lastly, reperfusion of blood into the ischemic area can trigger the so called reperfusion arrhythmias. The likelihood for reperfusion arrhythmias increases from 5 to 30 minutes after the occlusion in animal models and decreases after 30 minutes. This is due to the fact that arrhythmias must occur in viable cells. During a sudden reperfusion, a very rapid restoration of action potentials occurs in the ischemic myocardium. Electrolytes and metabolites wash out of the ischemic area and change electrophysiological properties of the normal cells close to the ischemic area. This remarkable 37 Chapter 3 Complex inheritance for susceptibility to sudden cardiac death 38 Chapter 3 inhomogeneity in the ischemic myocardium and the border increases the likelihood of reentry and subsequent fibrillation 13. Genetic susceptibility to sudden cardiac death A strong Mendelian hereditary component determines risk of SCD in young individuals 17,18. The genetic underpinnings of the Mendelian disorders associated with increased risk of SCD have been brought into focus during the last two decades leading to an enormous impact on patient care. This Mendelian form of SCD can be caused by underlying electrical (primary electrical disorders) or structural (cardiomyopathies) disturbances (Figure 2). The primary electrical disorders (including long QT syndrome, Brugada syndrome and sick sinus syndrome) are often associated with characteristic abnormal features on the electrocardiogram (ECG). Arrhythmias in these disorders are caused by abnormal intrinsic cardiac electrophysiological properties mainly due to mutations in genes encoding ion channel subunits 19. The most common of these disorders is probably the Long QT Syndrome associated with prolonged cardiomyocyte repolarization. Mutations in a total of 13 genes have so far been linked to this disorder. The genetic underpinnings of the Brugada syndrome on the other hand remain largely unknown. Mutations in the SCN5A gene account for about 20% of probands and while other genes have been implicated in the disorder, between them they account for less than 5% of cases 20. Structural alteration of the myocardium forms the substrate for arrhythmia in the cardiomyopathies, the most common of which is hypertrophic cardiomyopathy, in most cases caused by mutations in MYH7 gene, encoding the β-myosin heavy chain, and in MYBPC3 gene, encoding cardiac myosin-binding protein C (cMyBP‑C) 21. Another rare cardiomyopathy associated with SCD in the young and in athletes is arrhythmogenic right ventricular cardiomyopathy (ARVC). The pathological hallmark of ARVC consists of progressive loss of cardiac myocytes that are replaced by fibrofatty tissue, leading to electric instability. Five of the 8 causative genes thus far associated with the disorder encode major components of the cardiac desmosomes 19. Epidemiological studies have demonstrated that heritable factors also determine variability in susceptibility to SCD in the old age groups (age > 35-40) 22-24 where CAD is the most common underlying pathology. In a population-based case-control study by Friedlander et al. 22, a family history of MI or SCD was associated with more than 50% increased risk of SCD (relative risk [RR] = 1.57). This risk estimation was independent of all common risk factors. A few years later, the same investigators re-analyzed their case-control data. This time, they differentiated between family history of MI and family history of SCD and demonstrated that a positive family history of early-onset SCD (< 65 years of age) independent of parental history of MI contributed to a greater risk of SCD (RR = 2.7) 25. Similarly, in the Paris Prospective Study, selectively performed in men, among whom 118 cases of sudden death occurred, SCD of one parent was found to be an independent risk factor for sudden death (RR = 1.8). There was a remarkable increase in risk if both parents had a history of SCD (RR = 9.4) 23. Although these initial studies highlighted a heritable component in the determination of risk of SCD in the community, they did not differentiate between the different cardiac pathologies in which SCD occurred. Our group has investigated familial aggregation of SCD in the setting of acute myocardial ischemia in the Arrhythmia Genetics in the Netherlands Study (AGNES), conducted specifically in patients with a first acute ST- segment elevation MI 24. This case-control study demonstrated that patients with familial SCD were at higher risk of developing VF during a first acute MI (odds ratio [OR] = 2.72) 24. Within the same year, a study from Finland uncovered similar findings. Kaikkonen et al. 26 showed that patients with SCD in the setting of a first acute MI were more likely to have a family history of SCD compared with survivors of acute MI (OR = 1.6) or compared with healthy controls (OR = 2.2). The presence of SCD in two or more first degree relatives increased risk of SCD remarkably compared with survivors of MI (OR = 3.3) or compared with healthy controls (OR = 11.3). These studies clearly demonstrate familial aggregation of SCD pointing to a heritable component in the determination of risk. Importantly, since these studies control for the presence of acute MI, they show that genetic susceptibility specific for the arrhythmic event exists and is unrelated to, for example, the genetic susceptibility to the hemodynamic consequences of the MI itself. However, despite this evidence, advances in uncovering genetic factors underlying susceptibility to arrhythmias in the setting of complex cardiac pathologies, affecting a much greater proportion of the population, has been very limited 27-29. To date only a few genetic variants modulating risk in this setting have been uncovered. We here review the current insight on genetic determinants of SCD in the community and mainly describe genome-wide association approaches undertaken thus far in uncovering the genetic determinants of SCD risk. Genome-wide association studies (GWAS) GWAS test millions of common variants (variants present in more than 5% of the population) across the genome to identify those variants that are significantly associated with complex diseases 30. Conducting genetic studies for SCD in large scale is extremely challenging. Most cases of cardiac arrest occur early after the onset of symptoms. The majority of such 39 Chapter 3 Complex inheritance for susceptibility to sudden cardiac death 40 Chapter 3 early onset SCD cases that do not undergo resuscitation or are not witnessed are consequently not included in the analysis 11. DNA of individuals with the SCD phenotype is difficult to obtain due to the natural course of the event. Moreover, ethical issues related to collection of DNA from SCD victims limit inclusion of patients. In addition, the lack of homogeneity of the underlying cardiac pathology (and consequently the mechanism of the attendant arrhythmia) complicates the interpretation of findings across different genetic studies. However, large samples of homogeneous SCD phenotype are challenging to collect for various reasons. The SD cases in the community must have a cardiac origin to be defined as SCD. However, that is not always the case and other underlying pathologies (e.g. stroke or aneurysm) may be the cause. In addition, SCD may not always be mediated by VF. Even a documented VF may not always be in the setting of a first MI. Previous MI or structural disturbances of the heart (cardiomyopathies) may also be associated with VF and ultimately SCD. Detailed clinical information regarding the event (including previous medical history, drug use, etc.) or autopsies are the only methods to obtain sufficient information concerning the underlying cardiac pathology in SCD. However, obtaining information about previous medical and medication history of SCD victims, which would provide information about the underlying cardiac substrate, is largely restricted and autopsy is conducted only sporadically 31. Up to now, three genome wide association studies on SCD and one on VF have investigated the role of common genetic variants in occurrence of these traits 32-35. Only two studies were able to reach the genome-wide significant threshold of P < 5 × 10−8 and replicate the findings 33,35. Table 1 summarizes genetic variants that have been found in the studies for SCD/VF. The first GWAS for VF in MI was conducted in the AGNES case-control set 35 aiming to identify single nucleotide polymorphisms (SNPs) associated with risk of VF in the setting of acute MI. The AGNES study comprises Dutch individuals with a first ST-segment elevation acute MI where survivors of VF (n = 457) are compared with patients without VF (n = 515). The high specification of the phenotype in the AGNES study increases the chance to detect genetic variants that are associated with VF rather than other arrhythmias through which SCD may occur. The control set is collected Table 1 | Genetic variants that have been found associated with SCD SNP Location Nearest gene Risk allele Effect size P-value rs2824292 Intergenic CXADR G 1.78 3.3 × 10−10 VF rs4665058 Intronic BAZ2B A 1.92 1.8 × 10−10 SD/SCD SCD phenotype SNP, single nucleotide polymorphism; SCD, sudden cardiac death; VF, ventricular fibrillation; SD, sudden death from the same patient population as the VF patients. This similarly-exposed control set increases the statistical power for detection of variants and reduces the chance of confounding. The AGNES study identified (chapter 4 of this thesis) a genetic variant at chromosome 21q21 (lead SNP rs2824292) in a non-coding region in the vicinity of the CXADR gene, which encodes the coxsackie and adenovirus receptor. The association was replicated in a similar population consisting of 146 out of hospital cardiac arrest cases (in the setting of acute MI) and 391 controls (i.e. MI without VF). CXADR encodes the coxsackievirus and adenovirus receptor (CAR) and is expressed in the heart (http://www.genecards.org). CAR is long known to play a role in mediating viral myocarditis and its sequelum dilated cardiomyopathy 36,37. Two studies have uncovered a physiologic role for CAR in localization of connexin 45 at the intercalated disks of cardiomyocytes in the atrioventricular node, and a role in conduction of the cardiac impulse within this cardiac compartment 38,39. Whether CAR plays a role in ventricular conduction is yet unknown as is the mechanism whereby it could impact on risk of VF during acute MI. The second GWAS, conducted by Arking et al 33 consisted of a large meta-analysis of multiple genome-wide association studies for SD/SCD carried out in individuals of European ancestry. In the first stage, this study compared 1,283 SD/SCD cases and > 20,000 controls drawn from a combination of five case-control and population-based studies conducted in Europe and the U.S. Various underlying pathologies causing SD or SCD were included in this meta-analysis. The controls comprised both CAD controls and population-based controls. These investigators 33 identified a genetic variant at chromosome 2q24.2 (lead SNP rs4665058) in an intron in the BAZ2B gene, which encodes bromodomain adjacent zinc finger domain 2B and is expressed in the heart. The BAZ2B gene was not previously known to play a role in cardiac arrhythmia or SCD. BAZ2B which was first identified and described in 2000 by Jones et al. belongs to the ZK783.4 subfamily in the BAZ gene family (bromodomain adjacent zinc finger). The function of the ZK783.4 subfamily has yet to be elucidated. The finding was described to be consistent in studies comparing SD/SCD cases with CAD controls (FinGesture and Oregon-SUDS) 33 ensuring that the risk associated with rs4665058 may be specific to the SCD phenotype rather than CAD. This association was replicated in 3119 SD/ SCD cases and 11,146 controls from 11 European ancestry populations which also included the AGNES case-control set. When the AGNES case-control set was considered separately however, the BAZ2B locus did not demonstrate an effect on risk of VF. Similarly, the CXADR signal detected in the AGNES GWAS was not detected in a small case-control set (90 patients with acute MI and VF and 167 MI non-VF controls) from Germany 40. These differences may be due to differences in phenotype definition and study design, statistical power or pure chance. 41 Chapter 3 Complex inheritance for susceptibility to sudden cardiac death 42 Chapter 3 A pilot GWAS with a very small sample size 32 investigated genetic determinants of SCD by comparing genetic differences of 89 cases with 520 healthy controls. The cases were defined as patients suffering from sudden cardiac arrest due to documented sustained VT or VF requiring cardioversion or defibrillator in presence (n = 36) or absence (n = 53) of acute myocardial ischemia 32. This study identified 14 non-replicated variants associated with SCD at the genome wide significant level (see table 2 from Aouizerat et al. 32). The most significant SNP (rs12429889; P-value = 5.28 × 10−20) was located at chromosome 13q22.1 in the vicinity of KLF12 gene, which encodes Kruppellike factor 12. KLF12 is a transcriptional silencer of adaptor-related protein complex 2, alpha 1 subunit (AP2A1) which has been implicated in vesicle trafficking (OMIM: 601026; 607531). In the study by Aouizerat et al; the number of cases was very small and multiple SCD phenotypes were included. In addition, the study lacked replication of the results in other independent populations. In causal inference studies, it is important to keep in mind that the sentinel genetic variant itself (i.e. the SNP displaying the strongest genetic association) may not necessarily be the causal variant. SNPs display linkage disequilibrium (LD, the non-random association between alleles at two or more loci along a chromosomal segment) and are inherited as haplotype blocks. Thus any variant within such a haplotype block (displaying high LD with the sentinel SNP) could in principle be the causal variant 30. Common genetic variants are expected to modify the risk of SCD through different genetic mechanisms. However, the mechanism through which the identified variants are associated with SCD is in most cases not immediately clear. Oftentimes the sentinel variant does not commonly occur in strong LD with any missense or splice variants in the coding regions of genes. Variants identified in GWAS are often located in the nonprotein coding regions of the genome. This suggests that the genetic variation affects a regulatory element which modulates disease susceptibility through effects on the level of expression of a gene; the regulated gene may be neighboring the association signal but may also be further away in the genome. In this regard, studies investigating the genetic regulation of gene expression, commonly referred to as expression quantitative trait locus (eQTL) analysis, in cardiac tissue as well as genome-wide identification of regulatory regions by ChIP-Seq (chromatin immunoprecipitation sequencing) 41 are likely to aid causal inference. In addition to the future possibilities for risk stratification, an important motivation of carrying out genetic studies on SCD is to uncover novel molecular players that could illuminate previously unsuspected pathways involved in the determination of risk. Following GWAS, follow-on causal inference and functional studies in animal models resembling the disorder in humans are therefore necessary and important to reap the full benefit of GWAS efforts. This is a crucial step in order to translate the Complex inheritance for susceptibility to sudden cardiac death 43 emerging scientific knowledge to patient management and development of new or better targeted therapy for prevention of SCD. An alternative approach to GWAS of SCD is to identify genetic variants associated with phenotypes that are considered as risk factors for SCD 31. Such phenotypes are often referred to as “intermediate phenotypes”. It is thought that genetic variants that are associated with an intermediate phenotype should have a similar relation to the disease of interest if the intermediate phenotype is a causal factor for that disease 42. A proper intermediate phenotype should be quantifiable and should display heritability in order to be useful in gene discovery. Heart rate and ECG indices of conduction and repolarization are considered important quantifiable intermediate phenotypes for risk of developing cardiac arrhythmias (Table 2; reviewed in reference 31). For instance, we have previously shown that ECG indices measured during the acute phase of a first MI were associated with risk of ensuing VF 43. Furthermore, a number of studies have demonstrated that heart rate, PR interval, QRS duration and Table 2 | Established SNPs affecting ECG indices of heart rate, conduction and repolarization SNP Coded/Non Coded Allele GWAS Beta (ms per copy of coded Allele) Minor Allele (Frequency) Genea RR SNPs rs11154022 A/G 5.8 A (0.33) 8 kb from GJA1 rs12666989 C/G −7.0 C (0.20) UFSP1 rs17287293 G/A 8.6 G (0.14) SOX5-BCAT1 rs174547 C/T −6.2 C (0.31) FADS1 rs223116 A/G −7.4 A (0.24) THTPA-NGDN-ZFHX2-MYH7 rs2745967 G/A 5.4 G (0.38) CD34-PLXNA2 rs281868 G/A −6.3 A (0.49) SLC35F1 rs314370 C/T −7.6 C (0.20) SLC12A9 rs452036 A/G −7.8 A (0.39) MYH6 rs885389 A/G −0.17 A (0.37) GPR133 rs9398652 A/C −12.6 A (0.12) GJA1-HSF2 rs11047543 A/G −2.09 A (0.14) SOX5 rs11708996 C/G 3.04 C (0.16) SCN5A PR SNPs a According to the definition of the original publication where the association was first identified. Chapter 3 Intermediate phenotypes in SCD 44 Chapter 3 Table 2 | Established SNPs affecting ECG indices of heart rate, conduction and repolarization (continued) Coded/Non Coded Allele GWAS Beta (ms per copy of coded Allele) Minor Allele (Frequency) Genea rs11897119 C/T 1.36 C (0.38) MEIS1 rs1896312 C/T 1.95 C (0.29) TBX5-TBX3 rs251253 C/T −1.49 C (0.41) NKX2-5 rs3807989 A/G 2.29 A (0.42) CAV1-CAV2 rs3825214 G/A 7.35 G (0.20) TBX5 rs4944092 G/A −1.19 G (0.33) WNT11 rs6795970 A/G 14.81 A (0.39) SCN10A rs7660702 T/C 8.46 C (0.30) ARHGAP24 A/G 1.78 G (0.11) ATP1B1 rs11970286 T/C 1.53 T (0.47) PLN rs12029454 A/G 0.17 A (0.14) NOS1AP SNP QTc SNPs rs10919071 rs12053903 C/T −0.07 C (0.33) SCN5A rs12143842 T/C 0.18 T (0.24) NOS1AP rs12210810 C/G 0.06 C (0.04) PLN rs12296050 T/C 1.62 T (0.18) KCNQ1 rs16857031 G/C 0.15 G (0.14) NOS1AP rs17779747 T/G −1.10 T (0.34) KCNJ2 rs1805128 A/G 0.05 T (0.05) KCNE1 rs2074238 T/C −0.45 T (0.05) KCNQ1 rs2074518 T/C −0.06 T (0.49) LIG3 rs2968863 T/C −1.37 T (0.26) KCNH2 rs37062 G/A −0.10 G (0.23) CNOT1 rs4657178 T/C 0.3 T (0.25) NOS1AP rs4725982 T/C 0.09 T (0.19) KCNH2 rs8049607 T/C 0.07 C (0.49) LITAF rs846111 C/C 0.10 C (0.29) RNF207 rs10850409 A/G −0.49 A (0.25) TBX3 rs10865879 T/C 0.77 C (0.25) SCN5A-EXOG rs11153730 C/T 0.59 T (0.49) C6orf204-SLC35F1PLN-BRD7P3 rs11708996 C/G 0.79 C (0.16) SCN5A rs11710077 T/A −0.84 T (0.18) SCN5A QRS SNPs a According to the definition of the original publication where the association was first identified. Complex inheritance for susceptibility to sudden cardiac death 45 Coded/Non Coded Allele GWAS Beta (ms per copy of coded Allele) Minor Allele (Frequency) Genea rs11848785 G/A −0.5 G (0.27) SIPA1L1 rs13165478 A/G −0.55 A (0.37) HAND1-SAP30L rs1321311 A/C 7.14 A (0.24) CDKN1A rs1362212 A/G 0.69 A (0.16) TBX20 rs17020136 C/T 0.51 C (0.21) HEATR5B-STRN rs1733724 A/G 0.49 A (0.27) DKK1 rs17391905 G/T −1.35 G (0.02) C1orf185-RNF11CDKN2C-FAF1 rs17608766 C/T 0.53 C (0.13) GOSR2 SNP rs1886512 A/T −0.4 A (0.37) KLF12 rs2051211 G/A −0.44 G (0.26) EXOG rs2242285 A/G 0.37 A (0.43) LRIG1-SLC25A26 rs4074536 C/T −0.42 C (0.32) CASQ2 rs4687718 A/G −0.63 A (0.12) TKT-PRKCD-CACNA1D rs6795970 A/G 4.45 A (0.39) SCN10A rs7342028 T/G 0.48 T (0.25) VTI1A rs7562790 G/T 0.39 G (0.43) CRIM1 rs7784776 G/A 0.39 G (0.41) IGFBP3 rs883079 C/T 0.49 C (0.26) TBX5 rs9436640 G/T −0.59 G (0.48) NFIA rs9851724 C/T −0.66 C (0.35) SCN10A rs991014 T/C 0.42 T (0.43) SETBP1 rs9912468 G/C 0.39 G (0.40) PRKCA a According to the definition of the original publication where the association was first identified. QTc interval are strongly heritable traits 44-46. This implies that a strong genetic component determines the variation in these traits. Following these findings, large-scale GWAS in large samples of the general population have identified numerous SNPs modulating heart rate, and ECG indices of conduction (PR interval, QRS duration) and repolarization (QTc interval) 47-53. SNPs identified for each of these traits have recently been summarized by Kolder et al. 31. As is typical for genetic variants with high population frequency, these variants explain a very small portion of the population variance in the respective parameter. This translates to an effect of less than one or two milliseconds in the respective ECG parameter. Even when these common variants with marginal effects on ECG traits are considered Chapter 3 Table 2 | Established SNPs affecting ECG indices of heart rate, conduction and repolarization (continued) 46 Chapter 3 in aggregate, they still explain only a very small percentage of the variation in these traits. For instance, in a meta-analysis for identification of QTc-associating SNPs by Pfeufer et al. 51, SNPs at 10 different loci in aggregate explained only around 3% of the variance in this trait. So far, studies have largely shown that SNPs that were previously implicated in modulating ECG traits, do not exert an influence in determination of risk of SCD, both when considered individually or in aggregate 33,47. Arking et al. 33 tested 49 SNPs which are known to exert small effects on ECG traits for effects on modulation of SCD risk in the general population. Only one SNP (rs4687718) showed association with the SD/ SCD phenotype in a large population consisting of 1,283 SD/SCD cases and more than 20,000 controls of European ancestry. Noseworthy et al. 54 tested 15 common variants that were previously found to be associated with QTc interval in GWAS. While almost all of these variants showed association with QTc interval individually and in aggregate, these SNPs did not display modulatory effects on SCD risk in a population consisting of 116 SCD cases and 6808 controls. These variants in aggregate showed a nonlinear association with SCD. However, Lahtinen et al. 55 from the same group could not replicate this finding in a further larger meta-analysis. We recently tested common variants that were previously found to be associated with RR interval, PR interval, QRS duration, and QTc interval for effects on VF in the setting of a first acute MI in the AGNES case-control set 56. Our findings were in line with those of previous investigators as the SNPs did not display any marked effect on risk of VF. In those few studies where an individual effect of a SNP on risk of SCD was shown, the effect was at times counter-intuitive. For instance the QRS-shortening A-allele at rs4687718 33,50 is a SNP that has been found in GWAS for QRS duration and each A allele at rs4687718 was found to be associated with an increased risk of SCD (OR = 1.27) 33. In another study by Chambers et al. 47, the PR interval-prolonging allele at rs6795970 was associated with decreased risk of VF during acute MI. It is clear that more work is required to both validate these initial findings and eventually understand the underlying mechanism. Obviously, genetic variants identified thus far as modulators of ECG traits cannot be used for assessing genetic susceptibility to SCD. The findings so far highlights the need for further studies with large sample sizes aiming to uncover additional genetic variants, such as rare variants associated with larger effects, which would lead to a more-complete representation of the allelic architecture of these ECG differences in the general population. Complex inheritance for susceptibility to sudden cardiac death 47 Understanding the genetic structure of complex traits as is cardiac arrhythmia is a major challenge 57. The studies that have investigated the role of common genetic variation in SCD risk have so far identified only few signals. Difficulty in collection of SCD cases and the proper characterization of the underlying cardiac pathology for strict definition of the phenotype represent major obstacles. Collaborations in large scale have been initiated in order to increase the sample size and consequently the statistical power to detect more variants; the current efforts to gain statistical power are at the expense of phenotypic heterogeneity. Careful downstream epidemiological studies as well as functional studies will be required to understand the exact cardiac pathology where the variants exert their effect. The research in this field gets even more challenging as the search for genetic predisposition to complex phenotypes is shifting to encompass the role of rare variants in risk of SCD which consequently necessitates even larger sample sizes to ensure statistical power. Summary SCD accounts for up to half of all cardiovascular deaths. In the young it occurs primarily in the setting of the primary electrical disorders and the cardiomyopathies, disorders displaying Mendelian inheritance. Significant progress has been made in the last 15 years in unraveling genes underlying these disorders. However, most SCD cases occur due to VF in the setting of myocardial infarction/ischemia in the older segment of the population. During ischemia, multiple factors that can trigger arrhythmia include injury current, changes in electrophysiological properties of the cardiac Purkinje fibers, mechanical stretch due to left ventricular malfunction, changes in the heart rate and reperfusion of blood into the ischemic area. Although unequivocal evidence exists for a genetic component in the determination of risk for VF in the setting of ischemia/infarction, the underlying genetic factors remain largely unidentified. To date only a few genetic variants modulating VF risk in this setting have been uncovered. So far, GWAS have identified two loci close to the CXADR and within BAZ2B genes, respectively, as susceptibility loci for VF and SCD. The molecular function through which these loci are associated with SCD has yet to be elucidated. Intermediate phenotypes such as ECG traits have been used as a surrogate in order to identify genetic variants modulating risk of SCD. However, studies conducted thus far demonstrate that, such variants do not have a marked effect on susceptibility. Fu- Chapter 3 Future perspective for the genetics of SCD 48 Chapter 3 ture large scale collaborative studies on large patient sets might provide the statistical power required to detect their effect. Acknowledgement The authors are supported by research grants from the Netherlands Heart Foundation (grants 2001D019, 2003T302 and 2007B202), the Leducq Foundation (grant 05-CVD) and the Netherlands Heart Institute. Dr. C.R. Bezzina is an Established Investigator of the Netherlands Heart Foundation (grant 2005T024). We thank Jonas S. de Jong for providing Figure 1. Complex inheritance for susceptibility to sudden cardiac death 49 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. van der Werf, C., van Langen, I. M. & Wilde, A. A. M. Sudden Death in the Young What Do We Know About It and How to Prevent? Circulation-Arrhythmia and Electrophysiology 3, 96-104, doi:10.1161/circep.109.877142 (2010). deVreedeSwagemakers, J. J. M. et al. Out-of-hospital cardiac arrest in the 1990s: A population-based study in the Maastricht area on incidence, characteristics and survival. Journal of the American College of Cardiology 30, 1500-1505, doi:10.1016/s0735-1097(97)00355-0 (1997). Liberthson, R. R. Current concepts - Sudden death from cardiac causes in children and young adults. New England Journal of Medicine 334, 1039-1044, doi:10.1056/ nejm199604183341607 (1996). van der Werf, C. et al. Diagnostic yield in sudden unexplained death and aborted cardiac arrest in the young: The experience of a tertiary referral center in The Netherlands. Heart Rhythm 7, 1383-1389, doi:10.1016/j.hrthm.2010.05.036 (2010). Fishman, G. I. et al. Sudden Cardiac Death Prediction and Prevention Report From a National Heart, Lung, and Blood Institute and Heart Rhythm Society Workshop. Circulation 122, 2335-2348, doi:10.1161/circulationaha.110.976092 (2010). John, R. M. et al. Ventricular arrhythmias and sudden cardiac death. Lancet 380, 1520-1529 (2012). Chugh, S. S. Early identification of risk factors for sudden cardiac death. Nature Reviews Cardiology 7, 318-326, doi:10.1038/nrcardio.2010.52 (2010). Chugh, S. S. et al. Current burden of sudden cardiac death: Multiple source surveillance versus retrospective death certificate-based review in a large US community. Journal of the American College of Cardiology 44, 1268-1275, doi:10.1016/j.jacc.2004.06.029 (2004). Myerburg, R. J. & Castellanos, A. in Braunwald’s Heart Disease: ATextbook of Cardiovascular Medicine (eds P. Libby, R. O. Bonow, D. L. Mann, & D. P. Zipes) (Elsevier, 2007). Huikuri, H. V., Castellanos, A. & Myerburg, R. J. Medical progress: Sudden death due to cardiac arrhythmias. New England Journal of Medicine 345, 1473-1482, doi:10.1056/ NEJMra000650 (2001). Chugh, S. S. et al. Epidemiology of Sudden Cardiac Death: Clinical and Research Implications. Progress in Cardiovascular Diseases 51, 213-228, doi:10.1016/j.pcad.2008.06.003 (2008). Zipes, D. P. & Wellens, H. J. J. Sudden cardiac death. Circulation 98, 2334-2351 (1998). Janse, M. J. & Wit, A. L. Electrophysiological mechanisms of ventricular arrhythmias resulting from myocardial ischemia and infarction. Physiological Reviews 69, 1049-1169 (1989). Moss, A. J. et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. New England Journal of Medicine 346, 877-883, doi:10.1056/NEJMoa013474 (2002). Janse, M. J. Vulnerability to ventricular fibrillation. Chaos 8, 149-156, doi:10.1063/1.166295 (1998). Szumowski, L. et al. Mapping and ablation of polymorphic ventricular tachycardia after myocardial infarction. Journal of the American College of Cardiology 44, 1700-1706, doi: 10.1016/j.jacc.2004.08.034 (2004). Tan, H. L., Hofman, N., van Langen, I. M., van der Wal, A. C. & Wilde, A. A. Sudden unexplained death: heritability and diagnostic yield of cardiological and genetic examination Chapter 3 References 50 Chapter 3 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. in surviving relatives. Circulation 112, 207-213, doi:10.1161/circulationaha.104.522581 (2005). Basso, C. et al. Sudden cardiac death with normal heart: molecular autopsy. Cardiovascular Pathology 19, 321-325, doi:10.1016/j.carpath.2010.02.003 (2010). Wilde, A. A. & Bezzina, C. R. Genetics of cardiac arrhythmias. Heart (British Cardiac Society) 91, 1352-1358, doi:10.1136/hrt.2004.046334 (2005). Crotti, L. et al. Spectrum and Prevalence of Mutations Involving BrS1-Through BrS12-Susceptibility Genes in a Cohort of Unrelated Patients Referred for Brugada Syndrome Genetic Testing Implications for Genetic Testing. Journal of the American College of Cardiology 60, 1410-1418, doi:10.1016/j.jacc.2012.04.037 (2012). Watkins, H., Ashrafian, H. & Redwood, C. MECHANISMS OF DISEASE Inherited Cardiomyopathies. New England Journal of Medicine 364, 1643-1656 (2011). Friedlander, Y. et al. Family history as a risk factor for primary cardiac arrest. Circulation 97, 155-160 (1998). Jouven, X., Desnos, M., Guerot, C. & Ducimetiere, P. Predicting sudden death in the population - The Paris Prospective Study I. Circulation 99, 1978-1983 (1999). Dekker, L. R. et al. Familial sudden death is an important risk factor for primary ventricular fibrillation: a case-control study in acute myocardial infarction patients. Circulation 114, 1140-1145, doi:10.1161/circulationaha.105.606145 (2006). Friedlander, Y. et al. Sudden death and myocardial infarction in first degree relatives as predictors of primary cardiac arrest. Atherosclerosis 162, 211-216, doi:10.1016/s00219150(01)00701-8 (2002). Kaikkonen, K. S., Kortelainen, M.-L., Linna, E. & Huikuri, H. V. Family history and the risk of sudden cardiac death as a manifestation of an acute coronary event. Circulation 114, 1462-1467, doi:10.1161/circulationaha.106.624593 (2006). Arking, D. E., Chugh, S. S., Chakravarti, A. & Spooner, P. M. Genomics in sudden cardiac death. Circulation Research 94, 712-723, doi:10.1161/01.res.0000123861.16082.95 (2004). Myerburg, R. J. & Castellanos, A. Emerging paradigms of the epidemiology and demographics of sudden cardiac arrest. Heart Rhythm 3, 235-239, doi:10.1016/j.hrthm.2005.09.023 (2006). Noseworthy, P. A. & Newton-Cheh, C. Genetic Determinants of Sudden Cardiac Death. Circulation 118, 1854-1863, doi:10.1161/circulationaha.108.783654 (2008). Visscher, P. M., Brown, M. A., McCarthy, M. I. & Yang, J. Five Years of GWAS Discovery. American Journal of Human Genetics 90, 7-24, doi:10.1016/j.ajhg.2011.11.029 (2012). Kolder, I. C. R. M., Tanck, M. W. T. & Bezzina, C. R. Common genetic variation modulating cardiac ECG parameters and susceptibility to sudden cardiac death. Journal of Molecular and Cellular Cardiology 52, 620-629, doi:10.1016/j.yjmcc.2011.12.014 (2012). Aouizerat, B. E. et al. GWAS for discovery and replication of genetic loci associated with sudden cardiac arrest in patients with coronary artery disease. Bmc Cardiovascular Disorders 11, doi:10.1186/1471-2261-11-29 (2011). Arking, D. E. et al. Identification of a Sudden Cardiac Death Susceptibility Locus at 2q24.2 through Genome-Wide Association in European Ancestry Individuals. Plos Genetics 7, doi: 10.1371/journal.pgen.1002158 (2011). Arking, D. E. et al. Genome-Wide Association Study Identifies GPC5 as a Novel Genetic Locus Protective against Sudden Cardiac Arrest. Plos One 5, doi:10.1371/journal.pone.0009879 (2010). 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. Bezzina, C. R. et al. Genome-Wide Association Study Identifies a Region at Chr 21q21 as a Susceptibility Locus for Ventricular Fibrillation in Acute Myocardial Infarction. Circulation 122, 1 (2010). Bowles, N. E., Richardson, P. J., Olsen, E. G. J. & Archard, L. C. Detection of coxsackie-bvirus-specific RNA sequences in myocardial biopsy samples from patients with myocarditis and dilated cardiomyopathy. Lancet 1, 1120-1124 (1986). Pauschinger, M. et al. Detection of adenoviral genome in the myocardium of adult patients with idiopathic left ventricular dysfunction. Circulation 99, 1348-1354 (1999). Lisewski, U. et al. The tight junction protein CAR regulates cardiac conduction and cellcell communication. Journal of Experimental Medicine 205, 2369-2379, doi:10.1084/ jem.20080897 (2008). Lim, B.-K. et al. Coxsackievirus and adenovirus receptor (CAR) mediates atrioventricularnode function and connexin 45 localization in the murine heart. Journal of Clinical Investigation 118, 2758-2770, doi:10.1172/jci34777 (2008). Bugert, P. et al. No evidence for an association between the rs2824292 variant at chromosome 21q21 and ventricular fibrillation during acute myocardial infarction in a German population. Clinical Chemistry and Laboratory Medicine 49, 1237-1239, doi:10.1515/ cclm.2011.190 (2011). Blow, M. J. et al. ChIP-Seq identification of weakly conserved heart enhancers. Nature Genetics 42, 806-U107, doi:10.1038/ng.650 (2010). Verduijn, M., Siegerink, B., Jager, K. J., Zoccali, C. & Dekker, F. W. Mendelian randomization: use of genetics to enable causal inference in observational studies. Nephrology Dialysis Transplantation 25, 1394-1398, doi:10.1093/ndt/gfq098 (2010). Lemmert, M. E. et al. Electrocardiographic factors playing a role in ischemic ventricular fibrillation in ST elevation myocardial infarction are related to the culprit artery. Heart Rhythm 5, 71-78, doi:10.1016/j.hrthm.2007.09.011 (2008). Havlik, R. J., Garrison, R. J., Fabsitz, R. & Feinleib, M. Variability of heart-rate, P-R, QRS and Q-T durations in twins. Journal of Electrocardiology 13, 45-48, doi:10.1016/s00220736(80)80008-2 (1980). Hanson, B. et al. Genetic-factors in the electrocardiogram and heart-rate of twins reared apart and together. American Journal of Cardiology 63, 606-609, doi:10.1016/00029149(89)90907-7 (1989). Russell, M. W., Law, I., Sholinsky, P. & Fabsitz, R. R. Heritability of ECG measurements in adult male twins. Journal of electrocardiology 30 Suppl, 64-68, doi:10.1016/s00220736(98)80034-4 (1998). Chambers, J. C. et al. Genetic variation in SCN10A influences cardiac conduction. Nature Genetics 42, 149-U180, doi:10.1038/ng.516 (2010). Pfeufer, A. et al. Genome-wide association study of PR interval. Nature Genetics 42, 153U189, doi:10.1038/ng.517 (2010). Holm, H. et al. Several common variants modulate heart rate, PR interval and QRS duration. Nature Genetics 42, 117-U140, doi:10.1038/ng.511 (2010). Sotoodehnia, N. et al. Common variants in 22 loci are associated with QRS duration and cardiac ventricular conduction. Nature Genetics 42, 1068-U1062, doi:10.1038/ng.716 (2010). Pfeufer, A. et al. Common variants at ten loci modulate the QT interval duration in the QTSCD Study. Nature Genetics 41, 407-414, doi:10.1038/ng.362 (2009). 51 Chapter 3 Complex inheritance for susceptibility to sudden cardiac death 52 Chapter 3 52. 53. 54. 55. 56. 57. Arking, D. E. et al. A common genetic variant in the NOS1 regulator NOS1AP modulates cardiac repolarization. Nature Genetics 38, 644-651, doi:10.1038/ng1790 (2006). Newton-Cheh, C. et al. Common variants at ten loci influence QT interval duration in the QTGEN Study. Nature Genetics 41, 399-406, doi:10.1038/ng.364 (2009). Noseworthy, P. A. et al. Common Genetic Variants, QT Interval, and Sudden Cardiac Death in a Finnish Population-Based Study. Circulation-Cardiovascular Genetics 4, 305-U183, doi: 10.1161/circgenetics.110.959049 (2011). Lahtinen, A. M. et al. Common Genetic Variants Associated with Sudden Cardiac Death: The FinSCDgen Study. Plos One 7, doi:10.1371/journal.pone.0041675 (2012). Pazoki, R. et al. SNPs Identified as Modulators of ECG Traits in the General Population Do Not Markedly Affect ECG Traits during Acute Myocardial Infarction nor Ventricular Fibrillation Risk in This Condition. Plos One 8, doi:10.1371/journal.pone.0057216 (2013). Orozco, G., Barrett, J. C. & Zeggini, E. Synthetic associations in the context of genome-wide association scan signals. Human Molecular Genetics 19, R137-R144, doi:10.1093/hmg/ ddq368 (2010).