Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Lutembacher's syndrome wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Heart arrhythmia wikipedia , lookup
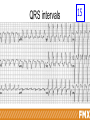
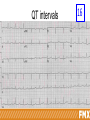
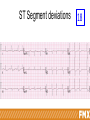
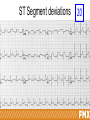
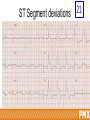
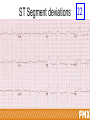
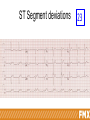
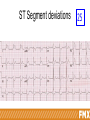
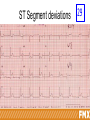
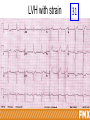
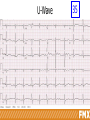
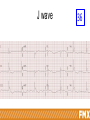
ECG Analysis (Fundamentals) Vukiet Tran, MD, MBA ACTIVITY DISCLAIMER The material presented here is being made available by the American Academy of Family Physicians for educational purposes only. This material is not intended to represent the only, nor necessarily best, methods or procedures appropriate for the medical situations discussed. Rather, it is intended to present an approach, view, statement, or opinion of the faculty, which may be helpful to others who face similar situations. The AAFP disclaims any and all liability for injury or other damages resulting to any individual using this material and for all claims that might arise out of the use of the techniques demonstrated therein by such individuals, whether these claims shall be asserted by a physician or any other person. Every effort has been made to ensure the accuracy of the data presented here. Physicians may care to check specific details such as drug doses and contraindications, etc., in standard sources prior to clinical application. This material might contain recommendations/guidelines developed by other organizations. Please note that although these guidelines might be included, this does not necessarily imply the endorsement by the AAFP. DISCLOSURE It is the policy of the AAFP that all individuals in a position to control content disclose any relationships with commercial interests upon nomination/invitation of participation. Disclosure documents are reviewed for potential conflict of interest (COI), and if identified, conflicts are resolved prior to confirmation of participation. Only those participants who had no conflict of interest or who agreed to an identified resolution process prior to their participation were involved in this CME activity. All individuals in a position to control content for this activity have indicated they have no relevant financial relationships to disclose. The content of my material/presentation in this CME activity will not include discussion of unapproved or investigational uses of products or devices. The content of my material/presentation in this CME activity will include discussion of unapproved or investigational uses of products or devices as indicated: Vukiet Tran, MD, MBA Assistant Professor, Department of Family and Community Medicine, University of Toronto, Ontario, Canada. Dr. Tran practices family medicine and emergency medicine in a group practice in suburban Toronto, Ontario, Canada. His practice encompasses the full spectrum of family medicine, from pediatric patients to the elderly. Dr. Tran has taught for 15 years in an academic emergency medicine center affiliated with the University of Toronto. His specialty topics include emergency medicine, cardiovascular medicine, dermatology, and procedures in the emergency department. Dr. Tran believes in lifelong learning. Learning Objectives 1. Compare and contrast the findings of ECG tests in different patient cases. 2. Relate the implications of ECG readings to potential cardiac disease. 3. Compare the findings of an ECG to a patient’s clinical presentation. 4. Compare the results of multiple ECG findings from the same patient. ECG IS ONLY A TOOL TO SUPPLEMENT YOUR CLINICAL ASSESSMENT INTERPRETATION OF ECG MUST BE DONE SYSTEMATICALLY - ESSENTIAL COMPONENTS NEED TO BE SYNTHESIZED - THE GOAL IS A RAPID AND ACCURATE DIAGNOSIS Simple and tried process 1. 2. 3. 4. 5. 6. 7. Rate Rhythm Axis Intervals ST segments Morphology Special conditions Simple and tried process 1.Rate 2. 3. 4. 5. 6. 7. Rhythm Axis Intervals ST segments Morphology Special conditions Normal ECG paper Pacemaker sites of the heart Pacemaker Normal rate (bpm) Sinoatrial (SA) node 60-100 Atrioventricular node (Junctional) 40-60 Ventricular 20-40 Determining the rate • Method I: 300-150-100-75-60-50-42-38 rule – – – – Choose an R that falls on or close a thick line The first thick line right to it is 300 line The second is the 150 line And so on… OR – Start with a QRS that occurs on a thick line – Locate the next QRS – Divide 300 by the number of thick lines in between the QRSs 1 2 Determining the rate • Method II: count the number of QRS in 6 seconds – That number multiple by 10 – More accurate method if the rhythm is irregular 3 4 Determining the rate • Method III: duration between two R waves – Count in duration (in seconds) between two R waves – divide 60 by this number 5 0.68 sec Rate = 60 ÷ 0.68 = 88 Simple and tried process 1. Rate 2.Rhythm 3. 4. 5. 6. 7. Axis Intervals ST segments Morphology Special conditions Sinus rhythms • Normal Sinus 6 Normal Sinus Rhythm • Regular rhythm 60-100 • Each QRS are preceded by a normal P wave • Each P wave followed by a QRS Complex • P are positives in I, II, AVF • PR interval is normal Sinus rhythms • Sinus Bradycardia 7 Sinus rhythms • Sinus Tachycardia 8 Junctional rhythms • Junctional escape rhythm 9 Junctional rhythm • Rate of 40-60 • QRS are narrow • No P waves Ventricular rhythms • Idioventricular escape rhythm 10 Ventricular rhythm • • • • Rate between 20-40 Regular rate QRS are wide No P waves Accelerated Idioventricular 10A Simple and tried process 1. Rate 2. Rhythm 3.Axis 4. 5. 6. 7. Intervals ST segments Morphology Special conditions Normal QRS Axis Axis determination • Method I – Determine which quadrant your axis is in using Lead I and AVF • Method II – Find the most isoelectric lead (the Axis is perpendicular to this lead) • Method III – The tallest QRS points toward the Axis (Limb Leads) Axis – Method I Lead I +ve Lead AVF +ve Axis Method II 11 Axis Method III 11 Causes of Abnormal Axis QRS Axis Possible Cardiac Etiologies Noncardiac Etiologies Normal Normal condition Left (-30 to -90) LVH – Left Ventricular Hypertrophy LAFB – Left Anterior Fascicular Block VT – Ventricular Tachycardia LBBB – Left Bundle Branch Block Inferior wall MI Pneumothorax (mechanical shift) Right (+110 to + 180) Normal young adult and pediatric patients RVH – Right Ventricular Hypertrophy LPFB – Left Posterior Fascicular Block VT – Ventricular Tachycardia Dextrocardia Lateral wall MI COPD and Cor Pulmonale Acute PE Hyperkalemia Extreme Left (-90 to -180) COPD Dextrocardia Right axis deviation • Left posterior fascicular block • Hyperkalemia • Na2+ channel blocking drugs (e.g. TCA’s, Quinidine & Antiarrhythmics) • Right ventricular hypertrophy • Pulmonary HTN - Acute (PE) and chronic (COPD) lung disease • Ventricular ectopy (VT) • Lateral MI (from Q-waves in lead I) • Lead misplacement • Dextrocardia • Normal thin adults with horizontally positioned hearts Simple and tried process 1. Rate 2. Rhythm 3. Axis 4.Intervals 5. ST segments 6. Morphology 7. Special conditions Normal intervals Intervals Normal range PR 0.12 - 0.20 seconds (rate dependent) QRS < 0.10 seconds QT < 450 msec in men < 470 msec in women Rate dependent Age dependent Bazett formula QTc = QT interval/√R-R interval 12 PR intervals 13 PR Intervals 14 QRS intervals 15 QT intervals 16 QT intervals 17 QT interval QT interval Calculations Assessment of QT interval Causes of QT prolongation • Long QT Syndrome – Congenital – Acquired • Medication • Electrolyte imbalance • Ischemia Drugs associated with prolonged QT Simple and tried process 1. 2. 3. 4. Rate Rhythm Axis Intervals 5.ST segments 6. Morphology 7. Special conditions ST Segment deviations ST Segment deviations 18 ST Segment deviations 19 ST Segment deviations 20 ST Segment deviations 21 ST Segment deviations 22 ST Segment deviations 23 ST Segment deviations 24 ST Segment deviations 25 ST Segment deviations 26 ST Segment deviations 27 ST Segment deviations 28 ST Segment deviations 29 STEMIs Territory Leads Coronary involved Anterior STE V1-V4 LAD Lateral STE V3-V6, I, AVL Marginal branch off Cx or Diagnonal off LAD Septal STE V1-V4 LAD – septal branch Inferior STE II, III, AVF RCA (80%) or dominant left Cx (20%) Posterior Big R in V1-V3 STD in V1-V3 STE in V8-V9 Associated with Inferior MI Cx Right ventricle STD in V1-V3 STE in V4r Associated with Inferior MI RCA Inferior MI • Hallmark findings: – STE II, III, AVF – ST depression in AVL – ALWAYS look for concurrent RV MI • STE V1 and/or STDV5,V6 – Get a RIGHT sided EKG (15-lead) • STE-> V4R Inferior/Right sided MI • Be careful with MONA!! RV MI • • • • • Most occur concurrent with inferior MI Remember to get the RIGHT sided EKG! Isolated STE V1 on the routine EKG STE in V4R RV MI is often associated with significant hypotension (preload dependence) Posterior MI • In V1-V3 – Horizontal ST depression – Tall, broad R waves (>30ms) – Upright T waves – Dominant R wave (R/S ratio > 1) in V2 Ddx of ST elevations • • • • • • • • 1-STEMI’s 2-LV Aneurysms 3-LVH 4-LBBB 5-RBBB 6-Paced 7-Pericarditis 8-Early Repolarization Summary Territory Leads Coronary involved Anterior STE V1-V4 LAD Lateral STE V3-V6, I, AVL Marginal branch off Cx or Diagnonal off LAD Septal STE V1-V4 LAD – septal branch Inferior STE II, III, AVF RCA (80%) or dominant left Cx (20%) Posterior Big R in V1-V3 STD in V1-V3 STE in V8-V9 Associated with Inferior MI Cx Right ventricle STD in V1-V3 STE in V4r Associated with Inferior MI RCA Simple and tried process 1. 2. 3. 4. 5. Rate Rhythm Axis Intervals ST segments 6.Morphology 7. Special conditions Left Ventricular Hypertrophy (LVH) LVH, no strain • • • • S in Lead V1 or V2 + R in V5 or V6>35 R in AVL > 11 R in V5 or V6 > 27 Repolarization changes 30 LVH with strain 31 RVH Right Ventricular Hypertrophy 32 • R > S in V1 • R in V1 + S in V6 > 11 • Right axis > 90o • Repolarization changes Bundle Branch Blocks Left Bundle Branch Blocks Left Bundle Branch Block 33 • No Q I, AVL, V6 • RSR1 • QRS predominantly negative in V1 • QRS>0.12 • Repolarization changes Right Bundle Branch Blocks Right Bundle Branch Block 34 • QRS>0.12 • RSR1 lead V1 • QRS predominantly positive in V1 • Wide S in I • Repolarization changes U wave U Wave • Positive deflection that occasionally appears after the T wave • It presence or absence does not signify a pathologic process – Certain disease state make the U wave more prominent Medical conditions • • • • • • • Hypokalemia Hypocalcemia Hypomagnesemia Hypothermia Raised ICP LVH Hypertrophic cardiomyopathy Drugs • • • • Digoxin Phenothiazines Class Ia antiarrhythmics (Quinidine, Procainamide) Class III antiarrhythmics (Amiodarone, Sotalol) U-Wave 35 J wave J wave 36 Simple and tried process 1. 2. 3. 4. 5. 6. 7. Rate Rhythm Axis Intervals ST segments QT interval Morphology 8.Special conditions Normal variants 1. Benign Early Repolarization 2. Athlete’s Heart 3. Persistent Juvenile Pattern Early Repolarization • STE beginning at the J point • STE is minimal (< 2mm) • Upward concave morphology, particularly at the initial portion of the ST segment • Diffusely distributed, mainly V2-V6 • T waves are “peaked” Early Repolarisation 37 Athlete’s Heart • Sinus bradycardia • 1st AV or 2nd AV block (Mobitz I) • Increased R or S voltage • Benign early repolarisation • Deep Q wave in inferior leads Athlete’s Heart 38 Persistent Juvenile Pattern • Healthy children and young adults • Women >>> men • < 40-45 yo • DDx: – Wellens’ disease – Ischemia – PE Persistent Juvenile Pattern 39 Arrhythmias and Dysrrhythmias DO YOU HAVE AN APPROACH TO TACHYARRHYTHMIAS? Approach to Tachy-arrhythmias • Is it Regular or Irregular? • Is it Narrow or Wide Complex? • What is the relationship of the P to the QRS? 48 Regular or Irregular? 49 50 51 52 53 Irregularly irregular rhythms • • • • • Premature atrial or ventricular beats Sinus arrhythmia Multifocal atrial tachycardia Atrial fibrillation Atrial flutter Approach to Tachy-arrhythmias OR Categories of Arrhythmias Supraventricular tachycardias 54 Where are the Ps? 55 Approach to Tachy-arrhythmias • Is it regular or irregular? • Is it narrow or wide complex? • What is the relationship of the P to the QRS? Summary of tachyarrhythmias Regular and Narrow Irregular and Narrow Sinus Tachycardia Atrial Flutter with fixed bloc Paroxysmal Atrial Tachycardia with block SVT Regular and Wide Sinus Arrhythmia Extrasystole Atrial Fibrillation Atrial Flutter with variable bloc Paroxysmal Atrial tachycardia (PAT) MAT (Multifocal Atrial Tachycardia) At least 3 different P waves, one for each QRS Irregular and Wide Above, with aberrancy Above, with aberrancy Hyperkalemia Drug Toxicity VT Ventricular Flutter Hyperkalemia Drug Toxicity Ventricular Tachycardia Torsade VF What rhythm is this? 40 What rhythm is this? 41 What rhythm is this? 43 What rhythm is this? 45 How would you treat this patient? 56 How would you treat this patient? 58 How would you treat this patient? 59 How would you treat this patient? 60 Most important question! Not perfusing Perfusing Narrow complex Narrow complex Synchronized cardioversion Adenosine Calcium Channel Blockers Beta-Blockers Digoxin Wide complex Wide complex Synchronized cardioversion (VT) Defibrillation (VF) Procainamide Amiodarone Synchronized cardioversion Management Rhythm Approach Sinus Tachycardia Treat the cause Premature beats Treat the cause Multifocal atrial tachycardia (MAT) Treat the cause SVT Chemical cardioversion • Adenosine • Calcium channel blockers • Beta-blockers Electrical cardioversion if unstable Atrial fibrillation or flutter Rate control • Adenosine • Calcium channel blockers • Beta-blockers Rhythm control • If < 48h only Anticoagulation Electrical cardioversion if unstable Test 61 Test 63 Test 64 Regular and Narrow Sinus Tachycardia Atrial Flutter with fixed block Atrial tachycardia/SVT P with every QRS Sinus Tachycardia P not with every QRS No P with QRS A. Flutter with fixed block SVT Regular and wide Sinus Tachycardia Atrial Flutter with fixed bloc SVT Hyperkalemia Drug Toxicity VT Ventricular Flutter Aberrancy Irregular and Narrow Sinus Arrhythmia Extrasystole Atrial Fibrillation Atrial Flutter with variable bloc MAT (Multifocal Atrial Tachycardia) PAT Drug toxicity 1 extra beat Extrasystole P with every QRS P with every QRs, but different Not every P conducts a QRS SA MAT Afib or Flutter Regular and wide Sinus Arrhythmia Extrasystole Atrial Fibrillation Atrial Flutter with variable bloc MAT (Multifocal Atrial Tachycardia) Hyperkalemia Drug toxicity Afib or Flutter with Pre-excitation Ventricular Tachycardia Torsade VF Aberrancy Summary of tachyarrhythmias Regular and Narrow Sinus Tachycardia Atrial Flutter with fixed bloc Paroxysmal Atrial Tachycardia with block SVT Regular and Wide Irregular and Narrow Sinus Arrhythmia Extrasystole Atrial Fibrillation Atrial Flutter with variable bloc Paroxysmal Atrial tachycardia (PAT) MAT (Multifocal Atrial Tachycardia) At least 3 different P waves, one for each QRS Irregular and Wide Above, with aberrancy Above, with aberrancy Hyperkalemia Drug Toxicity VT Ventricular Flutter Hyperkalemia Drug Toxicity Ventricular Tachycardia Torsade VF QUESTIONS? DO YOU HAVE AN APPROACH FOR BRADYARRHYTHMIAS? Approach to Brady-arrhythmias • Is the patient stable? Approach to Brady-arrhythmias • Not stable? • Transcutaneous or transvenous Pacemaker Drugs • Dopamine • NorEpineprhine • Epinephrine Heart blocks - Summary Type Characteristics Hemodynamic impact 1st PR longer than 0.20 None Mobitz 1 PR progressively prolongs, then P drops a QRS There is a junctional or ventricular escape beat Min-mod Mobitz 2 PR consistently stays identical, then P drops a QRS There is a junctional or ventricular escape beat Mod-severe Atrial and ventricular rates are independent of one another There is a junctional or ventricular escape beat Mod-severe 2nd 3rd Approach to Brady-arrhythmias • Is the patient stable? • What is the rate? • Are there P waves? • Are the QRS wide? What rhythm is this? 46 1st degree AV block 65 2nd degree AV Block – Mobitz I 66 Wenckebach , Lateral Ischemia 67 Second Degree Type II 2:1 block, RBBB 68 3rd degree AV block 69 3rd Degree AV Block, LVH 70 Heart blocks - Summary Type Characteristics Hemodynamic impact 1st PR longer than 0.20 None Mobitz 1 PR progressively prolongs, then P drops a QRS There is a junctional or ventricular escape beat Min-mod Mobitz 2 PR consistently stays identical, then P drops a QRS There is a junctional or ventricular escape beat Mod-severe Atrial and ventricular rates are independent of one another There is a junctional or ventricular escape beat Mod-severe 2nd 3rd Sinus arrhythmia • • • • P wave does not vary P-P interval varies Usually dependent on respiration If independent of respiration, more commonly pathologic, but may be inconsequential. 71 Sinus pause/arrest • Temporary failure of impulse generation: pause • If prolonged: arrest 72 73 Accelerated idioventricular rhythm • Focus is in the His-bundle branch system or ventricular myocardium • Regular • Rate faster than usual slow idioventricular rhythms 74 SUMMARY Summary of tachyarrhythmias Regular and Narrow Sinus Tachycardia Atrial Flutter with fixed bloc Paroxysmal Atrial Tachycardia with block SVT Regular and Wide Irregular and Narrow Sinus Arrhythmia Extrasystole Atrial Fibrillation Atrial Flutter with variable bloc Paroxysmal Atrial tachycardia (PAT) MAT (Multifocal Atrial Tachycardia) At least 3 different P waves, one for each QRS Irregular and Wide Above, with aberrancy Above, with aberrancy Hyperkalemia Drug Toxicity VT Ventricular Flutter Hyperkalemia Drug Toxicity Ventricular Tachycardia Torsade VF Most important question! Not perfusing Perfusing Narrow complex Narrow complex Synchronized cardioversion Adenosine Calcium Channel Blockers Beta-Blockers Digoxin Wide complex Wide complex Synchronized cardioversion (VT) Defibrillation (VF) Procainamide Amiodarone Synchronized cardioversion Management Rhythm Approach Sinus Tachycardia Treat the cause Premature beats Treat the cause Multifocal atrial tachycardia (MAT) Treat the cause SVT Chemical cardioversion • Adenosine • Calcium channel blockers • Beta-blockers Electrical cardioversion if unstable Atrial fibrillation or flutter Rate control • Adenosine • Calcium channel blockers • Beta-blockers Rhythm control • If < 48h only Anticoagulation Electrical cardioversion if unstable Thank You Questions? [email protected] Interested in More CME on this topic? aafp.org/fmx-cardio