Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
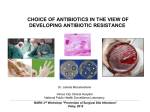
MAJOR ARTICLE Assessment of Antimicrobial Combinations for Klebsiella pneumoniae Carbapenemase– Producing K. pneumoniae Elizabeth B. Hirsch,1,2 Beining Guo,1,4 Kai-Tai Chang,1 Henry Cao,1 Kimberly R. Ledesma,1 Manisha Singh,3 and Vincent H. Tam1 1 University of Houston, Texas; 2Northeastern University, Boston, Massachusetts; 3SUNY-Downstate Medical Center, Brooklyn, New York; and 4Institute of Antibiotics, Huashan Hospital, Fudan University, Shanghai, China Background. The prevalence of blaKPC among gram-negative bacteria continues to increase worldwide. Limited treatment options exist for this multidrug-resistant phenotype, often necessitating combination therapy. We investigated the in vitro and in vivo efficacy of multiple antimicrobial combinations. Methods. Two clinical strains of Klebsiella pneumoniae carbapenemase (KPC)–producing K. pneumoniae were studied. The killing activities of six 2-agent combinations of amikacin, doripenem, levofloxacin, and rifampin were quantitatively assessed using a validated mathematical model. Combination time-kill studies were conducted using clinically relevant concentrations; observed bacterial burdens were modeled using 3-dimensional response surfaces. Selected combinations were further validated in a neutropenic murine pneumonia model, using humanlike dosing exposures. Results. The most enhanced killing effect in time-kill studies was seen with amikacin plus doripenem. Compared with placebo controls, this combination resulted in significant reduction of the bacterial burden in tissue at 24 hours, along with prolonged animal survival. In contrast, amikacin plus levofloxacin was found to be antagonistic in time-kill studies, showing inferior animal survival, as predicted. Conclusions. Our modeling approach appeared to be robust in assessing the effectiveness of various combinations for KPC-producing isolates. Amikacin plus doripenem was the most effective combination in both in vitro and in vivo infection models. Empirical selection of combinations against KPCs may result in antagonism and should be avoided. Keywords. beta-lactamases; combined killing; pharmacodynamics; synergism; AmpC. The frequency of antimicrobial resistance mediated by Klebsiellapneumoniaecarbapenemase(KPC)–producing bacteria is increasing at an alarming rate [1, 2]. Since the first outbreak reports surfaced from the northeastern region of the United States, KPC-harboring isolates have become fairly widespread and have been identified in at least 36 states [3, 4]. In the United Received 22 May 2012; accepted 11 October 2012; electronically published 13 December 2012. Correspondence: Vincent H. Tam, PharmD, Department of Clinical Sciences and Administration, University of Houston College of Pharmacy, 1441 Moursund St, Houston, TX 77030 ([email protected]). The Journal of Infectious Diseases 2013;207:786–93 © The Author 2012. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please e-mail: [email protected]. DOI: 10.1093/infdis/jis766 786 • JID 2013:207 (1 March) • Hirsch et al States, it appears that a single dominant clone, ST 258, accounts for almost 70% of KPC-producing K. pneumoniae isolates in the Center for Disease Control’s pulsed-field gel electrophoresis database [5]. International dissemination rates are also on the rise, with endemic and epidemic situations reported in several countries, including Israel, China, and Greece [1]. KPC-producing isolates represent a significant treatment problem because they are able to hydrolyze a broad spectrum of β-lactam antibiotics. Additional resistance mechanisms (ie, multiple enzymes and porin changes) may also be co-carried in these isolates, conferring cross-resistance to multiple antimicrobial classes [6, 7]. Large susceptibility studies have demonstrated that a great number of KPCharboring isolates are also resistant to the fluoroquinolones, the tetracyclines, selected aminoglycosides, and aztreonam, in addition to most β-lactam agents [8–10]. In general, susceptibility to a few antimicrobials, such as polymyxins and tigecycline, may only be retained [11]. As a result of broad antimicrobial resistance, treatment options are very limited. Further compounding the severity of the problem, high mortality rates have been associated with infection due to KPC-producing organisms, ranging up to 57% in some outbreaks [4, 12]. It has been noted that combination therapy may often be necessary for successful patient outcomes, but data in humans are still lacking and are often limited by retrospective and noncomparative study designs [11]. Several investigations have explored the use of various combination regimens for KPCproducing Enterobacteriaceae, but these investigations often lack fluctuating dosing exposures or in vivo validation [13–17]. It remains unknown which combinations of antimicrobial agents/classes are most effective for the treatment of infection due to KPC-producing organisms. Thus, in an effort to provide a rationale for the selection of effective combination therapy, we chose 4 agents (doripenem, amikacin, levofloxacin, and rifampin) representing various classes and mechanisms of action for this study. In view of the relative stability of doripenem against hydrolysis by KPC, we chose doripenem as our representative carbapenem [18]. The other agents were chosen in part for their favorable rates of in vitro susceptibility or their previously reported synergism against gram-negative organisms [8, 9, 19]. We used these 4 agents to investigate the in vitro and in vivo efficacy of six 2-agent combinations against 2 clinical KPC-producing isolates. METHODS Bacteria One KPC-2–producing isolate (KPVM9) obtained from Brooklyn, New York, and 1 KPC-3–producing isolate (KP6153) obtained from Houston, Texas, were used in the studies. KPVM9 minimum inhibitory concentrations (MICs) for doripenem, amikacin, rifampin, and levofloxacin were 16 mg/L, 64 mg/L, >64 mg/L, and 128 mg/L, respectively. This isolate also possessed SHV-11 and TEM-1 β-lactamases, along with reduced expression of ompK35 [20]. KP6153 MICs for doripenem, amikacin, rifampin, and levofloxacin were 32 mg/L, 32 mg/L, >256 mg/L, and 8 mg/L, respectively. KP6153 also possessed TEM-1 and a TEM-1–like enzyme with a single mutation (E26K), in addition to an SHV-1–like enzyme with a novel mutation (T114A). Furthermore, expression of ompK35 and ompK36 were both downregulated in this isolate. Spectrophotometric studies that used crude cell lysates from each isolate demonstrated effective hydrolysis of imipenem [21]. Real-time reverse transcription polymerase chain reaction studies of KP6153 revealed that KPC transcription was 3 times that of KPVM9. Antimicrobial Agents For in vitro experiments, doripenem, amikacin, rifampin, and levofloxacin were obtained from Peninsula Pharmaceuticals (Alameda, CA), LKT Laboratories (St. Paul, MN), SigmaAldrich (St. Louis, MO), and Waterstone Technologies (Carmel, IN), respectively. Stock solutions of each agent were prepared in sterile water, aliquoted, and stored at −70°C. For in vivo investigations, doripenem, levofloxacin, and amikacin were manufactured by Shionogi (Osaka, Japan), Janssen Pharmaceuticals (Beerse, Belgium), and Sicor Pharmaceuticals (Irvine, CA), respectively. Fresh solutions of each agent were made according to the appropriate concentrations, frozen at −70°C, and thawed immediately prior to administration. Time-Kill Studies and Modeling Single-agent and combination time-kill studies, using approximately 1–5 × 105 colony-forming units (CFU)/mL were conducted in triplicate as previously described [22, 23]. The concentration ranges examined for combination time-kill studies were determined on the basis of optimal sampling and were constrained to those clinically achievable in human serum: amikacin, 4–80 mg/L; doripenem, 4–32 mg/L; levofloxacin, 0.5–10 mg/L; and rifampin, 0.25–6 mg/L. Total bacterial burden at 24 hours (measured in triplicate) was mathematically modeled using a 3-dimensional response surface as described in detail elsewhere (Mathematica 5.2; Wolfram Research, Champaign, IL) [23]. Each experiment was conducted at least twice, on separate days. Volumes under the plane (VUP) of the observed (VUPobserved) and expected (VUPexpected) surfaces were computed by interpolation and double integration, respectively. Confidence intervals (CIs) of VUPobserved were computed with mean data points (±1.96 SDs). Synergy and antagonism were defined as interaction indices (VUPobserved/VUPpredicted) of <1 and >1, respectively. Animals Female Swiss Webster mice weighing 20–25 g (Harlan, Indianapolis, IN) were used in the study. The mice were housed in negative-pressure-ventilated microisolator cages to decrease the risk of infection from extraneous pathogens. Animals were allowed food and water ad libitum. The experimental protocol was approved by the Institutional Animal Care and Use Committee of the University of Houston. Experimental Pneumonia Model Selected combinations from the in vitro model were validated in a neutropenic murine pneumonia model. Details of this model are described elsewhere [24, 25]. Briefly, transient neutropenia was induced in the mice by administering 2 intraperitoneal doses of cyclophosphamide (150 mg/kg 4 days prior to infection and 100 mg/kg 1 day prior to infection) [26]. One intraperitoneal injection of uranyl nitrate (5 mg/kg 2 days KPC Combination Therapy • JID 2013:207 (1 March) • 787 prior to infection) was also administered, to induce transient nephrotoxicity [27]. On the day of infection, the bacterial inoculum was prepared by inoculating a flask containing prewarmed cations adjusted Mueller Hinton broth (Ca-MHB) and placed in a shaker water bath at 35°C until reaching logphase growth. This bacterial suspension was then diluted with Ca-MHB according to absorbance (630 nm), washed with sterile saline, and inoculated (10 µL) into the trachea of anesthetized animals, with laryngoscopic guidance. To adjust for virulence differences between the 2 isolates, lethal inoculum studies were performed before pneumonia studies. Here, mice were infected as described above. A total of 39 mice were randomly divided into 3 groups of 13 mice each. Three different inocula, ranging from 4 × 107 to 5 × 109 CFU/mL, were used for each bacterium. The inoculum resulting in 50%–100% mortality between 24 and 72 hours was used in the subsequent studies. This approach was chosen in an effort to mimic a window of opportunity in which pharmacologic intervention (clinically) may have an impact on patient outcomes. Immune Response Studies Immune response was studied in 12 animals. Six animals were infected as detailed above, while 6 control animals received sterile saline intratracheally. After 24 hours, serum tumor necrosis factor α (TNF-α) and interleukin 6 (IL-6) levels were measured by enzyme-linked immunosorbent assay (OptEIA kit; BD Biosciences, San Diego, CA) according to the manufacturer’s instructions and then compared between the 2 groups. Pharmacokinetic Studies Pharmacokinetic studies to achieve clinically relevant dosing exposures for amikacin (1500 mg every 24 hours) and levofloxacin (750 mg every 24 hours) were previously conducted by our group [24]. To establish human-like dosing exposures for doripenem, 54 mice were infected as described above and divided into 3 different dosing groups: 20, 80, and 200 mg/kg. Two hours after infection, the mice were administered a 0.2-mL (20 and 80 mg/kg) or 0.4-mL (200 mg/kg) intraperitoneal injection of doripenem. For each dosing group, 3 mice were sacrificed by CO2 asphyxiation, and blood was collected via cardiac puncture serially at various time points over 6 hours. After collection, the blood was allowed to clot on ice, and the serum was isolated after centrifugation. Serum was immediately frozen at −70°C (for up to 2 months) until analysis. Drug concentrations were assayed by the validated method described below. Serum doripenem concentrations were then analyzed by fitting a 1-compartment model with first-order absorption to the data. Best-fit model parameter estimates were used to determine the clinically relevant dose exposure. 788 • JID 2013:207 (1 March) • Hirsch et al Drug Assay Doripenem concentrations in mouse serum were assayed using a validated ultraperformance liquid chromatography (UPLC) method after protein precipitation. To a 50-μL aliquot of sample, 20 μL (40 mg/L ertapenem) was added as internal standard, followed by 100 μL acetonitrile. The sample mixtures were mixed and precipitates were removed by centrifugation at 15 000 × g for 15 minutes. The supernatants were recovered and evaporated to dryness at 40°C under air. The dry residue was then reconstituted in 200 μL of 25% acetonitrile (vol/vol) and centrifuged at 15 000 × g for an additional 10 minutes. A 10-μL aliquot of the resulting supernatant solution was injected onto the UPLC system for analysis. The UPLC system consisted of a Waters Acquity UPLC and BEH C18 column (50 mm × 2.1 mm × 1.8 μm, Waters, Milford, MA). Gradient elution was performed using various proportions of mobile phases A (0.1% [vol/vol] formic acid) and B (100% [vol/vol] acetonitrile) at 0.45 mL/min. Doripenem and ertapenem peaks were detected at 305 nm; retention times for doripenem and ertapenem were 1.54 and 1.84 minutes, respectively. The linear range for the assay was 5–80 mg/L, and the intraday and interday variability (calculated as coefficients of variation) were <10% and <16%, respectively. Samples expected to be above the linear range were diluted 5–10-fold with blank mouse serum prior to assay; those expected to be below the range were concentrated 2–3-fold in the final reconstitution step. Assessment of Efficacy Two hours after infection, 16 mice were randomly divided into treatment groups. From each group, 3 mice were sacrificed by CO2 asphyxiation prior drug treatment, to ascertain lung tissue bacterial burden. Antibiotic doses were given by intraperitoneal injections (0.2 mL) as follows: amikacin, 80 mg/kg every 24 hours; doripenem, 120 mg/kg every 8 hours; or levofloxacin, 150 mg/kg every 24 hours. Lung tissues were collected aseptically and homogenized in 10 mL sterile saline; the resulting pellets were resuspended in normal saline to 10 × their original volumes, to minimize the drug carryover effect. After 10-fold serial dilutions, they were then quantitatively cultured on Mueller-Hinton agar plates and incubated for 24 hours, and the bacterial burden in lung tissues were calculated after visual inspection of colony growth. Bacterial burden in lung tissues was assessed for each group at baseline (n = 3), after 24 hours of treatment (n = 3), and at death or the end of the experiment (96 hours). Survival was assessed in 10 mice per treatment group. The mice were examined every 8 hours; at each inspection time, any animals that appeared to be moribund were humanely euthanized. Death was recorded as it occurred, at the next inspection time. Any mice remaining at the end of the 96hour experiment were euthanized by CO2 asphyxiation. Statistical Analysis Lung tissue bacterial burden and serum cytokine levels were analyzed using the Student t test. Survival was evaluated with the Kaplan-Meier survival analysis and log-rank test. A P value of < .05 was considered statistically significant. RESULTS Combination Time-Kill Studies Selected graphical representation of combined killing effects against KPVM9 are shown in Figure 1. The most enhanced killing effect was seen with doripenem plus amikacin (KPVM9, interactive index = 0.60; 95% CI, .56–.65) against both isolates in combination time-kill studies. In contrast, amikacin plus levofloxacin was found to be most antagonistic (interactive index = 1.11; 95% CI, 1.06–1.16) against KPVM9 (Figure 1C). The assessment and ranking of combined killing for all combinations against KPVM9 are shown in Table 1. Interactive indices were not calculated for KP6153, because of an inherent limitation of the model. Reduction in bacterial burden was observed with high (but clinically relevant) drug concentrations. As a result, the predicted combined effect of 2 agents was unrealistic (negative bacterial burden). Consequently, the agent combinations were ranked on the basis of the effect observed with the highest drug concentration combinations (data not shown). Two combination regimens were chosen for in vivo validation: amikacin plus doripenem, because of the synergistic activity seen in vitro, and amikacin plus levofloxacin, because of the interesting antagonistic activity seen. Experimental Pneumonia Validation In mice infected with approximately 2 × 109 CFU/mL of KPVM9 and 6 × 109 CFU/mL of KP6153, mortality was 50% at 72 hours after inoculation. These inocula were used in the subsequent experiments. Serum TNF-α and IL-6 levels were significantly higher in infected mice, compared with control mice; mean TNF-α concentrations (±SD) were 397.3 ± 70.4 pg/mL, compared with 14.7 ± 4.3 pg/mL (P < .001), and mean IL-6 concentrations (±SD) were 25795.4 ± 3348.6 pg/mL, compared with 87.2 ± 66.5 pg/mL (P < .001). These findings were consistent with those observed in acute pneumonia in humans [28]. Figure 1. Graphical representation of the combined killing activity of various antimicrobial combinations against KPVM9. The solid dots denote observed bacterial burdens seen in combination time-kill studies, while the red mesh represents expected bacterial burden of the antimicrobial combination. When a dot (grey) is below the red mesh surface, observed killing is greater than expected killing (ie, synergism). Conversely, when a dot (blue) is above the red mesh surface, observed killing is less than expected killing (ie, antagonism). For each combination, an interactive index was computed by calculating the ratio of the volume under the plane (VUP) between the observed and expected surfaces (ie, VUPobserved/VUPexpected). Synergy and antagonism were defined as interactive indices of <1 and >1, respectively. As shown above, synergism Pharmacokinetics The observed and best-fit pharmacokinetic parameters for doripenem in infected animals are shown in Figure 2. The Figure 1 Continued. was observed with doripenem plus amikacin (A; interactive index = 0.60; 95% confidence interval [CI], 0.56–0.65), while the combination of levofloxacin plus doripenem (B) was viewed to be additive (interactive index = 0.98; 95% CI, 0.98–1.00). On the other hand, the combination of levofloxacin plus amikacin (C) was antagonistic (interactive index = 1.11; 95% CI, 1.06–1.16). KPC Combination Therapy • JID 2013:207 (1 March) • 789 Table 1. Assessment and combinations against KPVM9 ranking of antimicrobial Antimicrobial combination Interactive index (95% CI) Interpretation Doripenem plus amikacin Doripenem plus rifampin 0.60 (.56–.65) 0.99 (.98–1.00) Synergism Additivity Levofloxacin plus rifampin 0.99 (.98–1.00) Additivity Doripenem plus levofloxacin Amikacin plus rifampin 0.98 (.98–1.00) 1.05 (1.03–1.06) Additivity Antagonism Levofloxacin plus amikacin 1.11 (1.06–1.16) Antagonism Synergy and antagonism are defined as an interactive index of <1 and >1, respectively. Abbreviation: CI, confidence interval. model fit to the observed data was reasonable (r 2 > 0.95). On the basis of best-fit model parameter estimates, doripenem was administered at a dose of 120 mg/kg intraperitoneally 3 times daily. This dosing regimen was selected to simulate a clinically relevant pharmacodynamic exposure (a doripenem concentration of ≥1 mg/L 5 hours after the start of an infusion), using a human dose of 500 mg of doripenem over 1 hour. Bacterial Lung Clearance Bacterial burdens in mouse lung tissue observed at 24 hours after infection with either isolate (n = 8 for baseline; n = 3 per treatment group) are shown in Figure 3. In addition to the combination regimens, monotherapy regimens with amikacin and doripenem were also performed for 24 hours, for comparison. As expected, the bacterial burden increased by at least 1 log CFU/g at 24 hours in the absence of treatment, which was comparable to doripenem monotherapy against both isolates. Amikacin monotherapy resulted in increased bacterial burden against KPVM9 but a slight reduction in burden against KP6153. Compared with placebo controls, there were statistically significant decreases in bacterial burden at 24 hours for amikacin plus doripenem for both isolates (P < .01). Animal Survival Figure 4 shows the survival of infected animals after various treatment regimens (n = 10 per treatment group). Bacterial burdens observed in dead animals were significantly higher than those observed at baseline, suggesting pneumonia was likely the primary cause of death (data not shown). Survival was significantly prolonged for doripenem plus amikacin, compared with placebo controls (P < .01), for both isolates. As predicted by the mathematical model, there was an inferior trend in animal survival seen with the amikacin plus levofloxacin combination (Figure 4A; P = .31, compared with placebo control). DISCUSSION Infections caused by KPC-producing organisms are on the rise worldwide and have developed into endemic and epidemic situations in multiple countries [3]. As a result of resistance to multiple classes of antimicrobials, including carbapenems, the treatment of infections due to KPC-producing organisms poses a particular challenge to clinicians [29, 30]. Only limited clinical data are available, and the optimal treatment for such infections is unknown [11]. Although there are experimental compounds in development against KPC-producing bacteria, Figure 2. Single-dose pharmacokinetics of doripenem in infected animals. The open symbols represent experimental observations, while dotted lines represent the best-fit models. The best-fit model parameter estimates were an elimination rate constant (h−1) of 2.547, a volume of distribution (L/kg) of 0.08, and an absorption rate constant (h−1) of 1.47. 790 • JID 2013:207 (1 March) • Hirsch et al Figure 3. Change in tissue bacterial burden from baseline after 24 hours of therapy. Data are shown as mean values (±SD). Abbreviation: CFU, colony-forming units. they may not be commercially available for some time. For example, NXL104 and MK-7655 are both novel β-lactamase inhibitors that have shown in vitro activity in suppressing class A and C enzymes, including KPC-type carbapenemases [31–33]. However, until these agents are available for clinical use, effective treatment options are desperately needed. Previous attempts at pharmacokinetic/pharmacodynamic optimization for antimicrobials against KPC-producing isolates have met with limited success [14, 16, 34, 35]. Prolonged infusion of a high dose of meropenem (one 2-g dose every 8 hours, with each dose administered over 3 hours) was found to be ineffective against 9 of 11 clinical KPC-producing K. pneumoniae isolates in an in vitro pharmacodynamic model [35]. Although this regimen achieved a >3 log CFU/mL reduction against all isolates by 6 hours, regrowth occurred for most of the isolates tested. Similarly, the efficacy of doripenem (human-simulated doses of 1 and 2 g every 8 hours as 4-hour infusions) were evaluated in a murine thigh infection model against 7 KPC-producing K. pneumoniae clinical isolates [34]. A decrease of <1 log CFU was observed in infected mice. In the third approach, doripenem and ertapenem were used in combination against 1 KPC-producing isolate [14]. In these experiments, doripenem 2 g every 8 hours (as 3-hour infusions) plus ertapenem 1 g every 24 hours were simulated. In the in vitro model, there was a modest decrease in bacterial density, but regrowth was seen at the end of the 24-hour experiment. In the thigh infection model, reduction in the bacterial burden in mice treated with doripenem monotherapy (mean bacterial load [±SD], 0.47 ± 0.16 CFU/g) was similar to that observed in untreated immunocompetent mice (0.57 ± 0.33 log CFU/g). Finally, combinations of tigecycline with either meropenem or rifampin were evaluated against 5 clinical KPC-2– or KPC-3–producing K. pneumoniae isolates in an in vitro pharmacodynamic model. Tigecycline (50 mg Figure 4. Survival of animals infected with KPVM9 (A) and KP6153 (B). every 12 hours), meropenem (one 2-g dose every 8 hours, each administered over 3 hours), and rifampin (600 mg every 12 hours) doses simulated steady-state epithelial lining fluid concentrations for each agent. Tigecycline plus meropenem was the most effective combination, but regrowth was seen by 24 hours against the majority of tested isolates. KPC-producing isolates are particularly resilient against antimicrobial therapy. Consequently, our group sought to screen a larger selection of 2-agent combinations possessing varied mechanisms of action. Conventional methods used to study the in vitro interaction between 2 antimicrobial agents, such as the fractional inhibitory concentration index and the checkerboard method, are associated with limitations [36, 37]. In particular, these studies lack prospective validation and are often not useful for predicting clinical outcomes [38]. In the past, our group has performed investigations using a similar mathematical model, followed by in vitro or in vivo validation [22–24]. Our work here is an extension of the previous model used to identify effective combinations against KPC-producing isolates. Here, we studied 2 clinical isolates producing the most prevalent variants of blaKPC, KPC-2 and KPC-3 [1]. These isolates harbor multiple resistance mechanisms, including β-lactamases and outer membrane porin deletions. As predicted by our quantitative method, doripenem plus amikacin was the most effective combination against both isolates. At clinically relevant drug concentrations for both amikacin and doripenem, a considerable synergistic effect was observed after 24-hour time-kill studies (Figure 1A). When neutropenic, infected mice were treated with human-like doses of this combination, KPC Combination Therapy • JID 2013:207 (1 March) • 791 prolonged animal survival also resulted (Figure 4). To our knowledge, this is one of the first polymyxin-sparing combinations found to have a considerable killing effect against KPC-producing isolates. Although the doripenem and amikacin MICs of both isolates were considered non-susceptible, the combination of these two agents resulted in significant activity. In areas where KPC is endemic, use of similar combinations may be helpful, to avoid overuse of polymyxins in an effort to retain their activity against non–KPC-producing multidrug-resistant isolates. Although the mechanistic explanation for the observed synergy between doripenem and amikacin is not entirely known, we hypothesize that this interaction may be due to KPC’s weak hydrolytic activity against doripenem [18]. In contrast to the synergistic activity found, the mathematical model identified the combination of amikacin plus levofloxacin to be antagonistic (Figure 1C) against KPVM9. Animals treated with this combination experienced corresponding inferior survival rates, again validating our mathematical model assessments. This underscores the importance of avoiding the empirical selection of antimicrobial combinations, particularly for infections involving KPC-producing organisms in which high mortality may already be likely [39]. One limitation of the mathematical model was seen in this set of experiments. For KP6153, interactive indices were not calculated. Because significant reductions in bacterial burden were observed with clinically relevant, high single-drug concentrations, the predicted effect of several combinations was unrealistic and resulted in negative bacterial burdens. As a result, the surface response plots were not as helpful in identifying the most promising combinations against KP6153. Second, although favorable results have been shown in our research laboratory, this model is challenging to apply clinically. In the future, the possibility of similar testing may only be applicable in a clinical laboratory, using a scaled-down version that is reasonable to conduct with limited laboratory personnel and/or some level of automation. Furthermore, we chose only 1 representative agent to study for the entire class of antibiotics having the same mechanistic activity; therefore, it is not known whether other combinations of a carbapenem plus aminoglycoside would result in identical results seen with doripenem and amikacin. Last, it is unknown whether the synergistic/antagonistic activities observed against the most prevalent variants (KPC-2/KPC-3) would be identical against other KPC variants or against other isolates with alternative mechanisms of resistance. The future direction of our work will aim to answer several of these questions. In closing, our model appears robust at identifying a promising combination for the treatment of multidrug-resistant KPC-producing isolates. The present study also underscores the importance of avoiding empirical antimicrobial combinations, given that antagonistic effects may result. Exploration of 792 • JID 2013:207 (1 March) • Hirsch et al additional combinations and validation against other KPC variants are warranted. Notes Acknowledgments.We thank Drs David Landman and John Quale (SUNY-Downstate Medical Center, Brooklyn, NY) for the gift of KPVM9 and for their assistance with the molecular characterization of KP6153. Financial support. This work was supported in part by an unrestricted grant from Ortho McNeil-Janssen Pharmaceuticals. Potential conflicts of interest. E. B. H. has received an unrestricted research grant from Pfizer. V. H. T. has received unrestricted research grants from AstraZeneca and Merck and is on the speakers bureau of Merck. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed. References 1. Nordmann P, Cuzon G, Naas T. The real threat of Klebsiella pneumoniae carbapenemase-producing bacteria. Lancet Infect Dis 2009; 9:228–36. 2. Srinivasan A, Patel JB. Klebsiella pneumoniae carbapenemase-producing organisms: an ounce of prevention really is worth a pound of cure. Infect Control Hosp Epidemiol 2008; 29:1107–9. 3. Gupta N, Limbago BM, Patel JB, Kallen AJ. Carbapenem-resistant Enterobacteriaceae: epidemiology and prevention. Clin Infect Dis 2011; 53:60–7. 4. Bratu S, Landman D, Haag R, et al. Rapid spread of carbapenemresistant Klebsiella pneumoniae in New York City: a new threat to our antibiotic armamentarium. Arch Intern Med 2005; 165:1430–5. 5. Kitchel B, Rasheed JK, Patel JB, et al. Molecular epidemiology of KPC-producing Klebsiella pneumoniae isolates in the United States: clonal expansion of multilocus sequence type 258. Antimicrob Agents Chemother 2009; 53:3365–70. 6. Yigit H, Queenan AM, Anderson GJ, et al. Novel carbapenemhydrolyzing beta-lactamase, KPC-1, from a carbapenem-resistant strain of Klebsiella pneumoniae. Antimicrob Agents Chemother 2001; 45:1151–61. 7. Endimiani A, Hujer AM, Perez F, et al. Characterization of blaKPCcontaining Klebsiella pneumoniae isolates detected in different institutions in the Eastern USA. J Antimicrob Chemother 2009; 63:427–37. 8. Castanheira M, Sader HS, Deshpande LM, Fritsche TR, Jones RN. Antimicrobial activities of tigecycline and other broad-spectrum antimicrobials tested against serine carbapenemase- and metallo-betalactamase-producing Enterobacteriaceae: report from the SENTRY Antimicrobial Surveillance Program. Antimicrob Agents Chemother 2008; 52:570–3. 9. Bratu S, Mooty M, Nichani S, et al. Emergence of KPC-possessing Klebsiella pneumoniae in Brooklyn, New York: epidemiology and recommendations for detection. Antimicrob Agents Chemother 2005; 49:3018–20. 10. Bratu S, Tolaney P, Karumudi U, et al. Carbapenemase-producing Klebsiella pneumoniae in Brooklyn, NY: molecular epidemiology and in vitro activity of polymyxin B and other agents. J Antimicrob Chemother 2005; 56:128–32. 11. Hirsch EB, Tam VH. Detection and treatment options for Klebsiella pneumoniae carbapenemases (KPCs): an emerging cause of multidrug-resistant infection. J Antimicrob Chemother 2010; 65:1119–25. 12. Woodford N, Tierno PM Jr., Young K, et al. Outbreak of Klebsiella pneumoniae producing a new carbapenem-hydrolyzing class A betalactamase, KPC-3, in a New York Medical Center. Antimicrob Agents Chemother 2004; 48:4793–9. 13. Le J, McKee B, Srisupha-Olarn W, Burgess DS. In vitro activity of carbapenems alone and in combination with amikacin against KPCproducing Klebsiella pneumoniae. J Clin Med Res 2011; 3:106–10. 14. Bulik CC, Nicolau DP. Double-carbapenem therapy for carbapenemase-producing Klebsiella pneumoniae. Antimicrob Agents Chemother 2011; 55:3002–4. 15. Souli M, Galani I, Boukovalas S, et al. In vitro interactions of antimicrobial combinations with fosfomycin against KPC-2-producing Klebsiella pneumoniae and protection of resistance development. Antimicrob Agents Chemother 2011; 55:2395–7. 16. Wiskirchen DE, Koomanachai P, Nicasio AM, Nicolau DP, Kuti JL. In vitro pharmacodynamics of simulated pulmonary exposures of tigecycline alone and in combination against Klebsiella pneumoniae isolates producing a KPC carbapenemase. Antimicrob Agents Chemother 2011; 55:1420–7. 17. Pournaras S, Vrioni G, Neou E, et al. Activity of tigecycline alone and in combination with colistin and meropenem against Klebsiella pneumoniae carbapenemase (KPC)-producing Enterobacteriaceae strains by time-kill assay. Int J Antimicrob Agents 2011; 37:244–7. 18. Queenan AM, Shang W, Flamm R, Bush K. Hydrolysis and inhibition profiles of {beta}-lactamases from molecular classes A to D with doripenem, imipenem and meropenem. Antimicrob Agents Chemother 2010; 54:565–9. 19. Urban C, Mariano N, Rahal JJ. In vitro double and triple bactericidal activities of doripenem, polymyxin B, and rifampin against multidrugresistant Acinetobacter baumannii, Pseudomonas aeruginosa, Klebsiella pneumoniae, and Escherichia coli. Antimicrob Agents Chemother 2010; 54:2732–4. 20. Landman D, Bratu S, Quale J. Contribution of OmpK36 to carbapenem susceptibility in KPC-producing Klebsiella pneumoniae. J Med Microbiol 2009; 58:1303–8. 21. Hirsch EB, Chang KT, Lasco TM, Caeiro JP, Tam VH. Emergence of KPC-producing Klebsiella pneumoniae in Texas. Diagn Microbiol Infect Dis 2011; 69:234–5. 22. Lim TP, Ledesma KR, Chang KT, et al. Quantitative assessment of combination antimicrobial therapy against multidrug-resistant Acinetobacter baumannii. Antimicrob Agents Chemother 2008; 52: 2898–904. 23. Tam VH, Schilling AN, Lewis RE, Melnick DA, Boucher AN. Novel approach to characterization of combined pharmacodynamic effects of antimicrobial agents. Antimicrob Agents Chemother 2004; 48: 4315–21. 24. Yuan Z, Ledesma KR, Singh R, Hou J, Prince RA, Tam VH. Quantitative assessment of combination antimicrobial therapy against multidrug-resistant bacteria in a murine pneumonia model. J Infect Dis 2010; 201:889–97. 25. Tam VH, Ledesma KR, Schilling AN, et al. In vivo dynamics of carbapenem-resistant Pseudomonas aeruginosa selection after suboptimal dosing. Diagn Microbiol Infect Dis 2009; 64:427–33. 26. Craig WA, Redington J, Ebert SC. Pharmacodynamics of amikacin in vitro and in mouse thigh and lung infections. J Antimicrob Chemother 1991; 27 (Suppl C):29–40. 27. Andes D, Craig WA. In vivo activities of amoxicillin and amoxicillinclavulanate against Streptococcus pneumoniae: application to breakpoint determinations. Antimicrob Agents Chemother 1998; 42:2375–9. 28. Monton C, Torres A, El-Ebiary M, Filella X, Xaubet A, de la Bellacasa JP. Cytokine expression in severe pneumonia: a bronchoalveolar lavage study. Critical Care Medicine 1999; 27:1745–53. 29. Davies TA, Marie Queenan A, Morrow BJ, et al. Longitudinal survey of carbapenem resistance and resistance mechanisms in Enterobacteriaceae and non-fermenters from the USA in 2007–09. J Antimicrob Chemother 2011; 66:2298–307. 30. Landman D, Salamera J, Singh M, Quale J. Accuracy of carbapenem nonsusceptibility for identification of KPC-possessing Enterobacteriaceae by use of the revised CLSI breakpoints. J Clin Microbiol 2011; 49:3931–3. 31. Endimiani A, Choudhary Y, Bonomo RA. In vitro activity of NXL104 in combination with beta-lactams against Klebsiella pneumoniae isolates producing KPC carbapenemases. Antimicrob Agents Chemother 2009; 53:3599–601. 32. Hirsch EB, Ledesma KR, Chang KT, Schwartz MS, Motyl MR, Tam VH. In vitro activity of MK-7655, a novel beta-lactamase inhibitor, in combination with imipenem against carbapenem-resistant Gram-negative bacteria. Antimicrob Agents Chemother 2012; 56:3753–7. 33. Young K, Raghoobar SL, Hairston NN, et al. In vitro activity of the class A and C β-lactamase inhibitor MK-7655. 50th Interscience Conference on Antimicrobial Agents and Chemotherapy. September 12 - 15, 2010. Boston, MA. Abstract F1-2139. 34. Bulik CC, Nicolau DP. In vivo efficacy of simulated human dosing regimens of prolonged-infusion doripenem against carbapenemaseproducing Klebsiella pneumoniae. Antimicrob Agents Chemother 2010; 54:4112–5. 35. Bulik CC, Christensen H, Li P, Sutherland CA, Nicolau DP, Kuti JL. Comparison of the activity of a human simulated, high-dose, prolonged infusion of meropenem against Klebsiella pneumoniae producing the KPC carbapenemase versus that against Pseudomonas aeruginosa in an in vitro pharmacodynamic model. Antimicrob Agents Chemother 2010; 54:804–10. 36. King TC, Schlessinger D, Krogstad DJ. The assessment of antimicrobial combinations. Rev Infect Dis 1981; 3:627–33. 37. Rand KH, Houck HJ, Brown P, Bennett D. Reproducibility of the microdilution checkerboard method for antibiotic synergy. Antimicrob Agents Chemother 1993; 37:613–5. 38. Tan TY, Lim TP, Lee WH, Sasikala S, Hsu LY, Kwa AL. In vitro antibiotic synergy in extensively drug-resistant Acinetobacter baumannii: the effect of testing by time-kill, checkerboard, and Etest methods. Antimicrob Agents Chemother 2011; 55:436–8. 39. Gasink LB, Edelstein PH, Lautenbach E, Synnestvedt M, Fishman NO. Risk factors and clinical impact of Klebsiella pneumoniae carbapenemase-producing K. pneumoniae. Infect Control Hosp Epidemiol 2009; 30:1180–5. KPC Combination Therapy • JID 2013:207 (1 March) • 793