Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Electrocardiography wikipedia , lookup
Echocardiography wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Coronary artery disease wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
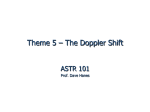
Journal of the American College of Cardiology © 2000 by the American College of Cardiology Published by Elsevier Science Inc. Vol. 36, No. 3, 2000 ISSN 0735-1097/00/$20.00 PII S0735-1097(00)00786-5 New Methods Relation of Tissue Doppler Derived Myocardial Velocities to Myocardial Structure and Beta-Adrenergic Receptor Density in Humans Kesavan Shan, MD,* Roger J. Bick, PHD,‡ Brian J. Poindexter, MSC,‡ Sarah Shimoni, MD,* George V. Letsou, MD,† Michael J. Reardon, MD,† Jimmy F. Howell, MD,† William A. Zoghbi, MD, FACC,* Sherif F. Nagueh, MD, FACC* Houston, Texas We sought to evaluate the relation of segmental tissue Doppler (TD) velocities to both the regional amount of interstitial fibrosis and the myocyte beta-adrenergic receptor density in humans. BACKGROUND The systolic myocardial velocity (Sm) and early diastolic myocardial velocity (Em) acquired by TD are promising new indexes of left ventricular function. However, their structural and functional correlates in humans are still unknown. METHODS Ten patients with coronary artery disease underwent echocardiographic examination including TD imaging, along with transmural endomyocardial biopsy at the time of coronary bypass surgery (two biopsies per patient for a total of 20 specimens). The specimens were analyzed for percent interstitial fibrosis and beta-adrenergic receptor density. RESULTS Normal segments (n ⫽ 8) had a higher beta-adrenoceptor density (2,280 ⫾ 738 vs. 1,373 ⫾ 460, p ⫽ 0.03) and a lower amount of interstitial fibrosis (13 ⫾ 3.3% vs. 28 ⫾ 11.5%, p ⫽ 0.002) than dysfunctional segments (n ⫽ 12). Myocardial systolic velocity and Em were also significantly higher (9.5 ⫾ 2.7 vs. 5.9 ⫾ 1.8 cm/s, p ⫽ 0.025 and 11.3 ⫾ 2.8 vs. 6.4 ⫾ 2.1 cm/s, p ⫽ 0.002, respectively) in normal segments. A significant relationship was present between Em and the beta-adrenergic receptor density (r ⫽ 0.78, p ⬍ 0.001) and percent interstitial fibrosis (r ⫽ ⫺0.7, p ⫽ 0.0026), which together accounted for 81% of the variance observed in Em. Likewise, a significant relationship was present between Sm and the beta-adrenergic receptor density (r ⫽ 0.68, p ⬍ 0.001) and the percent interstitial fibrosis (r ⫽ ⫺0.66, p ⫽ 0.004) and together accounted for 62% of the variance observed in Sm. CONCLUSIONS Systolic myocardial velocity and Em are strongly dependent on both the number of myocytes and the myocardial beta-adrenergic receptor density. (J Am Coll Cardiol 2000;36:891– 6) © 2000 by the American College of Cardiology OBJECTIVES The tissue Doppler (TD) derived myocardial systolic velocity (Sm) and early diastolic velocity (Em) are novel indexes of left ventricular systolic and diastolic performance that can provide important information on both global and regional systolic and diastolic function (1–10). They have also been applied clinically in the diagnosis of coronary artery disease (CAD) in conjunction with stress echocardiography (11). However, to date there are no studies in humans relating these velocities to myocardial structure and the determinants of cardiac contraction and relaxation at the cellular See page 897 level; such information would validate the utility of these velocities as indexes of myocardial function. Regional function is dependent on the number of normally functioning myocytes and is reduced with myocyte necrosis From the *Department of Medicine, Section of Cardiology, Baylor College of Medicine; †Department of Surgery, Baylor College of Medicine; and the ‡Department of Pathology, University of Texas Medical School, Houston, Texas. Manuscript received October 19, 1999; revised manuscript received January 17, 2000, accepted April 19, 2000. and replacement fibrosis. It is also dependent on the adrenergic nervous system and the circulating catecholamines, which play an important role in regulating the myocardial inotropic and lusitropic states at rest and with exercise. Recently, alterations in myocyte beta-adrenergic receptor density were described in diseases associated with myocardial dysfunction (12,13). Specifically, myocardial beta-adrenergic receptor density and cyclic AMP are reduced in chronic heart failure contributing to the decrease in myocardial contractility and the impaired relaxation noted in patients with this disease. Alternatively, transgenic mice overexpressing the beta-2-adrenergic receptors exhibit enhanced cardiac function (14). Our objective, therefore, was to evaluate the relation of segmental TD velocities to the regional amount of interstitial fibrosis and the myocyte betaadrenergic receptor density in patients who had known CAD and left ventricular regional dysfunction who were scheduled to undergo coronary artery bypass surgery. METHODS Ten consecutive patients with stable CAD and regional left ventricular dysfunction in the distribution of one or more 892 Shan et al. Tissue Doppler Velocities and Beta-Adrenoceptors Abbreviations and Acronyms Am ⫽ late diastolic velocity CAD ⫽ coronary artery disease Em ⫽ early diastolic velocity Sm ⫽ myocardial systolic velocity TD ⫽ tissue Doppler TEE ⫽ transesophageal echocardiography coronary arteries (ⱖ70% diameter stenosis), already scheduled for coronary artery bypass surgery, were prospectively enrolled in this investigation. The protocol was approved by the Baylor College of Medicine Affiliated Hospitals Institutional Review Board, and all subjects provided written informed consent before participation. Two to five days before surgery, patients underwent a two-dimensional and TD echocardiographic examination. At surgery and before cardioplegia, transmural myocardial biopsies were obtained from the core of the myocardial segments of interest. Areas of interest were determined a priori as segments with normal or depressed function from transthoracic studies performed before surgery (see below for details). Transesophageal echocardiography (TEE) was utilized to direct the biopsy to the selected segments. These were the same segments in which the TD myocardial velocities were measured. Biopsies were performed with a 20 mm, 14 gauge Tru-Cut biopsy needle. In each patient, two biopsies were acquired. In eight patients, one biopsy was acquired from a normal segment (to serve as control) and another from a dysfunctional segment. However, two patients lacked a normal segment, and biopsies were acquired from two distinct, dysfunctional segments. We defined normal segments as ones meeting all the following criteria: an end-diastolic thickness ⱖ0.9 cm, normal baseline function and a normal contractile reserve (augmented contractility in response to dobutamine without functional deterioration at higher doses) (11). The middle segments of the anterior and lateral walls were biopsied in each patient. The lateral wall was most frequently the normal wall and, thus, served to provide the control segment. In two subjects the sample obtained was only sufficient to analyze the beta-adrenoreceptor density. Echocardiographic studies and analysis. Presurgery images were obtained with either an Acuson (Sequoia, Mountain View, California) or a Hewlett-Packard (Sonos 5500, Andover, Massachusetts) ultrasound system equipped with the TD program. A complete echocardiographic study was performed using standard views. The TD program was applied in the pulse wave mode, and a 5 mm sample volume was placed in the center of each myocardial segment of interest identified by color-coded TD in the apical views. Gains and filters were adjusted as needed to eliminate background noise and allow for a clear tissue signal. Tissue Doppler velocities (range set from ⫺30 to 30 cm/s) were recorded for 5 to 10 cardiac cycles at a sweep speed of 100 mm/s and stored on videotape for later analysis. The JACC Vol. 36, No. 3, 2000 September 2000:891–6 A B A B Figure 1. (Top panel) Fluorescent labeling of beta-adrenoreceptors (green) and nuclei (blue with 4ⴕ6ⴕ-diamidino-2-phenylindole chloride, 0.1 g/ml). (A) Normal segment (B) Dysfunctional segment. (Middle panel) Mallory’s trichrome stain for interstitial fibrosis. (A) Normal segment; (B) Dysfunctional segment. (Lower panel) Tissue Doppler velocities. Am ⫽ late diastolic myocardial velocity; Em ⫽ early diastolic myocardial velocity; Sm ⫽ systolic myocardial velocity; from normal (A) and dysfunctional (B) segments. Notice the higher beta-adrenergic receptor density, the lower amount of interstitial fibrosis and the preserved Sm and Em velocities in the normal segment. position of the pulse wave Doppler sample volume was always in the midsegments of the anterior (A2), lateral (L2), posterior (P2) and inferior (I2) walls. Regional TD derived velocities were analyzed by a single observer blinded to the pathology data using a computerized station (Digisonics 500, Houston, Texas) to determine Sm, Em and late diastolic velocities (Am) (Fig. 1, bottom panel) (intraobserver variability 8 ⫾ 3%). Myocardial systolic velocity was measured ⬎50 ms from onset of the QRS complex to exclude velocity shifts occurring during isovolumic contraction (6,7,11). Pathological analysis. Visualization and quantification of beta receptors. All pathological analysis was performed by experienced pathologists who were blinded to all other data. Fresh biopsy samples of cardiac tissue were embedded in media containing 10.24% polyvinyl alcohol, 4.2% polyeth- JACC Vol. 36, No. 3, 2000 September 2000:891–6 ylene glycol and 85.5% sucrose (O.C.T. Compound TissueTek, Torrance, California) and placed on dry ice to freeze. The blocks were housed at 4°C in a Reichert Histo STAT chryotome and sectioned with a diamond knife at a thickness of 10 ⫾ 3 m. Sections were attached to 18 mm circular glass coverslips coated with Poly-L-Lysine (Sigma) and placed in 3.7% paraformaldehyde for 5 min at room temperature. Tissue slices were visualized using an Applied Precision DeltaVision Scanning Fluorescence Microscope (Issaquah, Washington) fitted with an Olympus IX70 microscope and deconvolution capabilities. The probe used was a green fluorescent BODIPY FL labeled analogue of the betaadrenergic receptor agonist CGP 12177 (Molecular Probes, Eugene, Oregon) (15,16). The sections were stained with the fluorescent receptor probe for 30 min at 37°C and placed on a glass slide on one drop of ethanol. Samples were visualized at a slice thickness of 0.25 mm, with the appropriate number of slices being acquired to pass from bottom to top of the tissue. After acquisition, the image was subjected to deconvolution (five iterations), then stacked and volume rendered with Imaris software (Bitplane AG, Zurich, Switzerland). The tissue samples were also stained with anti-actin antibodies, and secondary antibodies were tagged with an appropriate probe, as well as 4⬘6⬘-diamidino-2phenylindole chloride, 0.1 g/ml for visualization of nuclei. So as to not interfere with the excitation/emission windows of individual probes (Molecular Probes), a combination of tags was used. Stereology employed counting of distinct areas of fluorescence in three separate tissue slices after deconvolution and image enhancement (nine magnified fields in total). This methodology allowed delineation of individual receptors for counting (Fig. 1, top panel). Mean values for receptor density were determined per 60 m ⫻ 60 m tissue slices. Cell type recognition. The sections were composed of three types of cells: fibroblasts, endothelial cells and myocytes. To determine the cell types, a combination of probes was used: 4⬘6⬘-diamidino-2-phenylindole chloride, 0.1 g/ml (Molecular Probes) to identify nuclei and a secondary antibody (goat antirabbit or goat antimouse) tagged with either BODIPY or Texas Red to probe smooth muscle actin. Actin and myosin were identified with a BODIPY tagged secondary antibody (goat antirabbit). Smooth muscle actin identified vascular endothelial cells, while actin and myosin patterns and lack of intercalated discs were used to differentiate between myocytes and fibroblasts. Assessment of fibrosis. To determine the extent of fibrosis, after the specimens were fixed in 10% buffered formalin, processed through a series of ethanol solutions, embedded in paraffin and cut into 3 m sections, they were stained with hematoxylin-eosin and Mallory’s trichrome stain. Fibrosis stains purple with trichrome, which distinguishes it from viable myocardium, which stains pink (Fig. 1, middle panel). Fibrosis was quantitated with a computer image Shan et al. Tissue Doppler Velocities and Beta-Adrenoceptors 893 analysis technique using Optima Bioscan software and expressed as a percentage of the total biopsied section (17). Statistics. Data are presented as mean ⫾ SD. Two tailed unpaired t testing was applied to compare beta-adrenergic receptor density, percent interstitial fibrosis and TD velocities between normal and abnormal segments. Linear regression analysis was used to correlate TD velocities with beta-adrenergic receptor density and percent interstitial fibrosis. Significance was set at a p value ⱕ0.05. RESULTS The study group had a mean age of 61 ⫾ 7 years (range: 54 to 70, five women) and a mean ejection fraction of 32 ⫾ 10% (range: 20% to 45%). All except two patients had angina, and 8/10 had hypertension. The mean New York Heart Association class was 1.6 ⫾ 0.9 (range: 1 to 3). Five patients had three-vessel disease; three had two-vessel disease (one patient with left anterior descending and circumflex disease; the other two, circumflex and right coronary disease), and two had single vessel disease involving the proximal segment of the left anterior descending coronary artery. All patients were on nitrates; one patient was receiving beta-blockers, and three were on calcium channel blockers. Relation of TD velocities to beta-adrenergic receptor density and interstitial fibrosis. The beta-adrenergic receptors were located predominantly in the myocardium and not in the interstitial space. A weak, inverse and nonsignificant correlation was present between the beta-adrenergic receptor density and the percent of interstitial fibrosis (r ⫽ ⫺0.3, R2 ⫽ 0.1, p ⫽ 0.12). Receptor density ranged from 704 to 3,200 and averaged 1,648 ⫾ 705 per 60 m ⫻ 60 m tissue slices. The percent interstitial fibrosis ranged between 7% and 53%. Normal segments (n ⫽ 8), when compared with dysfunctional (n ⫽ 12) segments, exhibited a significantly higher beta-adrenergic receptor density (2,280 ⫾ 738 vs. 1,373 ⫾ 460, p ⫽ 0.03) and a significantly lower percent of interstitial fibrosis (13 ⫾ 3.3% vs. 28 ⫾ 11.5%, p ⫽ 0.002). Tissue Doppler velocities were satisfactorily recorded from all biopsied segments. In comparison with the 12 dysfunctional segments, the 8 normal segments had higher TD velocities (Sm normals: 9.5 ⫾ 2.7 vs. 5.9 ⫾ 1.8 cm/s for dysfunctional segments, p ⫽ 0.025; Em normals: 11.3 ⫾ 2.8 vs. 6.4 ⫾ 2.1 cm/s for dysfunctional segments, p ⫽ 0.002; Am normals: 13.5 ⫾ 6 vs. 8.2 ⫾ 2.5 cm/s for abnormal segments, p ⫽ 0.1). In the 20 segments combined, a significant relation was present between the beta-adrenergic receptor density and segmental Em velocity (r ⫽ 0.78, R2 ⫽ 0.59, p ⬍ 0.001, Fig. 2), with a significant relation also noted between Em and the percent of interstitial fibrosis (r ⫽ ⫺0.7, R2 ⫽ 0.49, p ⫽ 0.0026, Fig. 2). On multiple regression analysis, the beta-adrenergic receptor density and the percent of interstitial fibrosis accounted for 81% of the variance observed in Em (r ⫽ 0.9, R2 ⫽ 0.81, p ⬍ 0.001). Even within the eight 894 Shan et al. Tissue Doppler Velocities and Beta-Adrenoceptors Figure 2. (Upper panel) Relation of Em to beta-adrenoreceptor density. (Lower panel) Relation of Em to the percent of interstitial fibrosis. Em ⫽ early diastolic velocity. normal segments, Em still related significantly to both beta-adrenoceptor density (r ⫽ 0.79, p ⫽ 0.007) and the percent interstitial fibrosis (r ⫽ ⫺0.75, p ⫽ 0.03). Likewise, Em related to these two variables on analyzing the 12 abnormal segments alone (beta-adrenoceptor density: r ⫽ 0.75, p ⫽ 0.01; percent interstitial fibrosis: r ⫽ ⫺0.64, p ⫽ 0.08). Regarding Sm, significant relations were present with the percent of interstitial fibrosis (r ⫽ ⫺0.66, R2 ⫽ 0.44, p ⫽ 0.004, Fig. 3) and beta-adrenoceptor density (r ⫽ 0.68, R2 ⫽ 0.46, p ⬍ 0.001, Fig. 3). On multiple regression analysis, beta-adrenergic receptor density and percent of interstitial fibrosis accounted for 62% of the variance observed in Sm (r ⫽ 0.79, R2 ⫽ 0.62, p ⫽ 0.001). Similar to the findings with Em velocity, Sm showed inverse relations with percent interstitial fibrosis in normal (n ⫽ 8, r ⫽ ⫺0.62, p ⫽ 0.16) and dysfunctional segments (n ⫽ 12, r ⫽ ⫺0.8, p ⫽ 0.05). Myocardial systolic velocity also showed a positive relation with beta-adrenoceptor density in dysfunctional (r ⫽ 0.75, p ⫽ 0.05) and normal segments (r ⫽ 0.59, p ⫽ 0.2). Overall, Am had only a weak insignificant relation with the percent of interstitial fibrosis (r ⫽ ⫺0.43, p ⫽ 0.126). Myocardial systolic velocity (7.9 ⫾ 4 to 9.5 ⫾ 5, n ⫽ 20, p ⬍ 0.05) and Em (8.8 ⫾ 4.5 to 10.8 ⫾ 4.7, n ⫽ 20, p ⬍ 0.05) both significantly increased with low dose dobut- JACC Vol. 36, No. 3, 2000 September 2000:891–6 Figure 3. (Upper panel) Relation of Sm to beta-adrenoreceptor density. (Lower panel) Relation of Sm to the percent of interstitial fibrosis. Sm ⫽ myocardial systolic velocity. amine, whereas Am (11 ⫾ 5.9 to 9.9 ⫾ 5.7, n ⫽ 20, p ⫽ 0.4) did not. A significant relation was also present when Sm and Em changes with low dose dobutamine were related to interstitial fibrosis (r ⫽ ⫺0.72, ⫺0.68, respectively, both p ⬍ 0.04) and beta-adrenergic receptor density (r ⫽ 0.74, 0.73, respectively, both p ⬍ 0.03). DISCUSSION We have shown for the first time that Em and Sm are strongly dependent on both the percent of interstitial fibrosis and the myocardial beta-adrenergic receptor density. It is interesting that even on analyzing the abnormal (or normal) segments alone, Sm and Em related to the percent of interstitial fibrosis and beta-adrenoceptor density. We believe that the weak insignificant relation of fibrosis with beta-adrenoceptor density and the incremental predictive value of both parameters on multiple regression analysis are further proof that the decline in beta receptor density in abnormal segments is not merely due to replacement of myocytes by fibrous tissue but is the result of the decrease in the number of beta receptors per myocyte. In our patient cohort, as the amount of interstitial fibrosis increased, Sm and Em decreased. Because myocyte contraction determines the regional systolic function, it is not surprising that we found an inverse relation between the JACC Vol. 36, No. 3, 2000 September 2000:891–6 extent of regional interstitial fibrosis and segmental Sm. Likewise, the finding of a negative relation between interstitial fibrosis and Em supports the ventricular myocytes contribution to regional Em velocity. This helps explain the abnormal early diastolic wall motion of dysfunctional segments in patients with CAD and myocardial infarction. Such abnormal segments frequently exhibit reduced outward motion in early diastole and may actually move inwards during filling, a finding that has been applied to diagnose CAD with reasonable accuracy (18). It is generally accepted that in the human heart betaadrenergic receptors coupled with adenylate cyclase mediate positive inotropic effects on isolated ventricular muscle preparations (19). Furthermore, the downregulation of cardiac beta-adrenergic receptors in heart failure may significantly contribute to the impaired contractility frequently present in these patients (13,20). Therefore, in our investigation, cardiac segments with a higher beta-adrenergic receptor density had better contractility as manifested by the Sm velocity. Regarding Em velocity, our study shows that this novel parameter of myocardial relaxation is dependent on receptors that influence the left ventricular lusitropic state. There is ample evidence that beta-adrenoceptors help myocardial relaxation in humans. Parker et al. (21) reported that beta-adrenergic receptor stimulation in patients with heart failure results in a significant acceleration of isovolumic relaxation even to an extent comparable with that in normal individuals. This has been shown to occur through cAMPdependent phosphorylation of phospholamban and troponin I (22). Phospholamban phosphorylation results in an increase in Ca ATPase activity that pumps Ca into the sarcoplasmic reticulum, thus decreasing the amount of calcium at the contractile proteins. Phosphorylation of troponin I also aids relaxation as it desensitizes the contractile proteins to calcium. Interestingly, Am had no significant relation with the beta-adrenergic receptor density. This finding is in contrast with the strong relation of the receptor density to the other velocities. These observations support the active ventricular myocardium contribution to Sm and Em and suggest that Am is perhaps reflective of passive ventricular motion or maybe more dependent on atrial myocardium function. However, the latter hypothesis remains to be examined. Study limitations. One biopsy was obtained per dysfunctional segment. However, it is our belief that these specimens reflect well the core tissue in the biopsied segments since we used TEE to guide these core biopsies. Although more specimens could have been obtained, this was greatly limited by patient safety. The relation between TD velocities and histopathology data were not perfect with some degree of scatter. This may have been related to some contribution of heart translocation to the actual velocities. Therefore, the correlations could have been improved had we examined Em and Sm gradients. However, TD velocities were recorded from the apical views, where transloca- Shan et al. Tissue Doppler Velocities and Beta-Adrenoceptors 895 tion is expected to have a minimal impact on Sm and Em. Also, TD velocities were not acquired by TEE at the time of surgery. This was done to minimize the contribution of heart translocation, which is typically more prominent after sternotomy. Alternatively, it is possible that other variables like regional energy stores, cytokine levels and contractile proteins, which determine regional function and were not evaluated in our study, accounted for some degree of the scatter. Conclusions. In summary, this investigation provides novel information on the structural and functional correlates of Sm and Em velocities that further support their use as indexes of myocardial function. Acknowledgment The authors thank Ms. Maria E. Frias for her editorial assistance. Reprint requests and correspondence: Dr. Sherif F. Nagueh, 6550 Fannin Street, SM-1246, Houston, Texas 77030-2717. E-mail: [email protected]. REFERENCES 1. Isaaz K, Thompson A, Ethevenot G, Cloez JL, Brembilla B, Pernot C. Doppler echocardiographic measurement of low velocity motion of the left ventricular posterior wall. Am J Cardiol 1989;64:66 –75. 2. Miyatake K, Yamagishi M, Tanaka N, et al. New method for evaluating left ventricular wall motion by color-coded tissue Doppler imaging: in vitro and in vivo studies. J Am Coll Cardiol 1995;25:717–24. 3. Uematsu M, Miyatake K, Tanaka N, et al. Myocardial velocity gradient as a new indicator of regional left ventricular contraction: detection by a two-dimensional tissue Doppler imaging technique. J Am Coll Cardiol 1995;26:217–23. 4. Donovan CL, Armstrong WF, Bach DS. Quantitative Doppler tissue imaging of the left ventricular myocardium: validation in normal subjects. Am Heart J 1995;130:100 – 4. 5. Isaaz K, Munoz del Romeral L, Lee E, Schiller NB. Quantitation of the motion of the cardiac base in normal subjects by Doppler echocardiography. J Am Soc Echocardiogr 1993;6:166 –76. 6. Gorcsan J, III, Gulati VK, Mandarino WA, Katz WE. Color-coded measures of myocardial velocity throughout the cardiac cycle by tissue Doppler imaging to quantify regional left ventricular function. Am Heart J 1996;131:1203–13. 7. Gorcsan J, III, Strum DP, Mandarino WA, Gulati VK, Pinsky MR. Quantitative assessment of alterations in regional left ventricular contractility with color-coded tissue Doppler echocardiography. Comparison with sonomicrometry and pressure-volume relations. Circulation 1997;95:2423–33. 8. Garcia MG, Rodriguez L, Ares M, Griffin BP, Thomas JD, Klein AL. Differentiation of constrictive pericarditis from restrictive cardiomyopathy: assessment of left ventricular diastolic velocities in longitudinal axis by Doppler tissue imaging. J Am Coll Cardiol 1996;27:108 –14. 9. Oki T, Tabata T, Yamada H, et al. Clinical application of pulsed Doppler tissue imaging for assessing abnormal left ventricular relaxation. Am J Cardiol 1997;79:921– 8. 10. Nagueh SF, Middleton KJ, Kopelen HA, Zoghbi WA, Quinones MA. Doppler tissue imaging: a noninvasive technique for evaluation of left ventricular relaxation and estimation of filling pressures. J Am Coll Cardiol 1997;30:1527–33. 11. Katz WE, Gulati VK, Mahler CM, Gorcsan J, III. Quantitative evaluation of the segmental left ventricular response to dobutamine stress by tissue Doppler echocardiography. Am J Cardiol 1997;79: 1036 – 42. 12. Sato S, Sato N, Kudej RK, et al. Beta-adrenergic receptor signaling in stunned myocardium of conscious pigs. J Mol Cell Cardiol 1997;29: 1387– 400. 896 Shan et al. Tissue Doppler Velocities and Beta-Adrenoceptors 13. Bristow MR, Minobe WA, Raynolds MV, et al. Reduced beta 1 receptor messenger RNA abundance in the failing human heart. J Clin Invest 1993;92:2737– 45. 14. Milano CA, Allen LF, Rockman HA, et al. Enhanced myocardial function in transgenic mice overexpressing the beta 2 adrenergic receptor. Science 1994;264:582– 6. 15. Heithier H, Hallmann D, Boege F, et al. Synthesis and properties of fluorescent beta-adrenoceptor ligands. Biochemistry 1994;33:9126 –34. 16. Staehelin M, Simons P, Jaeggi K, Wigger N. CGP-12177: a hydrophilic beta-adrenergic receptor radioligand reveals high affinity binding of agonists to intact cells. J Biol Chem 1983;258:3496 –502. 17. Nagueh SF, Mikati I, Weilbaecher D, et al. Relation of the contractile reserve of hibernating myocardium to myocardial structure in humans. Circulation 1999;100:490 – 6. 18. Bhargava V, Sunnerhagen KS, Rashwan M, Podolin RA, Shabetai R. Detection and quantitation of ischemic left ventricular dysfunction JACC Vol. 36, No. 3, 2000 September 2000:891–6 19. 20. 21. 22. using a new video intensity technique for regional wall motion evaluation. Am Heart J 1990;120:1058 –72. Jones CR, Molenaar P, Summers RJ. New views of human cardiac beta-adrenoceptors. J Mol Cell Cardiol 1989;21:519 –35. Bristow MR. Changes in myocardial and vascular receptors in heart failure. J Am Coll Cardiol 1993;22:61A–71A. Parker JD, Landzberg JS, Bittl JA, Mirsky I, Colucci WS. Effects of beta-adrenergic stimulation with dobutamine on isovolumic relaxation in the normal and failing human left ventricle. Circulation 1991;84: 1040 – 8. Kaumann A, Bartel S, Molenaar P, et al. Activation of beta 2 adrenergic receptors hastens relaxation and mediates phosphorylation of phospholamban, troponin I and C-protein in ventricular myocardium from patients with terminal heart failure. Circulation 1999;99: 65–72.