Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
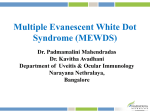
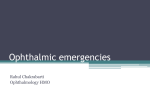
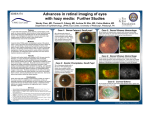
PART 6 RETINA AND VITREOUS SECTION 9 Retinal Detachment/Vitreous Vitreous Anatomy and Pathology J. Sebag 6.46 Definition: Vitreous is an extended extracellular matrix of approximately 4.0 mL in volume and 16.5 mm in axial length (emmetropia) that is situated between the lens and retina. Key features ■ The clear vitreous gel fills the center of the eye, modulates growth of the eye, maintains media transparency, and, during aging, detaches away from the retina, in most cases innocuously. Associated features ■ Anomalous posterior vitreous detachment is the inciting event in rhegmatogenous retinal detachment and vitreomaculopathies (via posterior vitreoschisis), as well as an important contributing factor in proliferative diabetic vitreoretinopathy. INTRODUCTION Although vitreous is the largest structure within the eye, constituting 80% of the ocular volume, investigators of vitreous anatomy are hampered by two fundamental difficulties: ● Any attempts to define vitreous morphology are efforts to “visualize” a tissue that is invisible by design (Fig. 6-46-1). ● The various techniques that were employed previously to define vitreous structure were flawed by artifacts induced by tissue fixatives, which caused precipitation of hyaluronan (formerly called hyaluronic acid), a glycosaminoglycan. The development of slit-lamp biomicroscopy by Gullstrand in 1912 was expected to enable clinical investigation of vitreous structure without the introduction of the aforementioned artifacts. Yet, a widely disparate set of descriptions resulted because of the first of the inherent difficulties just described; that is, the vitreous is largely invisible. This problem even persists in so-called modern investigations. Consider, for example, that in the 1970s Eisner1 described “membranelles” and Worst2 “cisterns,” in the 1980s Sebag and Balazs3, 4 identified “fibers,” and in the 1990s Kishi and Shimizu5 found “pockets” in the vitreous. The discrepant observations of the last-mentioned group have now been explained largely as an age-related phenomenon with no relevance to the inherent macromolecular structure or anatomy.6, 7 Fig. 6-46-1 Vitreous obtained at autopsy from a 9-month-old child. The sclera, choroid, and retina were dissected off the transparent vitreous, which remains attached to the anterior segment. A band of gray tissue can be seen posterior to the ora serrata. This is neural retina that was firmly adherent to the vitreous base and could not be dissected. The vitreous is almost entirely gel (because of the young age of the donor) and thus is solid and maintains its shape, although situated on a surgical towel exposed to room air. (Courtesy of the New England Eye Bank, Boston, MA.) TRIPLE HELIX CONFIGURATION OF THE COLLAGEN MOLECULE 8.6 nm 0.87 nm glycine predominantly imino acids MOLECULAR MORPHOLOGY Supramolecular Organization 766 Vitreous is composed of a dilute meshwork of collagen fibrils (Fig. 6-46-2) with interspersed extensive arrays of long hyaluronan molecules.8–10 The collagen fibrils provide a solid structure that is “inflated” by the hydrophilic hyaluronan.11 Rheological observations also suggest the existence of an important interaction between hyaluronan and collagen.12 Balazs has hypothesized that the hydroxylysine amino acids of Fig. 6-46-2 The triple helix configuration of the collagen molecule. Individual alpha chains are left-handed helices with approximately three residues per turn. The chains themselves, however, are coiled around each other in a right-handed twist. The triple helix configuration is stabilized by hydrogen bonds, which form between opposing residues in different chains (interpeptide hydrogen bonding). (Reprinted with permission from Nimni ME, Harkness RD. Molecular structure and functions of collagen. In: Nimni ME, ed. Collagen, Vol 1. Boca Raton, FL: CRC Press; 1988.) VITREOUS ANATOMY Berger's space (retrolental space of Erggelet) Vitreous Anatomy and Pathology Egger's line forming Wieger's ligament (hyaloideocapsular ligament) 6.46 canal of Hannover pars plicata pars plana ora serrata sclera choroid canal of anterior vitreous Petit vitreous base cortex Fig. 6-46-4 The eye of a 57-year-old man after dissection of the sclera, choroid, and retina, with the vitreous still attached to the anterior segment. The specimen was illuminated with a slit-lamp beam shone from the side and the view here is at a 90° angle to this plane to maximize the Tyndall effect. The anterior segment is below and the posterior pole is at the top of the photograph. A large bundle of prominent fibers courses anteroposteriorly to exit via the premacular dehiscence in the vitreous cortex. retina Cloquet's canal area of Martegiani secondary vitreous Fig. 6-46-3 Vitreous anatomy according to classical anatomic and histological studies. (Reprinted with permission from Schepens CL, Neetens A, eds. The vitreous and vitreoretinal interface. New York: Springer-Verlag; 1987:20.) collagen mediate polysaccharide binding to the collagen chain through O-glycosidic linkages.11 These polar amino acids are present in clusters along the collagen molecule, which perhaps explains why proteoglycans attach to collagen in a periodic pattern.13 Hyaluronan−collagen interaction in the vitreous may be mediated by a third molecule. In cartilage, “link glycoproteins” have been identified that interact with proteoglycans and hyaluronan.14 Supramolecular complexes of these glycoproteins are believed to occupy the interfibrillar spaces. Bishop9 has elegantly described the potential roles of type IX collagen chondroitin sulfate chains, hyaluronan, and opticin in the short-range spacing of collagen fibrils and how these mechanisms might break down in aging and disease. Many investigators believed that hyaluronan−collagen interaction occurs on a “physicochemical” rather than a “chemical” level.15 Reversible complexes of an electrostatic nature between solubilized collagen and various glycosaminoglycans could indeed form, since electrostatic binding between negatively charged hyaluronan and positively charged collagen could occur in vitreous. VITREOUS ANATOMY Macroscopic Morphology In an emmetropic adult human eye the vitreous is approximately 16.5 mm in axial length with a depression anteriorly just behind the lens (patellar fossa). The hyaloideocapsular ligament of Weiger is the annular region (1–2 mm in width and 8–9 mm in diameter) where the vitreous is attached to the posterior aspect of the lens. Erggelet’s or Berger’s space is at the center of the hyaloideocapsular ligament. The canal of Cloquet arises from this space and courses posteriorly through the central vitreous (Fig. 6-46-3), which is the former site of the hyaloid artery in the embryonic vitreous.16 The former lumen of the artery is an area devoid of collagen fibrils and surrounded by multifenestrated sheaths that were previously the basal laminae of the hyaloid artery wall.4 Posteriorly, Cloquet’s canal opens into a funnel-shaped region anterior to the optic disc, known as the area of Martegiani. Fig. 6-46-5 Human vitreous in old age. The central vitreous has thickened, tortuous fibers. The peripheral vitreous has regions devoid of any structure, which contain liquid vitreous. These regions correspond to “lacunae,” as seen clinically using biomicroscopy (arrows). Within the adult human vitreous fine, parallel fibers course in an anteroposterior direction, are continuous, and do not branch (Fig. 6-46-4). The fibers arise from the vitreous base, where they insert anterior and posterior to the ora serrata. Various concepts are used to explain the connection between the peripheral anterior vitreous fibers and the retina and pars plana,4 but all agree that the pathophysiology of retinal tears is vitreous traction upon foci of strong adhesion at the vitreoretinal interface in these locations. As the central fibers near the vitreous cortex course posteriorly, they are circumferential with the vitreous cortex, while central fibers “undulate” in a configuration parallel to Cloquet’s canal. Ultrastructural studies demonstrate that collagen, organized in bundles of packed, parallel fibrils, is the only microscopic structure that corresponds to these fibers.3 It is hypothesized that visible vitreous fibers form when hyaluronan molecules no longer separate the microscopic collagen fibrils, which results in the aggregation of collagen fibrils into bundles from which hyaluronan molecules are excluded.3, 4, 17 The areas adjacent to these large fibers have a low density of collagen fibrils and a relatively high concentration of hyaluronan molecules. Composed primarily of “liquid vitreous,” these areas scatter very little incident light and, when prominent, constitute “lacunae” seen in aging (Fig. 6-46-5). 767 6 MI RETINA AND VITREOUS CF N C A M V B Fig. 6-46-6 Fundus view of posterior vitreous detachment. (A) The posterior vitreous in the left eye of this patient is detached and the prepapillary hole in the posterior vitreous cortex is anterior to the optic disc (arrows, slightly below and to the left of the optic disc here). (B) A slit beam illuminates the retina and optical disc (at bottom) in the center. To the right is the detached vitreous. The posterior vitreous cortex is the dense, whitish gray, vertically oriented linear structure to the right of the slit beam. (Courtesy of CL Trempe, MD.) Microscopic Morphology 768 The vitreous cortex is defined as the peripheral “shell” of the vitreous that courses forward and inward from the anterior vitreous base, the “anterior vitreous cortex,” and posteriorly from the posterior border of the vitreous base, the “posterior vitreous cortex.” The posterior vitreous cortex is 100–110 mm thick and consists of densely packed collagen fibrils.4, 18 Although no direct connections exist between the posterior vitreous and the retina, the posterior vitreous cortex is adherent to the internal limiting lamina of the retina, which is actually the basal lamina of retinal Müller cells. The exact nature of the adhesion between the posterior vitreous cortex and the internal limiting lamina is not known, but it most probably results from the action of various extracellular matrix molecules.19 A hole in the prepapillary vitreous cortex can sometimes be visualized clinically when the posterior vitreous is detached from the retina (Fig. 6-46-6). If peripapillary glial tissue is torn away during posterior vitreous detachment and remains attached to the vitreous cortex about the prepapillary hole, it is referred to as Vogt’s or Weiss’ ring. Vitreous can extrude through the prepapillary hole in the vitreous cortex but does so to a lesser extent than through the premacular vitreous cortex. Various vitreomaculopathies can result.20 Other mechanisms, particularly tangential vitreomacular traction,21 are implicated in the pathogenesis of macular holes. Embedded within the posterior vitreous cortex are hyalocytes. These mononuclear cells are spread widely apart in a single layer situated 20–50 µm from the internal limiting membrane of the retina. The Fig. 6-46-7 Ultrastructure of human hyalocyte. A mononuclear cell is embedded within the dense collagen fibril (CF) network of the vitreous cortex. There is a lobulated nucleus (N) with a dense marginal chromatin (C). In the cytoplasm there are mitochondria (M), dense granules (arrows), vacuoles (V), and microvilli (MI). (Courtesy of Joe Craft and DM Albert, MD.) highest density of hyalocytes is in the vitreous base, followed next by the posterior pole, with the lowest density at the equator. Hyalocytes are oval or spindle shaped, 10–15 µm in diameter, and contain a lobulated nucleus, a well-developed Golgi complex, smooth and rough endoplasmic reticula, many large lysosomal granules (periodic acid-Schiff positive), and phagosomes (Fig. 6-46-7). Balazs11 pointed out that hyalocytes are located in the region of highest hyaluronan concentration and suggested that these cells are responsible for hyaluronan synthesis. Hyalocyte capacity to synthesize collagen was first demonstrated by Newsome et al.22 Thus, in a similar fashion to the chondrocyte metabolism in the joint, hyalocytes may be responsible for vitreous collagen synthesis at some point(s) during life. The phagocytic capacity of hyalocytes is consistent with the presence of pinocytic vesicles and phagosomes and the presence of surface receptors that bind immunoglobulin G and complement.18 It is intriguing to consider that hyalocytes are among the first cells to be exposed to any migratory or mitogenic stimuli during various disease states, particularly proliferative vitreoretinopathy. Therefore, the role of these cells must be considered when the pathophysiology of all proliferative disorders at the vitreoretinal interface is considered, including premacular membrane formation. The basal laminae about the vitreous are composed of type IV collagen closely associated with glycoproteins.18 At the pars plana, the basal lamina has a true lamina densa. The basal lamina posterior to the ora serrata is the internal limiting lamina of the retina. The layer immediately adjacent to the Müller cell is a lamina rara, which is 0.03–0.06 mm thick. The lamina densa is thinnest at the fovea (0.01–0.02 mm) and disc (0.07–0.1 mm). It is thicker elsewhere in the posterior pole (0.5–3.2 mm) than at the equator or vitreous base.4, 18 The anterior surface of the internal limiting lamina (vitreous side) is normally smooth, AGE-RELATED CHANGES Embryology and Postnatal Development Early in embryogenesis, the vitreous is filled with blood vessels, the vasa hyaloidea propria. It is not known what stimulates regression of this hyaloid vascular system, but studies have identified a protein native to vitreous that inhibits angiogenesis in experimental models.24 Teleologically, this seems necessary not only to induce regression of the vascular primary vitreous but also to inhibit subsequent cell migration and proliferation and thereby minimize light scatter and achieve transparency. Identifying the phenomena inherent in this transformation may reveal how to control pathologic neovascularization in the eye and elsewhere. Developmental Anomalies Persistent fetal vascular (PFV) syndrome is an uncommon developmental anomaly in which the hyaloid vasculature system of the primary vitreous fails to involute. This was initially described in detail by Reese25 in his 1955 Jackson Memorial Lecture, at which time the term employed was persistent hyperplastic primary vitreous (PHPV). Goldberg26 revisited this condition in his 1997 Jackson Memorial Lecture and coined the term PFV. There is a spectrum of PFV severity, ranging from pupillary strands and a Mittendorf’s dot to a dense retrolenticular membrane and/or retinal detachment. Anterior PFV consists of retrolenticular fibrovascular tissue that attaches to the ciliary processes and draws them centrally, inducing cataract formation, shallowing of the anterior chamber, and angle-closure glaucoma. Iris vessel engorgement and recurrent intraocular hemorrhage can result in phthisis bulbi, although the prognosis with surgery is often fair. In a recent series27 of operated eyes (both anterior and posterior PFV, n = 83), all of the successful cases (visual acuity of 20/70 or better, n = 12/83) were in anterior PFV. Posterior PFV consists of a prominent vitreous fibrovascular stalk that emanates from the optic nerve and courses anteriorly. Preretinal membranes at the base of the stalk are common, often with tractional retinal folds and traction retinal detachment. The prognosis for posterior PFV is poor, suggesting that pharmacotherapy may be the only solution for this form of PFV. In this regard, it has recently been proposed that insufficient levels of vitreous endostatin may be important in the pathogenesis of PFV.28 Proper vitreous biosynthesis during embryogenesis depends upon normal retinal development because at least some of the vitreous structural components are synthesized by retinal Müller cells.22 A clear gel, typical of normal “secondary vitreous,” appears only over normally developed retina. Thus, in various developmental anomalies, such as retinopathy of prematurity (ROP), familial exudative vitreoretinopathy, and related entities, vitreous that overlies undeveloped retina in the peripheral fundus is a viscous liquid and not a gel. The extent of this finding depends, at least in ROP, upon the gestational age at birth, because the younger the individual the less developed retina is present in the periphery, especially temporally. In other, truly congenital conditions, there are inborn errors of collagen metabolism that have now been elucidated. In Stickler syndrome, defects in specific genes have been associated with particular phenotypes,29 thus enabling the classification of patients with Stickler syndrome into four subgroups. Patients in the subgroups with vitreous abnormalities are found to have defects in the genes coding for type II procollagen and type V/XI procollagen. Ongoing synthesis of both collagen and hyaluronan occurs during development to the adult. Because the synthesis of collagen keeps pace with increasing vitreous volume, the overall concentration of collagen within the vitreous is unchanged during this period of life. Total collagen content in the gel vitreous decreases during the first few years of life and then remains at about 0.05 mg until the third decade.45 Because collagen concentration does not increase appreciably as the size of the vitreous increases, the network density of collagen fibrils effectively decreases. This could potentially weaken the collagen network and destabilize the gel. However, as net synthesis of hyaluronan occurs during this time, the dramatic increase in hyaluronan concentration “stabilizes” the thinning collagen network.17, 19 6.46 Vitreous Anatomy and Pathology whereas the posterior aspect is irregular, as it fills the spaces created by the irregular surface of the subjacent retinal glial cells. This feature is most marked at the posterior pole, whereas in the periphery both the anterior and posterior aspects of the internal limiting lamina are smooth. The significance, if any, of this topographic variation is not known. At the rim of the optic disc the retinal internal limiting lamina ceases, although the basal lamina continues as the “inner limiting membrane of Elschnig.”23 This membrane is 50 mm thick and is believed to be the basal lamina of the astroglia in the papilla. At the central-most portion of the optic disc the membrane thins to 20 mm, follows the irregularities of the underlying cells of the optic nerve head, and is composed only of glycosaminoglycans with no collagen.23 This structure is known as the “central meniscus of Kuhnt.” The thinness and chemical composition of these structures may account for, among other phenomena, the frequency with which abnormal cell proliferation arises from or near the optic disc in proliferative diabetic retinopathy and premacular membranes with macular pucker. The vitreous is known to be most firmly attached at the vitreous base, disc, and macula and over retinal blood vessels. The posterior aspect (retinal side) of the internal limiting lamina demonstrates irregular thickening the farther posteriorly from the ora serrata.4, 18 So-called attachment plaques between the Müller cells and the internal limiting lamina have been described in the basal and equatorial regions of the fundus but not in the posterior pole, except for the fovea.4, 18 It has been hypothesized that these develop in response to vitreous traction upon the retina. The thick internal limiting lamina in the posterior pole dampens the effects of this traction, except at the fovea, where the internal limiting lamina is thin. The thinness of the internal limiting lamina and the purported presence of attachment plaques at the central macula could explain the predisposition of this region to changes induced by traction. An unusual vitreoretinal interface overlies retinal blood vessels. Physiologically, this may provide a shock-absorbing function to dampen arterial pulsations. However, pathologically, this structural arrangement could also account for the proliferative and hemorrhagic events upon retinal blood vessels that are associated with vitreous traction. Aging of the Vitreous Substantial rheological, biochemical, and structural alterations occur in the vitreous during aging.30, 31 After 45–50 years of age a significant decrease occurs in the gel volume and an increase in the liquid volume of human vitreous. These findings were confirmed qualitatively in postmortem studies of dissected human vitreous, and liquefaction was observed to begin in the central vitreous.1,4–6 Vitreous liquefaction actually begins much earlier than the ages at which clinical examination or ultrasonography detects changes. Postmortem studies found evidence of liquid vitreous in eyes at 4 years of age and observed that by the time the human eye reaches its adult size (age 14–18 years) approximately 20% of the total vitreous volume consists of liquid vitreous.30 In these postmortem studies of fresh, unfixed human eyes it was observed that after the age of 40 years a steady increase occurs in liquid vitreous simultaneously with a decrease in gel volume. By 80–90 years of age more than half the vitreous is liquid. The finding that the central vitreous is where fibers are first observed is consistent with the concept that breakdown of the normal hyaluronan-collagen association results in the simultaneous formation of liquid vitreous and aggregation of collagen fibrils into bundles of parallel fibrils, seen as large fibers (see Fig. 6-46-4).1, 4–6 In the posterior vitreous such age-related changes often form large pockets of liquid vitreous, recognized clinically as lacunae,4–6 and mistakenly described as anatomic structures.5–7 The mechanism of vitreous liquefaction is not understood. Gel vitreous can be liquefied in vivo through the removal of collagen by enzymatic destruction of the collagen network.32 Endogenous liquefaction may be the result of changes in the minor glycosaminoglycans and chondroitin sulfate profile of vitreous. It has been shown that the injection of chondroitinase ABC can induce liquefaction and “disinsertion” of the vitreous.33 Plasmin is another agent being developed as an adjunct to vitreoretinal surgery34 because of its purported ability to induce liquefaction of the central vitreous and dehiscence at the vitreoretinal interface. Another possible mechanism of vitreous liquefaction is a change in the conformation of hyaluronan molecules with aggregation or cross-linking of collagen molecules. Singlet oxygen can induce conformational changes in the tertiary structure of hyaluronan molecules. Free radicals generated by metabolic and photosensitized reactions could alter hyaluronan and/or collagen structure and trigger a dissociation of collagen and hyaluronan molecules, which ultimately results in liquefaction.35 This is plausible because the cumulative effects of a lifetime of daily exposure to light may influence the structure and interaction of collagen and hyaluronan molecules by the proposed free radical mechanism(s). 769 confirmed posterior migration of the posterior border of the vitreous base during aging and also demonstrated intraretinal synthesis of collagen fibrils that penetrate the internal limiting of the retina and “splice” with vitreous collagen fibrils. These aging changes at the vitreous base could contribute to increased traction on the peripheral retina and to the development of retinal tears and detachment. 6 RETINA AND VITREOUS Posterior Vitreous Detachment A B Fig. 6-46-8 Vitreous structure in childhood. (A) The posterior and central vitreous in a 4-year-old child has a dense vitreous cortex with hyalocytes. A substantial amount of vitreous extrudes into the retrocortical (preretinal) space through the premacular vitreous cortex. However, no fibers are present in the vitreous. (B) Central vitreous structure in an 11-year-old child has hyalocytes in a dense vitreous cortex (arrows). No fibers are seen within the vitreous. The most common age-related event in the vitreous is PVD.40 True PVD can be defined as a separation between the posterior vitreous cortex and the internal limiting lamina of the retina; PVD can be localized, partial, or total (up to the posterior border of the vitreous base). Autopsy studies reveal that the incidence of PVD is 63% by the eighth decade,41 and it is more common in myopic eyes, in which it occurs on average 10 years earlier than in emmetropic and hyperopic eyes. Cataract extraction in myopic patients introduces additional effects, which caused PVD to develop in all but 1 of 103 myopic (greater than −6 D) eyes.4 Rheologic changes within the vitreous produce liquefaction, which, in conjunction with weakening of the vitreous cortex-internal limiting laminar adhesion, results in PVD. It is likely that dissolution of the posterior vitreous cortex−internal limiting laminar adhesion at the posterior pole allows liquid vitreous to enter the retrocortical space via the prepapillary hole and perhaps also the premacular vitreous cortex. With rotational eye movements, liquid vitreous can dissect a plane between the vitreous cortex and the internal limiting lamina, which results in true PVD. This volume displacement from the central vitreous to the preretinal space causes the observed collapse of the vitreous body (syneresis). Glare may be induced by PVD because of light scattering by the dense collagen fibril network in the posterior vitreous cortex. “Floaters” are the most common complaint of patients with PVD. These usually result from entoptic phenomena caused by condensed vitreous fibers, glial tissue of epipapillary origin (which adheres to the posterior vitreous cortex), and/or intravitreal blood. Floaters move with vitreous displacement during eye movement and scatter incident light, which casts a shadow on the retina that is perceived as a gray, “hairlike” or “fly-like” structure. In 1935, Moore42 described “light flashes” as a common complaint that results from PVD. Wise43 noted that light flashes occurred in 50% of cases at the time of PVD; they were usually vertical and temporally located. Voerhoeff44 suggested that the light flashes result from the impact of the detached posterior vitreous cortex upon the retina during eye movement. Anomalous Posterior Vitreous Detachment 770 Biochemical studies support the rheologic observations. Total vitreous collagen content does not change after 20–30 years of age. However, in studies of a large series of normal human eyes obtained at autopsy, the collagen concentration in the gel vitreous at 70–90 years of age (approximately 0.1 mg/mL) was greater than at 15–20 years of age (approximately 0.05 mg/mL).30 Because the total collagen content does not change, this finding most likely reflects the decrease in the volume of gel vitreous that occurs with aging and consequent increase in the concentration of the collagen that remains in the gel. The collagen fibrils in this gel become packed into bundles of parallel fibrils,3, 4, 17, 31 likely with cross-links between them. Abnormal collagen cross-links have, in fact, been identified in the vitreous of humans who have diabetes, and the findings are consistent with the existence of diabetic vitreopathy36 (see below), a phenomenon that has been described for other extracellular matrices in patients with diabetes. The structural changes that derive from the aforementioned biochemical and rheologic changes consist of a transition from a clear vitreous in youth (Fig. 6-46-8), the consequence of a homogeneous distribution of collagen and hyaluronan, to a fibrous structure in the adult (see Fig. 6-46-4), which results from aggregation of collagen fibrils. In old age advanced liquefaction (see Fig. 6-46-5) occurs with ultimate collapse of the vitreous and posterior vitreous detachment (PVD). The vitreous base posterior to the ora increases in size with increasing age to nearly 3.0 mm, to bring the posterior border of the vitreous base closer to the equator.37 This widening of the vitreous base was found to be most prominent in the temporal portion of the globe. The posterior migration of the vitreous base probably plays an important role in the pathogenesis of peripheral retinal breaks and rhegmatogenous retinal detachment. Within the vitreous base, a “lateral aggregation” of the collagen fibrils is present in older individuals,38 similar to aging changes within the central vitreous.17, 31 Recent studies39 have Anomalous posterior vitreous detachment (APVD)45 occurs when the extent of vitreous liquefaction exceeds the degree of weakening of vitreoretinal adherence and traction is exerted at this interface. There are various causes for an imbalance between the degree of gel liquefaction and weakening of vitreoretinal adhesion. As described above, inborn errors of collagen metabolism, such as those present in Marfan’s, EhlersDanlos, and Stickler’s syndromes,29 result in extreme gel liquefaction at an early age when there is persistent vitreoretinal adherence. The result is a high incidence of large retinal tears and detachments. Systemic conditions such as diabetes induce biochemical46 and structural47 alterations in vitreous. These changes, referred to as diabetic vitreopathy,36 are important in the pathobiology of proliferative diabetic vitreoretinopathy, and perhaps some cases of macular edema as well. Diabetic vitreopathy may one day be detected in vivo using noninvasive optical instrumentation.48, 49 There are also changes associated with myopia, known as myopic vitreopathy, where there is excess vitreous liquefaction for the degree of vitreoretinal adhesion, resulting in anomalous PVD and undue traction at the vitreoretinal interface. Regardless of the underlying cause, abnormal traction at the vitreoretinal interface can have deleterious effects upon retina as well as vitreous (Table 6-46-1). Retinal effects Effects upon the retina vary, depending on the site affected. These include hemorrhage, retinal tears and detachment, and vitreomacular traction syndromes, including macular holes and some cases of diabetic macular edema. Proliferative diabetic retinopathy (PDR) can be aggravated by anomalous PVD. Lindner50 found that vitreous hemorrhage occurred in 13−19% of patients with PVD. Because vitreous hemorrhage results from considerable vitreoretinal traction, this finding in a patient with PVD is generally considered to be an important risk factor TABLE 6-46-1 ANOMALOUS POSTERIOR VITREOUS DETACHMENT Retinal Effects Vitreous Effects Blood vessels Retinal hemorrhages Aggravate retinal neovascularization Vitreous hemorrhage Macula Vitreomacular traction syndrome Diabetic macular edema (diffuse) Vitreoschisis with macular pucker Macular holes Periphery Retinal tears/detachments White without pressure Optic disc Vitreopapillary traction syndrome Aggravate NVD (PDVR, CRVO) 6.46 A CRVO, central retinal vein occlusion; NVD, neovascularization of the optic disc; PDVR, proliferative diabetic vitreoretinopathy. for the presence of a retinal tear and detachment. One 15-year study in Belgium51 found that in 126 cases of nondiabetic, nontraumatic vitreous hemorrhage that did not clear for 6 months, 25% were found to have retinal tears and 8% had retinal detachments. Another study52 found that in 36 eyes with fundus-obscuring vitreous hemorrhage, 24/36 eyes (67%) were found to have at least one retinal break, with 88% of breaks located in the superior retina. Eleven eyes (31%) had more than one retinal break. Fourteen of 36 eyes (39%) had a rhegmatogenous retinal detachment. Retinal tears not involving blood vessels result from traction on other foci of usual vitreoretinal adhesion, such as the posterior border of the vitreous base. Abnormal foci of firm vitreoretinal adhesion, such as lattice degeneration and rosettes, are also frequently associated with retinal tears after PVD. Indeed, Byer53 has claimed that as many as 25% of the general population have some form of abnormal focal vitreoretinal adhesion, placing them at considerable risk from anomalous PVD. Vitreous Anatomy and Pathology Traction Site(s) B Fig. 6-46-9 Diabetic vitreopathy. (A) Right eye of a 9-year-old girl who has a 5-year history of type 1 diabetes shows extrusion of central vitreous through the posterior vitreous cortex into the retrocortical (preretinal) space. The subcortical vitreous appears very dense and scatters light intensely. Centrally, there are vitreous fibers (arrows) with an anteroposterior orientation and adjacent areas of liquefaction. (B) Central vitreous in the left eye of the same patient shows prominent fibers that resemble those seen in nondiabetic adults (see Fig. 6-46-5). (Reprinted with permission from Sebag J. Abnormalities of human vitreous structure in diabetes. Graefes Arch Clin Exp Ophthalmol. 1993;231:257–60.) Vitreous effects Effects upon vitreous primarily involve posterior vitreoschisis.54, 55 This condition results from splitting of the posterior vitreous cortex, with forward displacement of the anterior portion of the posterior vitreous cortex leaving part, or all, of the posterior layer of the split vitreous cortex still attached to the retina. Vitreoschisis has been detected in cases of proliferative diabetic vitreoretinopathy56, 57 and retinovascular diseases,55, 58 and likely has a role in the pathophysiology and sequelae of these conditions.45 Premacular membranes with macular pucker and cases of macular holes may also result from persistent attachment of partial or full-thickness posterior vitreous cortex to the macula while the remainder of the vitreous detaches forward. In the former case, tractional forces are centripetal (inward toward the fovea) causing macular pucker. In the latter condition tangential traction occurs in a centrifugal (outward from the fovea) direction, causing a macular hole.45 METABOLIC DISORDERS OF VITREOUS Diabetic Vitreopathy In humans who have diabetes, there is an increase in vitreous glucose levels.59 These elevated levels of glucose are associated with increased nonenzymatic glycation products in human vitreous collagen and elevated levels of the enzyme-mediated cross-link dihydroxylysinonorleucine.46 Also, considerable diabetic effects may involve hyaluronan. In the daily management of diabetes, significant fluctuations in the systemic concentrations of a variety of molecules may occur, which can alter the ionic milieu of the vitreous. Shifts in systemic metabolism, and in turn osmolarity and hydration of the vitreous, could result in periodic swelling and contraction of the entire vitreous, with consequent traction upon structures attached to the posterior vitreous cortex, such as new blood vessels that have grown out of the optic disc and/or retina.60 These events could influence the course of diabetic retinopathy as they may contribute to the proliferation of neovascular frond and perhaps even induce rupture of the new vessels and cause vitreous hemorrhage. Such molecular effects of diabetes result in morphological changes within the vitreous47 (Fig. 6-46-9). The roles of these and other pathological changes, such as posterior vitreoschisis,55 are being investigated at present. It is hoped that the future will see therapy designed to inhibit diabetic vitreopathy. Alternatively, the induction of innocuous PVD early in the course of diabetic retinopathy may have long-term salubrious effects in patients at great risk. Synchysis Scintillans This condition features vitreous opacification as a consequence of chronic vitreous hemorrhage. These vitreous opacities are noted when frank hemorrhage is no longer present. They appear as flat, refractile bodies, golden brown in color, and are freely mobile. Associated with liquid vitreous, they settle to the most dependent portion of the vitreous when eye movement stops. The vitreous about these opacities is degenerated so that collagen is displaced peripherally. Chemical studies demonstrate the presence of cholesterol crystals in these opacities, and the condition is sometimes referred to as “cholesterolosis bulbi.”61 Free hemoglobin spherules can be present within the vitreous.62 Asteroid Hyalosis This generally benign condition is characterized by small yellow-white spherical opacities throughout the vitreous. The prevalence of asteroid hyalosis was previously found to be 0.042–0.5%, although a recent study63 of 10 801 autopsy eyes found an incidence of 1.96%; it affects all races but with a male-to-female ratio of 2:1. Curiously, asteroid hyalosis is unilateral in over 75% of cases. Asteroid bodies are associated intimately with the vitreous gel and move with typical vitreous displacement during eye movement, which suggests a relationship with collagen fibril degeneration.64 However, PVD, either complete or partial, occurs less frequently in individuals with asteroid hyalosis than in agematched controls,65 which does not support age-related degeneration as a cause. Histological studies demonstrate a crystalline appearance and a pattern of positive staining to fat and acid mucopolysaccharide stains 771 6 RETINA AND VITREOUS that is not affected by hyaluronidase pretreatment.66 Electron diffraction studies showed the presence of calcium oxalate monohydrate and calcium hydroxyphosphate. Ultrastructural studies reveal intertwined ribbons of multilaminar membranes (with a 6 nm periodicity) that are characteristic of complex lipids, especially phospholipids, that lie in a homogeneous background matrix.66 In these investigations, energydispersive x-ray analysis showed calcium and phosphorus to be the main elements in asteroid bodies. Electron diffraction structural analysis demonstrated calcium hydroxyapatite and possibly other forms of calcium phosphate crystals. Some reports suggest an association between asteroid hyalosis and diabetes mellitus,67, 68 while other investigations found no such association.63, 69 Asteroid hyalosis appears to be associated with certain pigmentary retinal degenerations,70 although it is not known whether this is related to the presence of diabetes in these patients. Yu and Blumenthal71 proposed that asteroid hyalosis results from aging collagen, whereas other studies72 suggested that asteroid formation is preceded by depolymerization of hyaluronan. Amyloidosis vitreous involvement in nonfamilial forms have been reported. The opacities first appear in the vitreous adjacent to retinal blood vessels and later appear in the anterior vitreous. Initially, the opacities are granular with wispy fringes and later take on a “glass wool” appearance. When the opacities form strands, they appear to attach to the retina and the posterior aspect of the lens by thick footplates.65 Following PVD, the posterior vitreous cortex is observed to have thick, linear opacities that follow the course of the retinal vessels. The opacities seem to aggregate by “seeding” on vitreous fibrils and along the posterior vitreous cortex.66 Histopathological specimens contain star-like structures with dense, fibrillar centers. The amyloid fibrils are 5–10 nm in diameter and are differentiated from the 10–15 nm vitreous fibrils by stains for amyloid and by the fact that the vitreous fibrils are very straight and long.66 Electron microscopy can confirm the presence of amyloid, and immunocytochemical studies identified the major amyloid constituent as a protein that resembles prealbumin.73 Streeten66 proposed that hyalocytes could perform the role of macrophage processing of the amyloid protein before its polymerization. This may further explain why the opacities initially appear at the posterior vitreous cortex where hyalocytes reside. Amyloidosis can result in the deposition of opacities in the vitreous of one or both eyes. Bilateral involvement can be an early manifestation of the dominant form of familial amyloidosis, although rare cases of REFERENCES 772 1. Eisner G. Biomicroscopy of the peripheral fundus. New York: Springer-Verlag; 1973. 2. Worst JGF. Cisternal systems of the fully developed vitreous body in the young adult. Trans Ophthalmol Soc UK. 1977;97:550–4. 3. Sebag J, Balazs EA. Morphology and ultrastructure of human vitreous fibers. Invest Ophthalmol Vis Sci. 1989;30:187–91. 4. Sebag J. The Vitreous-Structure, Function, and Pathobiology. New York: Springer-Verlag; 1989. 5. Kishi S, Shimizu K. Posterior precortical vitreous pocket. Arch Ophthalmol. 1990;108:979–82. 6. Sebag J. Letter to the editor. Arch Ophthalmol. 1991;109:1059–60. 7. Kakehashi A. Age-related changes in the premacular vitreous cortex. Invest Ophthalmol Vis Sci. 1996;37:2253. 8. Scott JE. The chemical morphology of the vitreous. Eye. 1992;6:553–5. 9. Bishop PN. Structural macromolecules and supramolecular organization of the vitreous gel. Prog Retinal Eye Res.. 2000;19:323–44. 10. Mayne R. The eye. Connective tissue and its heritable disorders, New York: Wiley-Liss; 2001 :131–41. 11. Balazs EA. The vitreous. In: Davson H, ed. The Eye, Vol la. London: Academic Press; 1984. :533–89. 12. Tokita M, Fujiya Y, Hikichi K. Dynamic viscoelasticity of bovine vitreous body. Biorheology. 1984;21:751–65. 13. Asakura A. Histochemistry of hyaluronic acid of the bovine vitreous body as studied by electron microscopy. Acta Soc Ophthalmol Jpn. 1985;89:179–91. 14. Hardingham TE. The role of link-protein in the structure of cartilage-proteoglycan aggregates. Biochem J. 1979; 177:237–47. 15. Comper WD, Laurent TC. Physiological function of connective tissue polysaccharides. Physiol Rev. 1978;58:255–315. 16. Schepens CL, Neetens A, eds. The vitreous and vitreoretinal interface. New York: Springer-Verlag; 1987:20. 17. Sebag J. Age-related changes in human vitreous structure. Graefes Arch Clin Exp Ophthalmol. 1987;225:89–93. 18. Sebag J. Surgical anatomy of vitreous and the vitreoretinal interface. In: Tasman W, Jaeger E, eds. Clinical ophthalmology, Vol 6Philadelphia: JB Lippincott; 1994:1–36. 19. Sebag J. Age-related differences in the human vitreoretinal interface. Arch Ophthalmol. 1991;109:966–71. 20. Sebag J. Anatomy and pathology of the vitreo-retinal interface. Eye. 1992;6:541–52. 21. Gass JDM. Reappraisal of biomicroscopic classification of stages of development of a macular hole. Am J Ophthalmol. 1995;119:752–9. 22. Newsome DA, Linsemayer TF, Trelstad RJ. Vitreous body collagen. Evidence for a dual origin from the neural retina and hyalocytes. J Cell Biol. 1976;71:59–67. 23. Heergaard S, Jensen OA, Prause JU. Structure of the vitreal face of the monkey optic disc. Graefes Arch Clin Exp Ophthalmol. 1988;226:377–83. 24. Lutty GA, Mello RF, Chandler C, et al. Regulation of cell growth by vitreous humor. J Cell Sci. 1985;76:53–65. 25. Reese AB. Persistent hyperplastic primary vitreous. Am J Ophthalmol. 1955;30:317–31. 26. Goldberg MF. Persistent fetal vasculature. Am J Ophthalmol. 1997;124:587–625. 27. Pollard ZF. Persistent hyperplastic primary vitreous − diagnosis, treatment, and results. Trans Am Ophthalmol Soc. 1997;95:487–549. 28. Duh EJ, Yao YG, Dagli M, Goldberg MF. Persistence of fetal vasculature in a patient with Knobloch syndrome − potential role for endostatin in fetal remodeling of the eye. Ophthalmology. 2004;111:1885–8. 29. Snead MP, Yates JRW. Clinical and molecular genetics of Stickler syndrome. J. Med Genet. 1999;36:353–9. 30. Balazs EA, Denlinger JL. Aging changes in the vitreous. In: Aging and human visual function, New York: Alan R Liss; 1982. :45–57. 31. Sebag J. Ageing of the vitreous. Eye. 1987;1:254–62. 32. Aguayo J, Glaser BM, Mildvan A, et al. Study of vitreous liquefaction by NMR spectroscopy and imaging. Invest Ophthalmol Vis Sci.. 1985;26:692–7. 33. Hageman G, Russel S. Chondroitinase-mediated disinsertion of the primate vitreous body. Invest Ophthalmol Vis Sci. 1994;35:1260. 34. Verstraeten TC, Chapman C, Hartzer M, et al. Pharmacologic induction of posterior vitreous detachment in the rabbit. Arch Ophthalmol. 1993;111:849–54. 35. Ueno N, Sebag J, Hirokawa H, Chakrabarti B. Effects of visible light irradiation on vitreous structure in the presence of a photosensitizer. Exp Eye Res. 1987;44:863–70. 36. Sebag J. Diabetic vitreopathy. Ophthalmology. 1996;103:205–6. 37. Teng CC, Chi HH. Vitreous changes and the mechanism of retinal detachment. Am J Ophthalmol. 1957;44:335. 38. Gartner J. Electron microscopic study on the fibrillar network and fibrocyte-collagen interactions in the vitreous cortex at the ora serrata of human eyes with special regard to the role of disintegrating cells. Exp Eye Res. 1986;42:21–33. 39. Wang J, McLeod D, Henson DB, Bishop PN. Age-dependent changes in the basal retinovitreal adhesion. Invest Ophthalmol Vis Sci. 2003;44:1793. 40. Sebag J. Classifying posterior vitreous detachment − a new way to look at the invisible. Br J Ophthalmol. 1997;81:521. 41. Foos RY. Posterior vitreous detachment. Trans Am Acad Ophthalmol Otolaryngol. 1974;76:480–96. 42. Moore RF. Subjective ‘lightening streak’. Br J Ophthalmol.1935:545–50. 43. Wise GN. Relationship of idiopathic preretinal macular fibrosis to posterior vitreous detachment. Am J Ophthalmol. 1975;79:358–61. 44. Voerhoeff FH. Are Moore’s lightening streaks of serious portent?. Am J Ophthalmol. 1956;41:837–41. 45. Sebag J. Anomalous PVD – a unifying concept in vitreoretinal diseases. Graefes Arch Clin Exp Ophthalmol. 2004;242:690–8. 46. Sebag J, Buckingham B, Charles MA, Reiser K. Biochemical abnormalities in vitreous of humans with proliferative diabetic retinopathy. Arch Ophthalmol. 1992;110:1472–9. 47. Sebag J. Abnormalities of human vitreous structure in diabetes. Graefes Arch Clin Exp Ophthalmol. 1993;231:257–60. 48. Sebag J, Ansari RR, Dunker S, Suh SI. Dynamic light scattering of diabetic vitreopathy. Diabetes Technol Therapeut. 1999;1:169–76. 49. Sebag J. Seeing the invisible − the challenge of imaging vitreous. J Biomed Optics. 2004;9:38–46. 50. Lindner B. Acute posterior vitreous detachment and its retinal complications. Acta Ophthalmol. 1966;87 (Suppl):1–08. 51. Verbraeken H, Van Egmond J. Non-diabetic and non-oculotraumatic vitreous haemorrhage treated by pars plana vitrectomy. Bull Soc Belge Ophthalmol. 1999;272:83–9. 52. Sarrafizadeh R, Hassan TS, Ruby AJ, et al. Incidence of retinal detachment and visual outcome in eyes presenting with posterior vitreous separation and dense fundus-obscuring vitreous hemorrhage. Ophthalmology. 2001;108:2273–8. 53. Byer NE. Posterior vitreous detachment as a risk factor for retinal detachment. Ophthalmology. 1995;102:528. 54. Green RL, Byrne SF. Diagnostic ophthalmic ultrasound. In: Ryan SJ, ed. Retina, St Louis: CV Mosby; 1989. 55. Kakehashi A, Schepens CL, de Sousa-Neto A, et al. Biomicroscopic findings of posterior vitreoschisis. Ophthalmic Surg. 1993;24:846–50. 56. Chu T, Lopez PF, Cano MR, et al. Posterior vitreoschisis. An echographic finding in proliferative diabetic retinopathy. Ophthalmology. 1996;103:315–22. 57. Genovesi-Ebert F, Rizzo S, Chiellini S, et al. Reliability of standardized echography before vitreoretinal surgery for proliferative diabetic retinopathy. Ophthalmologica. 1998;2122(Suppl 1):91–2. 58. Badrinath SS, Gopal L, Sharma T, et al. Vitreoschisis in Eale’s disease – pathogenic role and significance in surgery. Retina. 1999;19:51–4. 59. Lundquist O, Osterlin S. Glucose concentration in the vitreous of nondiabetic and diabetic human eyes. Graefes Arch Clin Exp Ophthalmol. 1995;232:71–4. 60. Faulborn J, Bowald S. Microproliferations in proliferative diabetic retinopathy and their relation to the vitreous. Graefes Arch Clin Exp Ophthalmol. 1985;223:130–8. 61. Andrews JS, Lynn C, Scobey JW, Elliot JH. Cholesterolosis bulbi − case report with modern chemical identification of the ubiquitous crystals. Br J Ophthalmol. 1973;57:838–44. 62. Grossniklaus HE, Frank KE, Farbi DC, et al. Hemoglobin spherulosis in the vitreous cavity. Arch Ophthalmol. 1988;106:961–2. 63. Fawzi AA, Vo B, Kriwanek R, et al. Asteroid hyalosis in an autopsy population – the UCLA experience. Arch Ophthalmol. 2005;123:486–90. 67. Smith JL. Asteroid hyalites − incidence of diabetes mellitus and hypercholesterolemia. JAMA. 1958;168:891–3. 68. Bergren RC, Brown GC, Duker JS. Prevalence and association of asteroid hyalosis with systemic disease. Am J Ophthalmol. 1991;111:289–93. 69. Hatfield RE, Gastineau CF, Rucke CW. Asteroid bodies in the vitreous − relationship to diabetes and hypercholesterolemia. Mayo Clin Proc. 1962;37:513–4. 70. Sebag J, Albert DM, Craft JL. The Alström syndrome − ocular histopathology and retinal ultrastructure. Br J Ophthalmol. 1984;68:494–501. 71. Yu SY, Blumenthal HT. The calcification of elastic tissue. In: Wagner BM, Smith DE, eds. The connective tissue, Baltimore: Williams & Wilkins; 1967. 72. Lamba PA, Shukla KM. Experimental asteroid hyalopathy. Br J Ophthalmol. 1971;55:279–83. 73. Doft BH, Rubinow A, Cohen AS. Immunocytochemical demonstration of prealbumin in the vitreous in heredofamilial amyloidosis. Am J Ophthalmol. 1984;97:296–300. 6.46 Vitreous Anatomy and Pathology 64. Rodman HI, Johnson FB, Zimmerman LE. New histopathological and histochemical observations concerning asteroid hyalitis. Arch Ophthalmol. 1961;66: 552–63. 65. Wasano T, Hirokuwa H, Tagawa H, et al. Asteroid hyalosis − posterior vitreous detachment and diabetic retinopathy. Am J Ophthalmol. 1987;19:255–8. 66. Streeten BA. Disorders of the vitreous. In: Garner A, Klintworth GK, eds. Pathobiology of ocular disease − a dynamic approach, Part B, New York: Marcel Dekker; 1982:1381–419. 773