Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Electrocardiography wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Cardiovascular disease wikipedia , lookup
Heart failure wikipedia , lookup
Cardiac surgery wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Coronary artery disease wikipedia , lookup
Myocardial infarction wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
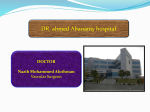
Ventricular Arterial Stiffening Integrating the Pathophysiology David A. Kass Downloaded from http://hyper.ahajournals.org/ by guest on June 17, 2017 Abstract—Vascular stiffening of the large arteries is a common feature of aging and is exacerbated by many common disorders such as hypertension, diabetes, and renal disease. This change influences the phasic mechanical stresses imposed on the blood vessels that in turn is important to regulating smooth muscle tone, endothelial function, and vascular health. In addition, the heart typically adapts to confront higher and later systolic loads by both hypertrophy and ventricular systolic stiffening. This creates altered coupling between heart and vessel that importantly affects cardiovascular reserve function. In this overview, I discuss the notion of a coupling disease in which stiffness of both heart and arteries interact to limit performance and generate clinical symptoms. This involves changes in the mechanical interaction of both systems, changes in signaling within the arteries themselves, and alterations in coronary flow regulation. Lastly, I briefly review recent development in de-stiffening strategies that may pave the way to treat this syndrome and its clinical manifestations. (Hypertension. 2005;46:185-193.) Key Words: arteries 䡲 compliance 䡲 ventricular function W idening of the arterial pulse is common in the elderly and is generally a reflection of arterial stiffening. It is a dominant circulatory hemodynamic risk factor for cardiac disease and stroke.1–3 Pulsatility of blood flow and pressure is also an intrinsic feature of the circulation. For example, during aerobic exercise, the arterial pulse can increase ⬎100% in peripheral arteries and by ⬇50% in central arteries (Figure 1A).4 Short-term widening of the pulse pressure under these circumstances might be considered physiological and not a source for vascular or ventricular disease. One might even anticipate increased pulsatile mechanical stimulation of the arteries to enhance endothelial regulation of vascular tone to improve blood flow where needed. As discussed later in this review, there is a growing body of data supporting such signaling and its role in enhancing organ perfusion. However, this may require normal vascular distensibility and thus may be compromised in stiff arteries. In contrast, chronic increases in pulse pressure (Figure 1A) caused by age-related arterial damage and/or diseases that stimulate vascular stiffening (eg, diabetes, renal disease) worsen cardiovascular risk. When considering the pathophysiologic implications of vascular stiffening, it is important not to overlook the role played by the heart to which the blood vessels are coupled. Evidence shows that ventricular systolic and diastolic stiffness also increase with age, which increase in tandem with large-artery stiffening.5,6 This is likely linked to the interaction of heart and vascular load, and also by intrinsic changes in the heart itself, and common comorbidities such as diabe- tes, hypertension, renal disease, and neurohumoral stress that impact both systems. Importantly, such combined stiffening alters how the heart–arterial system interacts at rest, but particularly under stress by exertional demands, salt loading, and abrupt changes in heart function. In this broad sense, combined ventricular–arterial stiffening potently impacts on cardiovascular reserve, blood pressure lability and diastolic dysfunction, coronary and peripheral flow regulation, endothelial function, and mechanical signaling, and undoubted other factors. It is in this broader context that I propose the concept of stiff heart artery coupling disease. These changes occur to some extent with aging5 and may be particularly prominent in patients with cardiac hypertrophy in whom heart failure symptoms develop despite having a preserved ejection fraction.6 In this review, I discuss the pathophysiology of coupling disease and suggest some novel approaches to treating it. Ventricular–Arterial Stiffening Age-dependent increases in vascular stiffening are well established with evidence from multiple large cross-sectional studies involving various ethnicities.7,8 Mechanisms underlying this stiffening, methodologies to assess it, and new approaches to treat it have all been subjects of recent reviews9 –11 and are not discussed here. What has been only more recently revealed is that age-related vascular stiffening is also accompanied by changes in the left ventricle (LV) that increase end-systolic chamber stiffness.5 This does not require renal disease and/or cardiac hypertrophy to be present,5 Received February 15, 2005; first decision February 23, 2005; revision accepted April 13, 2005. From the Division of Cardiology, Department of Medicine, Johns Hopkins Medical Institutions, Baltimore, Md. Correspondence to David A. Kass, MD, Ross 835, Johns Hopkins Medical Institutions, 720 Rutland Avenue, Baltimore, MD 21205. E-mail [email protected] © 2005 American Heart Association, Inc. Hypertension is available at http://www.hypertensionaha.org DOI: 10.1161/01.HYP.0000168053.34306.d4 185 186 Hypertension July 2005 Downloaded from http://hyper.ahajournals.org/ by guest on June 17, 2017 Figure 1. A, Physiological versus pathologic causes for higher artery pulse pressure. Upper panel, Radial and central arterial pressures increasing with aerobic exercise in a young subject. Lower panel, Arterial pulse pressure increases with vascular aging. B, Increased ventricular end-systolic stiffness (Ees) accompanies arterial stiffening with age. Pressure–volume loops from young and elderly individual show increases in Ees that match increases in arterial loading indexed by arterial elastance (Ea). C, Inverse correlation between total arterial compliance and ventricular end-systolic stiffness in humans. D, Increased load sensitivity of systolic pressure by ventricular–arterial stiffening in the elderly. From Chen et al5 and Kawaguchi et al.6 although both play important roles in vascular and ventricular stiffening.10 Importantly, this combination of ventricular–arterial stiffening alters the way in which the cardiovascular system can respond to stress demands and changes in volume and pressure loading. Furthermore, it appears common in patients with heart failure and preserved ejection fraction and may importantly contribute to the clinical features of this disorder.6 Figure 1B shows example pressure–volume (PV) relations measured invasively in a young and elderly individual, with neither having any demonstrable clinical heart disease at the time of study. Each set of loops was obtained by transient obstruction of venous return, with the baseline condition reflected by the most rightward loop of the set. The 2 relations depicted are the end-systolic PV relation and slope (Ees) and the ratio of end-systolic pressure to stroke volume— or effective arterial elastance (Ea). These are often equal in absolute magnitude, a combination yielding optimal and efficient matching of heart and artery. However, the elderly patient displays marked increases in both elastances, with Ea reflecting vascular stiffening and Ees LV systolic stiffening. The change in loop shape (trapezoidal) in the elderly subject reflects stiff arteries with a wider pulse pressure. The diastolic PV relation (lower boundary of the loops) is also somewhat steeper. As reported by Chen et al,5 Ea, Ees, and diastolic stiffness increase with age and correlate with one another. Figure 1C shows such an inverse relation between Ees and total arterial compliance, with the latter a component of Ea (Ea increases as compliance declines). Patients with low arterial compliance display increased Ees.6 Higher ventricular and arterial stiffness has important implications to blood pressure lability and loading sensitivity. This is shown by example in Figure 1D, with the data derived from the same set of PV loops shown in Figure 1B. Decreasing preload results in only a modest decline in systolic blood pressure in the younger individual but a much greater change in the older subject. As previously reported,5 the slope of such relations is determined by both arterial and ventricular stiffness and increases with age. Another implication of combined ventricular–arterial stiffening is that exertional capacity can be limited and this may play a role in patients with heart failure and normal-range ejection fraction. An example from the recent study of Kawaguchi et al6 is shown in Figure 2A. This patient has increased Ees and Ea at baseline, and on performance of sustained hand-grip exercise (solid loop) displayed a marked hypertensive response and elevated diastolic pressures. The steep basal Ees means that contractile reserve, normally reflected by further increases in Ees, is limited, whereas pressure-loading changes are amplified. Evidence that such pathophysiology likely contributes to exertional intolerance was reported by Hundley et al (Figure 2B).12 There is a direct relation between arterial distensibility (ie, compliance) and peak oxygen consumption during exercise testing. Patients with cardiac failure symptoms and preserved ejection fraction (EF) are shown by the white triangles and have the stiffest arteries. This study did not determine whether these patients also had increased Ees, although a more recent study found such elevations that exceeded that predicted from age alone in Kass Pathophysiology of Ventricular–Vascular Stiffening 187 Downloaded from http://hyper.ahajournals.org/ by guest on June 17, 2017 Figure 2. A, Effect of increased demand (handgrip exercise) on LV function depicted by pressure–volume loop in subject with ventricular–arterial stiffening and cardiac failure with preserved ejection fraction. From Kawaguchi et al.6 B, Positive correlation between arterial stiffness and metabolic exercise capacity. From Hundley et al.12 C, Loss of afterload-dependence of pressure relaxation in transgenic mice with activated PKA–phosphorylation sites on troponin I (PKA-TnI TG). NTG indicates nontransgenic control. From Takimoto et al.15 such patients.6 Gender differences in ventricular arterial stiffening may also impact exercise performance.13 Cardiac relaxation is delayed when hearts are exposed to elevated systolic pressure during ejection (ie, increased afterload), as occurs with vascular stiffening or enhanced systemic resistance.14 As noted in Figures 1 and 2A, ventricular– vascular stiffening exacerbates the load–pressure interaction, worsening the potential impact on diastole. A correlation between greater prolongation of diastolic relaxation and ventricular vascular (VV) stiffening was found in a recent study.6 Underlying mechanisms for load-dependence of relaxation have been previously unclear, although recent murine studies in which protein kinase A–phosphorylation sites on troponin I were constitutively active has yielded new insights.15 As shown in Figure 2C, normal mice show marked relaxation delay when cardiac afterload is increased by partial aortic constriction, whereas the mutant animals display little effect, highlighting a key role of TnI-PKA phosphorylation state as a coupler between load and relaxation. Impact of Blood Flow Pulsatility A major hemodynamic consequence of arterial stiffening is widening of the arterial pulse, which also increases cyclic changes of arterial flow. In studies performed over the past decade, we and other investigators have found that such pulsatility itself triggers vasodilator responses and contributes to flow reserve. In vitro studies suggest this may be blunted by loss of wall distension (ie, vascular stiffening), although this has not yet been tested in vivo. The initial observation that enhancing flow pulsatility itself triggers vasodilation in vivo came in an experiment testing effects of systemic vascular stiffening on cardiac function and mechanoenergetics.16,17 In canine hearts ejecting into a stiff conduit substituting for the thoracic aorta, total compliance was reduced and central arterial pulse pressure increased 2- to 3-fold. At matched cardiac oxygen consumption, hearts ejecting into this stiff load displayed ⬇15% increase in mean coronary blood flow.17 Subsequent studies using a servocontrolled perfusion pump to selectively vary pulse pressure 188 Hypertension July 2005 Downloaded from http://hyper.ahajournals.org/ by guest on June 17, 2017 Figure 3. A, Change in phasic coronary pressure and flow waveforms with increased pulse perfusion. B, Augmentation of coronary flow by pulse perfusion is enhanced by concomitant coronary vasodilation from adenosine. C, Role of NO and KCa-dependent signaling in pulse perfusion enhancement of mean coronary flow; raw tracings (upper) and summary results (lower). L-NMMA indicates NG-monomethyl-L-arginine. Monoacetate (NO synthase inhibitor) and CbTX (charybdotoxin) and AP (apamin) (KCa-inhibitors). From Paolocci et al.19 D, Effect of acute coronary occlusion on LV function in canine model with heart ejection directed into a stiff (wide pulse pressure) or compliant aorta. With the former, there is a marked decline in LV pressure and increase in chamber volumes (dilation) induced by the acute ischemia. This is minimal if the heart ejects into a compliant vasculature, despite identical sites of coronary occlusion. Modified from Saeki et al17 and Kass et al.24 in a given vascular bed18 –20 confirmed this and clarified the biochemical mechanisms. Figure 3A shows the effect of altering pulse pressure in a coronary artery and consequent changes in phasic flow. Diastolic flow increased slightly with the higher pulse pressure despite a decline in mean pressure during this period, and there was a greater increase in flow during the systolic period. Net flow increased ⬇15%, confirmed by both coronary sinus and microsphere flow, and is not associated with changes in regional function or metabolic demand. A 15% change in coronary flow from higher perfusion pulsatility, although significant, was not large, raising doubts that such a mechanism would play an important physiological role. However, the situation changed markedly when distal vascular tone is modestly lowered by adenosine involving activation of ATP-sensitive potassium channels20 (Figure 1B). Under such conditions, the same augmentation of pulse pressure results in a marked increase in mean flow, with a peak response nearly doubling flow over that at the normal (40 mm Hg) pulse pressure. This was specific to vasodilators that were active in the distal microvessels (ie, ⬍150 m) by mechanisms involving activation of KATP channels (adenosine, pinacidil). Alternative dilators operating on more prox- imal vessels (calcium channel blockers, acetylcholine, bradykinin) did not replicate this synergistic interaction with perfusion pulsatility.20 Endothelial-dependent vasodilation caused by elevated perfusion pulsatility has been confirmed in vascular beds other than the coronary arteries. For example, Nakano et al21 reported that augmenting pulse perfusion in skeletal muscle triggers primary nitric oxide (NO)-dependent vasodilation. More recently, studies using external muscle compression to enhance central coronary blood flow revealed enhanced endothelial-dependent flow dilation in upper arm vascular beds exposed to the resulting higher perfusion pulsatility.22 Steady shear stress induces vasodilation largely by activating NO synthase (NO release) and by stimulating factors that induce hyperpolarization.23 Although the precise mediators for the latter remain unclear and likely vary with the vascular tissue and site, they commonly stimulate calcium-dependent potassium channels (KCa) and can be inhibited by KCablocking toxins. Both NO and KCa signaling are involved with pulse perfusion-mediated dilation as shown by Paolocci et al19 (Figure 3C). Inhibiting either pathway alone reduced the pulse perfusion response by half, whereas when combined this response was virtually eliminated. Kass Pathophysiology of Ventricular–Vascular Stiffening 189 Downloaded from http://hyper.ahajournals.org/ by guest on June 17, 2017 Figure 4. A, Phasic pressure waveforms generated in vitro to stimulate vascular pulse perfusion in distensible or stiff vessels; left tracings are from compliant silastic tube, right tracings from stiff tube. B, Differential activation of the serine/threonine kinase Akt by pulse perfusion in compliant versus stiff tubes. C, Similar differential response in endothelial NO synthase phosphorylation in stiff vs compliant tubes. Although normally compliant arteries can dilate in response to pulse perfusion, in the coronary circulation, this is also coupled to changes in the phasic pattern of flow, as noted in Figure 3A, and this has potentially detrimental consequences on cardiac reserve. Normal coronary perfusion is principally diastolic, and reducing systolic pressure has less impact on mean flow. However, this may not hold in hearts ejecting into a stiff arterial system with consequent increases in flow during systole. This shift can render the heart more sensitive to a decline in systolic pressure as occurs with loading changes or acute dysfunction (eg, myocardial infarction). An example is shown in Figure 3D. On the right are data from an in vivo heart ejecting into a stiff (bypass) arterial system resulting in high arterial pulsatility. Acute coronary occlusion led to a rapid decline in LV pressure and marked chamber dilation (LV volume), ultimately triggering cardiac demise. After full resuscitation, the experiment was repeated but with the same heart now ejecting into the compliant vascular system. The magnitude of cardiac dysfunction was markedly attenuated (data from Kass et al24). Thus, high perfusion pulsatility can benefit vascular tone yet have detrimental effects on myocardial flow regulation. As discussed in the next section, the benefits may diminish in vessels that are not compliant, so that the net balance tips further toward pathophysiology in such settings. Role of Wall Distensibility Another feature of ventricular–arterial stiffening is that it changes the mechanical forces to which endothelial cells and arterial smooth muscle cells are exposed. Because these mechanical forces play key roles in regulating wall tone, atherogenesis, angiogenesis, and other features of vascular homeostasis, understanding their impact is important. Using perfusion systems that expose cultured endothelial cells to controlled levels of phasic flow with or without distension, studies have revealed effects of pulsatility on NO synthase gene expression,25–27 endothelin, and other signaling cascades28 that tend to favor a vasorelaxant response. 190 Hypertension July 2005 Arterial and Ventricular Destiffening Strategies Reduce smooth muscle tone Nitrates, ACE inhibitors, ARBs, calcium channel blockers Enhance endothelial function/relaxation Exercise Antioxidants Tetrahydrobiopterin Statins Rho kinase inhibitors Alter structural properties Reduce fibrosis (ARBs, aldosterone blockers, TGF-1 inhibitors) Limit or reverse hypertrophy Advanced glycation end-product cleavage Enhance elasticity (elastin, fibrillin, etc) ACE indicates angiotensin-converting enzyme; ARB, angiotensin receptor blocker; TGF, transforming growth factor. Downloaded from http://hyper.ahajournals.org/ by guest on June 17, 2017 Recent studies used more physiological waveforms (Figure 4A) and assessed post-translational changes in signaling proteins.29 Endothelial cells cultured on the inner surface of distensible tubes were exposed to pulse perfusion with the degree of wall distensibility varied. These studies found important differences in signaling related to distensibility (Figure 4B and 4C). The enzyme Akt is stimulated in response to mechanical shear stress30 and cyclic stretch,31 and by receptor-coupled growth factors (eg, IGF-1).32 Activated Akt phosphorylates NO synthase to enhance NO release30 and stimulates proteins controlling vasculogenesis, endothelial cytoprotection, and apoptosis.32 When cyclic stretch and shear were combined in normally compliant tubes, Akt was activated much more than with steady shear alone (Figure 3B).33 This was lacking if wall compliance was reduced, however. Downstream targets of Akt such as NO synthase also displayed this differential activation. (Figure 3C). This is further supported by data showing enhanced NO release from endothelial cells grown in distensible tubes exposed to pulsatile flow from external compression.34 Destiffening Strategies Past and evolving strategies to counter vascular stiffening have been recently reviewed35 and are summarized in the Table. To date, the major emphasis has been on inhibitor smooth muscle tone, working through the NO/cGMP pathway, or by blocking neurohormones such as angiotensinconverting enzyme and angiotensin II. Calcium channel blockers have also been used. For example, verapamil has been shown to acutely lower ventricular systolic stiffness and arterial stiffness and, in association with these changes, improve aerobic exercise capacity in aged volunteers.36 This exercise benefit was not reproduced when smooth muscle tone only was reduced using an intravenous nitrate.37 Ongoing studies using angiotensin II receptor-blocking agents in patients with heart failure and normal-range EF may help clarify the role of such drugs for this disorder. Previous data from the substudy CHARM (Preserved) trial found only slight clinical benefits38 but the study population was not really representative. Exercise remains an important factor and has been shown to reduce vascular stiffening with aging.39 Whether it can also lower ventricular systolic stiffening remains unknown. There is increasing interest in the use of 3-hydroxy-3-methylglutaryl– coenzyme A reductase inhibitors (statins). Studies have shown that statins augment Akt activity in vessels,40 improve blood flow by increasing NO synthase activation,41 and may reduce vascular stiffening.42 Statins also inhibit small GTPbinding proteins Rac1 and RhoA and thereby may impede development of cardiac hypertrophy.43– 45 Other strategies may involve enhancing NO synthase signaling by increasing substrate availability (arginase inhibition) or its cofactor tetrahydrobiopeterin (BH4).46 Another tactic gaining interest is to reduce fibrosis and/or modify structural proteins thought linked to stiffness. Drugs that inhibit angiotensin II and particularly aldosterone47,48 are intriguing in this regard. Both may have the added advantages to targeting both vascular and ventricular changes. Efforts to enhance elastin by blocking neutrophil elastace have yielded very exciting results in both the heart and vasculature.49 However, translation to human trials has remained limited by the toxicity of these drugs, and this avenue remains one undergoing investigation. A different strategy that may also target both heart and arteries relates to the cleavage of advanced glycation endproducts (AGEs). AGEs are highly stable glucose—protein links that accumulate with normal aging but are enhanced in settings of glucose excess (diabetes) and/or molecular stress such as from oxidation.50,51 These cross links form in collagen and other long-lived structural molecules resulting in reduced turnover by metalloproteinases and likely increased tissue stiffness. Proof for the involvement of AGEs in structural stiffness remains fairly indirect but has been fueled by animal and a recent clinical trial found that a breaker of AGE (ALT-711) improves vascular distensibility,52,53 and perhaps ventricular diastolic distensibility (Figure 5A).54 Last, we recently reported that enhancement of protein kinase G activation by inhibiting PDE5a may provide a novel approach to ventricular–arterial stiffening.55 PDE5a is the enzymatic target of sildenafil, which is widely used to treat erectile dysfunction. In the vasculature, PDE5a inhibition increases cGMP to activate protein kinase G-I, leading to reduced vascular tone. PDE5a inhibitors also appear to lower vascular stiffness,56 although the extent to which this is independent of mean pressure remains somewhat unclear. cGMP plays an important role as a negative modulator of vascular proliferation and fibrosis. Similarly, increasing cGMP/PKG activation in the heart reduces fibrosis and can be anti-hypertrophic.57,58 In mice, PDE5a inhibition markedly inhibits the development of cardiac hypertrophy and fibrosis while improving ventricular function despite sustained ventricular afterload increase59 (Figure 5B). Furthermore, this treatment reversed hypertrophy and fibrosis once established (Figure 5C). It remains to be determined whether this strategy will prove efficacious for treating humans with ventricularvascular stiffening (coupling disease). Perspectives This brief review is meant to place recent studies regarding pulsatile perfusion, arterial, and ventricular stiffening in Kass Pathophysiology of Ventricular–Vascular Stiffening 191 Downloaded from http://hyper.ahajournals.org/ by guest on June 17, 2017 Figure 5. Novel de-stiffening strategies. A, Effect of advanced glycation endproduct cross-link breaker (ALT-711) on human arterial total compliance as a function of changes in mean arterial pressure over a 2-month treatment period. From Kass et al.52 B, Inhibition of pressure load-induced cardiac hypertrophy (traverse aortic constriction [TAC]) in mice treated with the PDE5a inhibitor sildenafil (left). Right panel shows capacity of sildenafil to reverse pre-established ventricular hypertrophy (also triggered by pressure load) over subsequent 2 weeks. From Takimoto et al.55 perspective. Although many previous reviews have focused on stiffening of the arteries themselves, and much of this special issue highlights this pathophysiology, such changes have major ramifications on the heart and the manner in which it interacts with the rest of the body. Cardiac maladaptations such as hypertrophy and increased ventricular end-systolic elastance make the net effects of vascular stiffening even worse, particularly from the standpoint of net cardiovascular reserve, blood pressure regulation, and blood volume distribution. It is in the context of the coupling between these altered systems that one best understands the physiological manifestations observed in many affected patients. New de-stiffening strategies are needed, and some are presently undergoing development and entering clinical trials. Greater appreciation of the impact of coupling disease in the elderly should help us apply even the known therapies with better focus and hopefully improve our approach to this disorder. Acknowledgments Supported by National Institutes of Health grants HL-47511 and AG-18324. References 1. Asmar R, Rudnichi A, Blacher J, London GM, and Safar M. Pulse pressure and aortic pulse wave are markers of cardiovascular risk in hypertensive populations. Am J Hypertens. 2001;14:91–97. 2. Miura K, Dyer AR, Greenland P, Daviglus ML, Hill M, Liu K, Garside DB, Stamler J. Pulse pressure compared with other blood pressure indexes in the prediction of 25-year cardiovascular and all-cause mortality rates: The Chicago Heart Association Detection Project in Industry Study. Hypertension. 2001;38:232–237. 3. Haider AW, Larson MG, Franklin SS, Levy D. Systolic blood pressure, diastolic blood pressure, and pulse pressure as predictors of risk for congestive heart failure in the Framingham Heart Study. Ann Intern Med. 2003;138:10 –16. 4. Rowell LB, Brengelmann GB, Blackmon JR, Bruce RA, Murray JA. Disparities between aortic and peripheral pulse pressure induced by upright exercise and vasomotor changes in man. Circulation. 1968;37: 954 –964. 5. Chen C-H, Nakayama M, Nevo E, Fetics BJ, Maughan WL, Kass DA. Coupled systolic-ventricular and vascular stiffening with age implications for pressure regulation and cardiac reserve in the elderly. J Am Coll Cardiol. 1998;32:1221–1227. 6. Kawaguchi M, Hay I, Fetics B, Kass DA. Combined ventricular systolic and arterial stiffening in patients with heart failure and preserved ejection fraction: implications for systolic and diastolic reserve limitations. Circulation. 2003;107:714 –720. 7. Avolio AP, Deng FQ, Li WQ, Luo YF, Huang ZD, Xing LF, O’Rourke MF. Effects of aging on arterial distensibility in populations with high and 192 8. 9. 10. 11. 12. 13. 14. Downloaded from http://hyper.ahajournals.org/ by guest on June 17, 2017 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. Hypertension July 2005 low prevalence of hypertension: comparison between urban and rural communities in China. Circulation. 1985;71:202–210. Safar ME. Pulse pressure, arterial stiffness, and cardiovascular risk. Curr Opin Cardiol. 2000;15:258 –263. Mitchell GF. Arterial stiffness and wave reflection in hypertension: pathophysiologic and therapeutic implications. Curr Hypertens Rep. 2004;6:436 – 441. Safar ME, Levy BI, Struijker-Boudier H. Current perspectives on arterial stiffness and pulse pressure in hypertension and cardiovascular diseases. Circulation. 2003;107:2864 –2869. Oliver JJ, Webb DJ. Noninvasive assessment of arterial stiffness and risk of atherosclerotic events. Arterioscler Thromb Vasc Biol. 2003;23: 554 –566. Hundley WG, Kitzman DW, Morgan TM, Hamilton CA, Darty SN, Stewart KP, Herrington DM, Link KM, Little WC. Cardiac cycledependent changes in aortic area and distensibility are reduced in older patients with isolated diastolic heart failure and correlate with exercise intolerance. J Am Coll Cardiol. 2001;38:796 – 802. Najjar SS, Schulman SP, Gerstenblith G, Fleg JL, Kass DA, O’Connor F, Becker LC, Lakatta EG. Age and gender affect ventricular-vascular coupling during aerobic exercise. J Am Coll Cardiol. 2004;44:611– 617. Leite-Moreira AF, Correia-Pinto J, Gillebert TC. Afterload induced changes in myocardial relaxation: a mechanism for diastolic dysfunction. Cardiovasc Res. 1999;43:344 –353. Takimoto E, Soergel DG, Janssen PM, Stull LB, Kass DA, Murphy AM. Frequency- and afterload-dependent cardiac modulation in vivo by troponin I with constitutively active protein kinase A phosphorylation sites. Circ Res. 2004. Kelly RP, Tunin R, Kass DA. Effect of reduced aortic compliance on cardiac efficiency and contractile function of in situ canine left ventricle. Circ Res. 1992;71:490 –502. Saeki A, Recchia F, Kass DA. Systolic flow augmentation in hearts ejecting into a model of stiff aging vasculature. Influence on myocardial perfusion-demand balance. Circ Res. 1995;76:132–141. Recchia FA, Senzaki H, Saeki A, Byrne BJ, Kass DA. Pulse pressurerelated changes in coronary flow in vivo are modulated by nitric oxide and adenosine. Circ Res. 1996;79:849 – 856. Paolocci N, Pagliaro P, Isoda T, Saavedra FW, Kass DA. Role of calcium-sensitive K(⫹) channels and nitric oxide in in vivo coronary vasodilation from enhanced perfusion pulsatility. Circulation. 2001;103: 119 –124. Pagliaro P, Senzaki H, Paolocci N, Isoda T, Sunagawa G, Recchia FA, Kass DA. Specificity of synergistic coronary flow enhancement by adenosine and pulsatile perfusion in the dog. J Physiol (Lond). 1999;520(Pt 1):271– 80:271–280. Nakano T, Tominaga R, Nagano I, Okabe H, Yasui H. Pulsatile flow enhances endothelium-derived nitric oxide release in the peripheral vasculature. Am J Physiol Heart Circ Physiol. 2000;278:H1098 –H1104. Shechter M, Matetzky S, Feinberg MS, Chouraqui P, Rotstein Z, Hod H. External counterpulsation therapy improves endothelial function in patients with refractory angina pectoris. J Am Coll Cardiol. 2003;42: 2090 –2095. Busse R, Edwards G, Feletou M, Fleming I, Vanhoutte PM, Weston AH. EDHF: bringing the concepts together. Trends Pharmacol Sci. 2002;23: 374 –380. Kass DA, Saeki A, Tunin RS, Recchia FA. Adverse influence of systemic vascular stiffening on cardiac dysfunction and adaptation to acute coronary occlusion. Circulation. 1996;93:1533–1541. Hendrickson RJ, Cappadona C, Yankah EN, Sitzmann JV, Cahill PA, Redmond EM. Sustained pulsatile flow regulates endothelial nitric oxide synthase and cyclooxygenase expression in co-cultured vascular endothelial and smooth muscle cells. J Mol Cell Cardiol. 1999;31:619 – 629. Ziegler T, Silacci P, Harrison VJ, Hayoz D. Nitric oxide synthase expression in endothelial cells exposed to mechanical forces. Hypertension. 1998;32:351–355. Qiu Y, Tarbell JM. Interaction between wall shear stress and circumferential strain affects endothelial cell biochemical production. J Vasc Res. 2000;37:147–157. Lehoux S, Esposito B, Merval R, Tedgui A. Differential regulation of vascular focal adhesion kinase by steady stretch and pulsatility. Circulation. 2005;111:643– 649. Peng X, Recchia FA, Byrne BJ, Wittstein IS, Ziegelstein RC, Kass DA. In vitro system to study realistic pulsatile flow and stretch signaling in cultured vascular cells. Am J Physiol Cell Physiol. 2000;279:C797–C805. 30. Dimmeler S, Fleming I, Fisslthaler B, Hermann C, Busse R, Zeiher AM. Activation of nitric oxide synthase in endothelial cells by Akt-dependent phosphorylation. Nature. 1999;399:601– 605. 31. Chen AH, Gortler DS, Kilaru S, Araim O, Frangos SG, Sumpio BE. Cyclic strain activates the pro-survival Akt protein kinase in bovine aortic smooth muscle cells. Surgery. 2001;130:378 –381. 32. Shiojima I, Walsh K. Role of Akt signaling in vascular homeostasis and angiogenesis. Circ Res. 2002;90:1243–1250. 33. Peng X, Haldar S, Deshpande S, Irani K, Kass DA. Wall stiffness suppresses Akt/eNOS and cytoprotection in pulse-perfused endothelium. Hypertension. 2003;41:378 –381. 34. Dai G, Tsukurov O, Chen M, Gertler JP, Kamm RD. Endothelial nitric oxide production during in vitro simulation of external limb compression. Am J Physiol Heart Circ Physiol. 2002;282:H2066 –H2075. 35. Zieman S, Melanovsky V, Kass DA. Mechanisms, pathophysiology and therapy of arterial stiffness. Arterioscler Thromb Vasc Biol. 2005. 25:932–934. 36. Chen CH, Nakayama M, Talbot M, Nevo E, Fetics B, Gerstenblith G, Becker LC, Kass DA. Verapamil acutely reduces ventricular-vascular stiffening and improves aerobic exercise performance in elderly individuals. J Am Coll Cardiol. 1999;33:1602–1609. 37. Nussbacher A, Gerstenblith G, O’Connor FC, Becker LC, Kass DA, Schulman SP, Fleg JL, Lakatta EG. Hemodynamic effects of unloading the old heart. Am J Physiol. 1999;277:H1863–H1871. 38. Yusuf S, Pfeffer MA, Swedberg K, Granger CB, Held P, McMurray JJ, Michelson EL, Olofsson B, Ostergren J. Effects of candesartan in patients with chronic heart failure and preserved left-ventricular ejection fraction: the CHARM-Preserved Trial. Lancet. 2003;362:777–781. 39. Tanaka H, Dinenno FA, Monahan KD, Clevenger CM, DeSouza CA, Seals DR. Aging, habitual exercise, and dynamic arterial compliance. Circulation. 2000;102:1270 –1275. 40. Kureishi Y, Luo Z, Shiojima I, Bialik A, Fulton D, Lefer DJ, Sessa WC, Walsh K. The HMG-CoA reductase inhibitor simvastatin activates the protein kinase Akt and promotes angiogenesis in normocholesterolemic animals. Nat Med. 2000;6:1004 –1010. 41. Mital S, Zhang X, Zhao G, Bernstein RD, Smith CJ, Fulton DL, Sessa WC, Liao JK, Hintze TH. Simvastatin upregulates coronary vascular endothelial nitric oxide production in conscious dogs. Am J Physiol Heart Circ Physiol. 2000;279:H2649 –H2657. 42. Ferrier KE, Muhlmann MH, Baguet JP, Cameron JD, Jennings GL, Dart AM, Kingwell BA. Intensive cholesterol reduction lowers blood pressure and large artery stiffness in isolated systolic hypertension. J Am Coll Cardiol. 2002;39:1020 –1025. 43. Laufs U, Kilter H, Konkol C, Wassmann S, Bohm M, Nickenig G. Impact of HMG CoA reductase inhibition on small GTPases in the heart. Cardiovasc Res. 2002;53:911–920. 44. Takemoto M, Node K, Nakagami H, Liao Y, Grimm M, Takemoto Y, Kitakaze M, Liao JK. Statins as antioxidant therapy for preventing cardiac myocyte hypertrophy. J Clin Invest. 2001;108:1429 –1437. 45. Patel R, Nagueh SF, Tsybouleva N, Abdellatif M, Lutucuta S, Kopelen HA, Quinones MA, Zoghbi WA, Entman ML, Roberts R, Marian AJ. Simvastatin induces regression of cardiac hypertrophy and fibrosis and improves cardiac function in a transgenic rabbit model of human hypertrophic cardiomyopathy. Circulation. 2001;104:317–324. 46. Alp NJ, Channon KM. Regulation of endothelial nitric oxide synthase by tetrahydrobiopterin in vascular disease. Arterioscler Thromb Vasc Biol. 2004;24:413– 420. 47. White WB, Duprez D, St Hillaire R, Krause S, Roniker B, Kuse-Hamilton J, Weber MA. Effects of the selective aldosterone blocker eplerenone versus the calcium antagonist amlodipine in systolic hypertension. Hypertension. 2003;41:1021–1026. 48. Lacolley P, Labat C, Pujol A, Delcayre C, Benetos A, Safar M. Increased carotid wall elastic modulus and fibronectin in aldosterone-salt-treated rats: effects of eplerenone. Circulation. 2002;106:2848 –2853. 49. Ohta K, Nakajima T, Cheah AY, Zaidi SH, Kaviani N, Dawood F, You XM, Liu P, Husain M, Rabinovitch M. Elafin-overexpressing mice have improved cardiac function after myocardial infarction. Am J Physiol Heart Circ Physiol. 2004;287:H286 –H292. 50. Zieman SJ, Kass DA. Advanced glycation endproduct crosslinking in the cardiovascular system: potential therapeutic target for cardiovascular disease. Drugs. 2004;64:459 – 470. 51. Yan SF, Ramasamy R, Naka Y, Schmidt AM. Glycation, inflammation, and RAGE: a scaffold for the macrovascular complications of diabetes and beyond. Circ Res. 2003;93:1159 –1169. Kass Pathophysiology of Ventricular–Vascular Stiffening 52. Kass DA, Shapiro EP, Kawaguchi M, Capriotti AR, Scuteri A, deGroof RC, Lakatta EG. Improved arterial compliance by a novel advanced glycation end-product crosslink breaker. Circulation. 2001;104: 1464 –1470. 53. Vaitkevicius PV, Lane M, Spurgeon H, Ingram DK, Roth GS, Egan JJ, Vasan S, Wagle DR, Ulrich P, Brines M, Wuerth JP, Cerami A, Lakatta EG. A cross-link breaker has sustained effects on arterial and ventricular properties in older rhesus monkeys. Proc Natl Acad Sci U S A. 2001;98: 1171–1175. 54. Asif M, Egan J, Vasan S, Jyothirmayi GN, Masurekar MR, Lopez S, Williams C, Torres RL, Wagle D, Ulrich P, Cerami A, Brines M, Regan TJ. An advanced glycation endproduct cross-link breaker can reverse age-related increases in myocardial stiffness. Proc Natl Acad Sci U S A. 2000;97:2809 –2813. 55. Takimoto E, Champion HC, Li M, Belardi D, Ren S, Rodriguez ER, Bedja D, Gabrielson KL, Wang Y, Kass DA. Chronic inhibition of cyclic 56. 57. 58. 59. 193 GMP phosphodiesterase 5A prevents and reverses cardiac hypertrophy. Nat Med. 2005;11:214 –222. Vlachopoulos C, Hirata K, O’Rourke MF. Effect of sildenafil on arterial stiffness and wave reflection. Vasc Med. 2003;8:243–248. Holtwick R, van Eickels M, Skryabin BV, Baba HA, Bubikat A, Begrow F, Schneider MD, Garbers DL, Kuhn M. Pressure-independent cardiac hypertrophy in mice with cardiomyocyte-restricted inactivation of the atrial natriuretic peptide receptor guanylyl cyclase-A. J Clin Invest. 2003; 111:1399 –1407. Pilz RB, Casteel DE. Regulation of gene expression by cyclic GMP. Circ Res. 2003;93:1034 –1046. Takimoto E, Champion HC, Belardi D, Moslehi J, Mongillo M, Mergia E, Montrose DC, Isoda T, Aufiero K, Zaccolo M, Dostmann WR, Smith CJ, Kass DA. cGMP catabolism by phosphodiesterase 5A regulates cardiac adrenergic stimulation by NOS3-dependent mechanism. Circ Res. 2005;96:100 –109. Downloaded from http://hyper.ahajournals.org/ by guest on June 17, 2017 Ventricular Arterial Stiffening: Integrating the Pathophysiology David A. Kass Downloaded from http://hyper.ahajournals.org/ by guest on June 17, 2017 Hypertension. 2005;46:185-193; originally published online May 23, 2005; doi: 10.1161/01.HYP.0000168053.34306.d4 Hypertension is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2005 American Heart Association, Inc. All rights reserved. Print ISSN: 0194-911X. Online ISSN: 1524-4563 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://hyper.ahajournals.org/content/46/1/185 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Hypertension can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Hypertension is online at: http://hyper.ahajournals.org//subscriptions/