Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Herpes simplex wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Antibiotics wikipedia , lookup
Marburg virus disease wikipedia , lookup
Cryptosporidiosis wikipedia , lookup
Tuberculosis wikipedia , lookup
Carbapenem-resistant enterobacteriaceae wikipedia , lookup
Onchocerciasis wikipedia , lookup
Sarcocystis wikipedia , lookup
Gastroenteritis wikipedia , lookup
Anaerobic infection wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Clostridium difficile infection wikipedia , lookup
Visceral leishmaniasis wikipedia , lookup
Trichinosis wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Hepatitis C wikipedia , lookup
Leptospirosis wikipedia , lookup
Hepatitis B wikipedia , lookup
Dirofilaria immitis wikipedia , lookup
Oesophagostomum wikipedia , lookup
Schistosomiasis wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Neisseria meningitidis wikipedia , lookup
Candidiasis wikipedia , lookup
Neonatal infection wikipedia , lookup
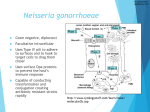
1 Name Teachers Name Class Date Gonorrhea This is a disease caused by Neisseria gonorrhoeae, a bacterium that can grow and multiply easily in mucus membranes of the body especially reproductive tract, including the cervix , uterus , and fallopian tubes in women, and in the urethra in women and men. The bacteria can also grow in the mouth, throat, and anus. Morphology Under oil immersion, they are intracellular Gram-negative kidney-shaped diplococci in polymorphonuclear leukocytes, the presence of which is required for the presumptive diagnosis of gonorrhea. The presence of extracellular Gram-negative diplococci is an equivocal finding that must be confirmed by culture or nucleic acid test. The endocervical smears from females or rectal specimens are more difficult to interpret due to the presence of other Gram-negative coccobacilli, including Moraxella osloensis, Moraxella phenylpyruvica, Kingella denitrificans and Acinetobacter species (Nancy, seifert, koomey,580) Gram stain Gram-negative diplococcic Pigmentation 2 N. gonorrhoeae colonies are pinkish-brown in color. Clear, golden-brown pigmentation apparent after incubation for 48 h. cultures results from autolysis of the cells (Nancy, seifert, koomey,578) Oxidase Test Oxidase test positive Acid Production Acid only from glucose Enzyme Substrate Test Hydroxyprolylaminopeptidase positive Nitrate Reduction Test Nitrate negative Polysaccharide from Sucrose Strains of some organisms do not grow on medium on which polysaccharide is detected, polysaccharide may be found in the growth inoculated onto the plate (Nancy, seifert, koomey, 583) N. gonorrhoeae does not produce polysaccharide from sucrose. Production of Deoxyribonuclease (DNase) DNase negative Superoxol Test Reaction with 30% hydrogen peroxide Superoxol positive; all strains give positive reaction 3 Catalase Test Reacts with 3% hydrogen peroxide The Disease Gonorrhea disease transmitted through sexual contact with an infected person. Gonorrhea may also be spread by contact with infected bodily fluids, so that a mother could transmit the infection to her newborn during birth. The most usual site of Neisseria gonorrhea infection is the urogenital tract. Men with this infection may also experience dysuria with penile discharge, and women might also have slight vaginal mucopurulent discharge, extreme pelvic pain, or no symptoms. A different N. gonorrhea infection occurs around anorectal, conjunctival, pharyngeal, and ovarian/uterine. Infections that arise inside the neonatal length may also cause ophthalmic neonatorum. If left untreated, N. gonorrhea infections can disseminate to other regions of the body, which generally reasons synovium and pores and skin infections(Susan,850). Disseminated gonococcal contamination presents as a few pores and skin lesions which can be restricted to the extremities. Those legions start as papules and progress into bullae, petechia, and necrotic lesions. Gonorrhea Symptoms in women Lower abdominal pain, burning urine, red itchy eyes, Bleeding between periods, Spotting during intercourse, vulvitis and Burning throat. In some women, symptoms mild and go unnoticed. 4 Many women with gonorrhea discharge think they have a yeast infection and self-treat with over-thecounter yeast infection drug (Douglas S, 1275) Gonorrhea symptoms in men Greenish yellow discharge from penis, burning urine, burning throat, swollen testicles, and swollen glands in the throat. Treatment Treatment is always (1) outpatient for genital infection; however, (2) admission may be necessary for complicated disseminated gonococcal infection (DGI) or gonococcal arthritis. In females, the risk of complications is much higher. In light of high rates of noncompliance, reinfection, and poor follow-up, clinicians advocate admitting a female patient whenever a question of a complication of pelvic inflammatory disease (PID) is present. Institutions have attempted to quantify abnormalities found on pelvic examination in an attempt to admit those patients with a higher likelihood of complications (Susan, 852) Cases with future fertility at risk, physicians are fairly aggressive, especially in situations in which the patient is young and unfamiliar to them. Physicians admit patients with corneal involvement for treatment with IV antibiotics. Drugs Ceftriaxone 250 mg intramuscular (IM) single dose and Azithromycin 1 g PO single dose Because of multidrug-resistant gonorrhea, treatment recommendations are as follows Treat gonorrhea with a single intramuscular injection of 250 mg ceftriaxone plus azithromycin 1 g PO as a single dose 5 If ceftriaxone is unavailable, patients be given a single oral dose of cefixime 400 mg and a single dose of azithromycin 1 g PO Ceftriaxone mode of action Ceftriaxone inhibits the mucopeptide synthesis in the bacterial cell wall. The beta-lactam part of Ceftriaxone binds to carboxypeptidases, endopeptidases, and transpeptidases in the bacterial cytoplasmic membrane. (Susan,852) The above enzymes are involved in cell-wall synthesis and cell division. By binding to these enzymes, Ceftriaxone results in the formation of defective cell walls and cell death. Azithromycin mode of action Azithromycin a macrolide antibiotic inhibits bacterial protein synthesis, quorum-sensing and reduces the formation of biofilm. Accumulating effectively in cells, particularly phagocytes, it is delivered in high concentrations to the site of infection, as reflected in rapid plasma clearance and extensive tissue distribution. Prevention as a form of long term treatment abstaining from sexual intercourse using condom every time you have vaginal, oral, or anal sexual intercourse having only one sexual partner who is uninfected and who is also sexually monogamous Since gonorrhea doesn’t cause symptoms, it’s good to get tested regularly. Consult your doctor about frequency of testing gonorrhea and other STIs. Avoid having sexual intercourse for at least seven days after completion of treatment. 6 Treatment side effects Side effects of certain medications are another concern regarding antibiotic therapy. All the recommended antibiotic medications can cause changes in the bacteria that normally inhabit the bowel or vagina (Michael A, 642) this makes women more susceptible to diarrhea or vaginal yeast infections because the bacteria treatment kills the normal flora. Gastrointestinal discomfort is another common side effect of antibiotics. Others include; Ceftriaxone and cefixime can trigger allergic reactions. May cause kidney damage. Ciprofloxacin and ofloxacin, have been linked to problems in the nervous system like headaches, dizziness, and convulsions. For me I would prefer the short term treatment since the infection is somehow shameful but I would back on doctor’s advice. 7 Work cited Freitag, Nancy E., H. Steven Seifert, and Michael Koomey. "Characterization of the pilF—pilD pilus‐assembly locus of Neisseria gonorrhoeae." Molecular microbiology 16.3 (1995): 575-586. Wang, Susan A., et al. "Multidrug-resistant Neisseria gonorrhoeae with decreased susceptibility to cefixime—Hawaii, 2001." Clinical Infectious Diseases 37.6 (2003): 849-852. Kellogg, Douglas S., et al. "Neisseria gonorrhoeae I. Virulence genetically linked to clonal variation." Journal of Bacteriology 85.6 (1963): 1274-1279. Apicella, Michael A., et al. "The pathogenesis of gonococcal urethritis in men: confocal and immunoelectron microscopic analysis of urethral exudates from men infected with Neisseria gonorrhoeae." Journal of Infectious Diseases 173.3 (1996): 636-646. 8