Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
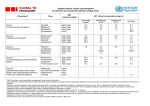
New Medicines Committee Briefing May 2013 Levofloxacin 0.5% (Oftaquix®) eye drops Levofloxacin (Oftaquix®) is to be reviewed for use within: Primary Care Secondary Care Summary: Oftaquix® is indicated for the topical treatment of bacterial external ocular infections. Oftaquix® is a broad spectrum antibacterial agent of the fluoroquinolone class. Oftaquix® is the L-isomer of the racemic drug substance ofloxacin with the antibacterial activity residing primarily in the L-isomer. Oftaquix® is a black triangle drug ( ) and is monitored intensively by the CHM and MHRA. Oftaquix® has a high corneal penetration compared to ofloxacin and ciprofloxacin 1 Formulary application Consultant submitting application: Ms Anupama Pherwani (Consultant Ophthalmologist) Clinical Director supporting application: Gareth Rowland (Clinical Director) Ms Pherwani has requested that Oftaquix® be considered for inclusion in the North Staffordshire Joint Formulary for the treatment of infectious keratitis (infective corneal ulcers). Currently, this is being treated with ofloxacin 0.3% or combination of gentamicin 1.5% and cefuroxime 5% (unlicensed). Ms Pherwani states that levofloxacin achieves higher concentration in tear film and anterior chamber and can be used in patients more than 1 year old. She also noted that it is a broad spectrum antibiotics and more effective against key ocular pathogens – strep. pneumoniae and P. aeruginosa. Levofloxacin have a low cytotoxicity compared to other antibiotics, with neutral pH, it is well tolerated compared to ciprofloxacin. Ms Pherwani did note the cost as a disadvantage to the proposed addition although cheaper to the current combination of gentamicin and cefuroximine. Background1,2,3,4,5,6,7 Keratitis or corneal inflammation is a potentially sight threatening condition which may have infectious or non-infectious aetiology. Bacterial keratitis is a sight-threatening process that can lead to severe visual loss. A particular feature of bacterial keratitis is its rapid progression; corneal destruction may be complete in 24-48 hours with some of the more virulent bacteria. Corneal ulceration, stromal abscess formation, surrounding corneal oedema, and anterior segment inflammation are characteristic of this disease. Interruption of an intact corneal epithelium and/or abnormal tear film permits entrance of microorganisms into the corneal stroma, where they may proliferate and cause ulceration. Virulence factors may initiate microbial invasion, or secondary effector molecules may assist the infective process. Risk factors for bacterial corneal infection include contact lens wear, ocular surface disease, corneal trauma and previous ocular or eyelid surgery. Certain ocular diseases and systemic conditions which depress the immune system also increase the possibility of bacterial keratitis. Early diagnosis and treatment are vital to minimizing any visual-threatening progression. In addition, close follow-up, attention to laboratory data, and changing antimicrobials if no clinical improvement is evident are important elements for successful outcome. 2 Treatment for corneal ulcers and infections depends on the cause. Treatment should be started as soon as possible to prevent scarring of the cornea. Topical antibiotics constitute the mainstay of treatment in cases of bacterial keratitis whereas the use of topical corticosteroids remains controversial. If the exact cause is not known, patients may be given antibiotic drops that work against many kinds of bacteria. The most common groups of bacteria responsible for bacterial keratitis are as follows: Streptococcus, Pseudomonas, Enterobacteriaceae (including Klebsiella, Enterobacter, Serratia, and Proteus), and Staphylococcus species. Once the exact cause is known, drops that treat bacteria, herpes, other viruses, or a fungus are prescribed. Severe ulcers sometimes require a corneal transplant. Most acute superficial eye infections can be treated topically. Bacterial eye infections are generally treated topically with eye drops and ointments. The treatment regimen for bacterial keratitis usually includes the administration of topical broad-spectrum antibiotics at short intervals to achieve local concentrations greater than the minimum inhibitory concentration for most bacteria. A common clinical practice associate cephalosporin active against some grampositive organisms frequently associated with bacterial keratitis with an aminoglycoside (gentamicin) active against large spectrum of gram-negative organisms. These antibiotics are used in highly concentrated solutions generally referred to as “fortified antibiotics”, to achieve high concentrations. Fluoroquinolones offer an alternative to fortified antibiotics. Ofloxacin, ciprofloxacin, levofloxacin, gatifloxacin and moxifloxacin offer the theoretical advantage of a good ocular penetration and of a broad-spectrum activity against both gram-positive and gramnegative pathogens at non-fortified concentrations. Levofloxacin is a later-generation antibacterial agent of the fluoroquinolone class. It was launched in several European countries in 2002. The main indications for treatment are bacterial blepharitis and conjunctivitis, bacterial keratitis – especially when associated with contact lenses – and endophthalmitis, where it is provided as an additional therapeutic agent. It is also used as prophylaxis to reduce the bacterial conjunctival flora prior to intraocular surgery. Levofloxacin is the L- isomer of the racemic drug ofloxacin with a broad spectrum antimicrobial activity. It has similar physicochemical, pharmacological and toxicological properties to other marketed fluoroquinolones such as ofloxacin, ciprofloxacin and moxifloxacin. Levofloxacin has been demonstrated in in vivo and in vitro studies to be up to four times more active than ofloxacin. The bactericidal activity of ofloxacin resides primarily in the L-isomer and this is thought to be related to the higher binding affinity of the L-isomer to the DNA-DNA gyrase complex. Therefore, levofloxacin is by its nature, twice as active as ofloxacin per unit of mass. Like other fluoroquinolones, levofloxacin acts by inhibiting two bacterial enzymes that control the topological state of DNA: DNA gyrase and topoisomerase IV. The primary target of levofloxacin in Gram-negative bacteria such as Escherichia coli and Neisseria gonorrhoeae is DNA gyrase, while topoisomerase IV is the primary target in Gram-positive cocci such as S. aureus and S. pneumonia. The antimicrobial action is characterised by concentration-dependent bactericidal activity and the ability to induce a post-antibiotic effect against a range of bacteria. 3 In addition, levofloxacin is at least 10 times more soluble than ofloxacin and 400 times more soluble than ciprofloxacin in water at neutral pH. This characteristic may contribute to its increased penetration into the aqueous humour compared with the earlier generation fluoroquinolones norfloxacin, ciprofloxacin, or ofloxacin.8 Current Formulary Status The North Staffordshire Joint Formulary currently lists the following agents: 11.3 ANTI-INFECTIVE EYE PREPARATIONS 11.3.1 Antibacterials Gentamicin Ofloxacin Therapeutic class and mode of action:3 Levofloxacin is a synthetic antibacterial agent of the fluoroquinolone class with the L-isomer of the racemic drug substance ofloxacin. The antibacterial activity of ofloxacin resides primarily in the L-isomer. Levofloxacin inhibits bacterial type II topoisomerases—DNA gyrase and topoisomerase IV. Levofloxacin preferentially targets DNA gyrase in Gram-negative bacteria and topoisomerase IV in Gram-positive bacteria. Licensed Indications:3 Oftaquix® 5 mg/ml eye drops are indicated for the topical treatment of bacterial external ocular infections in patients 1 year of age caused by levofloxacin susceptible microorganisms. Dosage and Administration:3 One ml of eye drops, solution, contains 5.12 mg of levofloxacin hemihydrate equivalent to 5 mg of levofloxacin Posology For all patients instil one to two drops in the affected eye(s) every two hours up to 8 times per day while awake for the first two days and then four times daily on days 3 through 5. 4 If different topical ocular medications are used concomitantly, at least a 15-minute interval is required between instillations. To prevent contaminating the dropper tip and solution, the dropper tip should not come into contact with the eyelids or surrounding areas. The duration of treatment depends on the severity of the disorder and on the clinical and bacteriological course of infection. The usual treatment duration is 5 days. Safety and efficacy in the treatment of corneal ulcer and ophthalmia neonatorum has not been established. Use in the Elderly No adjustment of dosage is required. NICE and other guidance NONE Efficacy 1. The pharmacokinetics and ocular bioavailability of levofloxacin in an open-label study9 A 2 day, open-label, single centre study of levofloxacin concentrations in human tears following a single topical administration of 0.5% levofloxacin ophthalmic solution in 30 healthy adult volunteers with asymptomatic eyes. The objective of the study was to assess the pharmacokinetics and ocular bioavailability of levofloxacin in human tears, and to determine the tear concentration of levofloxacin. Each volunteer received 1 drop of 0.5% levofloxacin in each eye and were assigned 1 of 5 groups with 9 defined time point for tear sampling after administration from 5 minutes to 24 hours after administration. Six tear samples were collected at each time point (1 eye each from 6 volunteers), except at 24 hour time point, at which 12 samples were collected (both eyes of 6 volunteers. All volunteers had a baseline Schirmr tear test of 10 mm or more in each eye, and a best corrected visual acuity score of +0.3 logMar in each eye. Levofloxacin concentrations were measured using reverse-phase high-performance liquid chromatography. At 5 minutes after administration of a single topical dose of levofloxacin, the mean tear concentration was 49.19 +/- 26.73 microgram/mL. The mean peak concentration of levofloxacin in the tear film, 221.06 +/- 256.68 microgram/mL, was reached at 15 minutes after administration. At 4 hours after administration, the mean tear concentration of levofloxacin was 17.04 +/- 15.13 microgram/mL. At 6 hours after administration, the mean concentration of levofloxacin was 6.57 +/- 5.26 5 microgram/mL. At 24 hours after administration, levofloxacin concentrations > 2 microgram/mL were measured in 2 of 6 (33%) subjects. Only 2 of 30 volunteers reported adverse event which were both mild (stinging and decreased vision) as they resolved without treatment. There were no notable changes from baseline in mean visual acuity during the study and no subject experienced a change from baseline of >0.2 logMar units. One subject experienced a transient decrease in visual acuity in 1 eye secondary to chemosis. The authors concluded that levofloxacin concentrations in the tear fluid after a single topical dose (1 drop) reached high levels quickly and remained above the minimum inhibitory concentration (MIC) for most suspected ophthalmic pathogens (< 2 microg/mL) for at least 6 hours in most healthy volunteers, and for up to 24 hours in some volunteers. 2. Aqueous humour levels of levofloxacin compared to ciprofloxacin10 A total of 59 patients (16 males, 43 females; mean age 67.2 ± 15.4 years) undergoing elective cataract surgery were randomly assigned to topical treatment with either levofloxacin 0.5% or ciprofloxacin 0.3% eye drops, at one drop every 15 min for four doses immediately prior to surgery. The purpose of the study was to compare aqueous humour levels of levofloxacin and ciprofloxacin following topical application to patients scheduled for cataract surgery. Patients were not eligible for participation in the study if they failed to meet standard provisions regarding antibiotic treatment in the previous week or required the use of any topical or systemic medication that could interfere with study measurements. Patients with pre-existing corneal disorders, uveitis or glaucoma were excluded. At the beginning of the cataract operation, 50 µl of aqueous humour were withdrawn from the anterior chamber via a cannula attached to a tuberculin syringe after paracentesis. The concentrations of levofloxacin and ciprofloxacin in the aqueous humour were analysed using high performance liquid chromatography. Only 55 patients (30 were levofloxacin group and 25 were in ciprofloxacin group) had adequate aqueous humour samples. 29 right eyes (19 in the levofloxacin group and 10 in the ciprofloxacin group) and 30 left eyes (12 in the levofloxacin group and 18 in the ciprofloxacin group) were operated on. About 80% of the patients in both groups had visual acuity of 0.5 or less in the eye to be operated on. The mean axial length of eyes to be operated on was 25.1 ± 3.2 mm in the levofloxacin group and 24.2 ± 2.8 mm in the ciprofloxacin group. No clinically significant changes were seen in the group means of intraocular pressure (IOP) during the course of the study. The results showed that the mean and median concentrations (µg/ml), and the minimum, maximum and lower quartile (Q1, 25%) and upper quartile (Q3, 75%) values of levofloxacin were significantly higher than ciprofloxacin in the aqueous humour samples. Although the concentration of levofloxacin (0.5%) in the ophthalmic drops tested was only 1.67 times that of 6 ciprofloxacin in the control drops (0.3%), the (geometric) mean concentration of levofloxacin in aqueous humour (0.728 µg/ml) was 9.1 times that of ciprofloxacin (0.080 µg/ml). The difference was statistically highly significant (95% CI: 5.9–14.1; p < 0.0001). The authors concluded that levofloxacin achieves 9.1 times the aqueous humour concentration of ciprofloxacin. It could be considered a better choice than ofloxacin or ciprofloxacin for topical ophthalmic use. 3. Aqueous humour levels of levofloxacin compared to ofloxacin11 This was a randomised investigator-masked study of 69 patients who received 4 drops of either levofloxacin 0.5% or ofloxacin 0.3% eye drops within 1 hour (60 min, 45 min, 30 min, and 15 min) of elective cataract surgery. The eye drops were administered in the absence of the surgeon. Aqueous humour samples of at least 50 µL were drawn from the anterior chamber at the beginning of the cataract operation. The concentrations of the fluoroquinolones in the anterior chambers were measured using high-performance liquid chromatography. To exclude a dilution effect of the anterior chamber (AC), they were related to the AC volumes and AC depths (measured by ultrasound). An early postoperative examination (1-2 hours after surgery) consisted of biomicroscopy and measurement of the intraocular pressure as well as an inquiry into possible adverse events. The aim of the study was to investigate the penetration of topically applied levofloxacin 0.5% and ofloxacin 0.3% eye drops into the aqueous humour of patients having cataract surgery. The mean concentration of levofloxacin (1139.9 ng/mL +/- 717.1 [SD]) in the aqueous humour was significantly higher (P = 0.0008) than that of ofloxacin (621.7 +/- 368.7 ng/mL). The aqueous humour concentrations correlated negatively with the measured volumes and depths of the ACs. The authors concluded that levofloxacin, is more soluble in water enabling the use of higher drug concentrations (0.5%) compared with other currently available fluoroquinolone eye drops (0.3%). The concentration AC with levofloxacin eye drops was about 2-fold that reached with ofloxacin eye drops. The concentration of the antibacterial isomer was approximately 3.5 to 4 times higher when levofloxacin was administered. 4. Levofloxacin versus fortified antibiotics (amikacin and cefazolin) for treating bacterial keratitis12 A prospective, double-blinded, randomized controlled clinical trial was conducted in 71 eyes from 69 patients suspected of having infectious bacterial keratitis. The patients were randomized into two arms, 0.5% levofloxacin eye drops (34 eyes) or fortified cefazolin 5% and amikacin 5% (37 eyes). 68 eyes were included in the efficacy analysis. During treatment, on days 2, 7, 14, and 21, the patient’s symptoms and signs were scored from grade 0-3 (absent to severe). 7 Both groups would apply their assigned medications every 10 minutes during the first 30 minutes of treatment and later decreased it to one hour every three days. On days 4-7, one drop was used every two to four hours depending on the patients’ clinical responses. After day 7, topical antibiotics were tapered to every six hours and discontinued when there was evidence that the ulcer had completely healed. During treatment, the patients were followed on days 2, 7, 14, and 21. During each visit, the patient’s symptoms and signs were assessed using scores from grade 0-3 (absent to severe). Symptoms accessed were for discomfort, pain, tearing, photophobia, and itching. Changes in clinical signs, such as swollen eyelids, chemosis, and conjunctival hyperaemia were evaluated using biomicroscopy examination. Those patients whose symptoms worsened or did not respond to the assigned drugs were considered as failures, and subsequently withdrew from the study. The primary outcome of this study was to assess the resolution of keratitis (healed or not healed). Cured or healed ulcer was defined as no corneal infiltration, no sign of inflammation and complete epithelial healing. Treatment failure was defined as those who were unresponsive to their treatment and showed no clinical improvement or worsening of clinical signs within 72 hours. At the end of the treatment, 61 out of 71 eyes completely healed. There were no statistical differences for the resolution of keratitis (p=0.81) and mean time to heal between the two groups (p=0.92). Further analysis of the mean time-duration to heal by the severity of the ulcer also showed no statistically significant differences between groups (Mild ulcers had a p-value of 0.50. Severe ulcers had a p-value of 0.75). Concerning the timeduration for the clinical signs (p=0.37) and symptoms (p=0.38) to disappear, they did not observe any statistical differences between groups. The patients compliance was 80% based on the self-reported diaries. The authors concluded that the efficacy and safety of 0.5% topical levofloxacin was comparable to fortified cefazolin 5% and amikacin 5% for the treatment of mild-to-moderate bacterial keratitis. Safety and adverse effects:3 Contraindication: Hypersensitivity to the active substance levofloxacin, to other quinolones or to any of the excipients, e.g. benzalkonium chloride. Adverse effect: Approximately 10% of patients can be expected to experience adverse reactions. The reactions are usually graded as mild or moderate, are transient, and are generally restricted to the eye. As the product contains benzalkonium chloride, contact eczema and/or irritation may be due to the active component or to this preservative. 8 Common (1/100 to <1/10): ocular burning, visual disturbances and mucous strand. Drug Interactions:3 Uncommon (>1/1,000, <1/100): headache, rhinitis, conjunctival follicles. Specific drug interaction studies have not been conducted with Oftaquix 5 mg/ml eye drops. Since maximum plasma concentrations of levofloxacin after ocular administration are at least 1000 times lower than those reported after standard oral doses, interactions mentioned for systemic use are unlikely to be clinically relevant when using Oftaquix 5 mg/ml eye drops. Pregnancy and lactation Pregnancy: There are no adequate data from the use of levofloxacin in pregnant women. Animal studies are insufficient with respect to effects on pregnancy and embryonal/foetal development and parturition and postnatal development. The potential risk for humans is unknown. Oftaquix 5 mg/ml eye drops should be used during pregnancy only if the potential benefit justifies the potential risk to the foetus. Lactation: Levofloxacin is excreted in human milk. However, at therapeutic doses of Oftaquix no effects on the suckling child are anticipated. Oftaquix 5 mg/ml eye drops should be used during lactation only if the potential benefit justifies any potential risk to the nursing child. Presentation:3 Eye drops, solution, clear, light yellow to light greenish-yellow solution, practically free of visible particulate matter. 9 Costing: Dr Pherwani estimated that 15-20 patients will be treated per year. The estimated expenditure per year per treatment course (190 drops) will be £1,795.50 - £2,394.00 when the single dose units are used. UHNS expenditure for a 12-month period (January-December 2012): UHNS Lloyds Approximate Epact (Discount & Fees not included) Total Gentamicin 1.5% £1,666.24 £42.84 £0 £1,709.08 Cefuroxime 5% £4,576.02 £213.91 £193.43 £4,983.36 Ciprofloxacin 0.3% £65.34 £75.84 £202.10 £343.28 Levofloxacin 0.5% £1,461.59 £596.21 £632.67 £2,690.47 Moxifloxacin 0.5% £0.00 £0.00 £0.00 £0.00 £7,250.76 £277.43 £522.97 £8,051.16 Ofloxacin 0.3% 10 Cost Analysis Cost comparison to other antibacterial eye drops with broad spectrum activity: Product Gentamicin 1.5% plus Cefuroxime 5% Ofloxacin 0.3% Levofloxacin 0.5% Formulary status Dosing freq. Pack size Price per pack 5ml £24.42 Non Formulary 1 drop every hour Day and Night for 2/7, then every hour by Day for 2/7, then every 2 hourly for 4/7, then 6 times per day for 7/7, then QDS for 7/7. 5ml £55.44 Formulary Non Formulary Ciprofloxacin 0.3% Non Formulary Moxifloxacin 0.5% Non Formulary 1 drop every hour Day and Night for 2/7, then every hour by Day for 2/7, then every 2 hourly for 4/7, then 6 times per day for 7/7, then QDS for 7/7. 1 drop every hour Day and Night for 2/7, then every hour by Day for 2/7, then every 2 hourly for 4/7, then 6 times per day for 7/7, then QDS for 7/7. 1 drop every hour Day and Night for 2/7, then every hour by Day for 2/7, then every 2 hourly for 4/7, then 6 times per day for 7/7, then QDS for 7/7. 1 drop every hour Day and Night for 2/7, then every hour by Day for 2/7, then every 2 hourly for 4/7, then 6 times per day for 7/7, then QDS for 7/7. Price per Course £73.26 £166.32 £239.64 5ml £1.98 £5.94 5ml £7.32 £21.96 30 x 0.5ml 18.90 £109.62 5ml £1.98 £5.94 5ml £11.76 £35.28 11 References 1 British National Formulary (BNF) 64 September 2012. Accessed via www.bnf.org Kresken M. et al. Effectiveness of levofloxacin Eye Drops – A Microbiological Perspective. European Ophthalmic Review, 2009, 2(1):12-5. 3 Summary of Product Characteristics Oftaquix® (levofloxacin) 5 mg/ml eye drops 4 Van Bambeke F, et al. Quinolones in 2005: an update. Clin Microbiol Infect, 2005; 11: 256-80. 5 Hooper DC. Quinolone mode of action. Drugs, 1995;49 (Suppl. 2):10-15. 6 Ross DL, Riley CM. Aqueous solubility of some variously substituted quinolone antimicrobials. Int J Pharm 1990;63: 237–50. 7 Mitsui Y, Ooishi M, Sasaki K, Ohashi Y. AQCmax as a pharmacokinetic parameter of ophthalmic solution. J Eye 1995;12:783–6. 8 Sasaki K, Mitsui Y, Fukuda M, et al. Intraocular penetration mode of five fluoroquinolone ophthalmic solutions evaluated by the newly proposed parameter of AQCmax. J Eye 1995;12: 787–90. 9 Raizman MB, Rubin JM, Graves AL, Rinehart M. Tear concentrations of levofloxacin following topical administration of a single dose of 0.5% levofloxacin ophthalmic solution in healthy volunteers. Clin Ther. 2002; 24(9):1439-50. 10 Colin J., Simonpoli S. et al. Corneal penetration of levofloxacin into the human aqueous humour: a comparison with ciprofloxacin. Acta Ophthalmol. Scand. 2003; 81:611-613. 11 Koch HR, Kulus SC et al. Corneal penetration of fluoroquinolones: aqueous humor concentrations after topical application of levofloxacin 0.5% and ofloxacin 0.3% eyedrops. J Cataract Refract Surg. 2005; 31(7):1377-85. 12 Kasetsuwana N, Tanthuvanit P. et al. The efficacy and safety of 0.5% Levofloxacin versus fortified Cefazolin and Amikacin ophthalmic solution for the treatment of suspected and culture-proven cases of infectious bacterial keratitis: a comparative study. Asian Biomedicine. 2011; 5: 77-83. 2 Produced by Sr. Maria Chidiamara Njoku Primary Care/Secondary Care Interface Pharmacist University Hospital of North Staffordshire Telephone: 01782 674541 e-mail: [email protected] Produced for use within the NHS. Not to be reproduced for commercial purposes. 12