Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
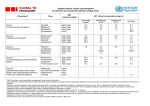
Pharmacy & Therapeutics Committee News July 2015 Fluoroquinolone Formulary Change: Levofloxacin to Replace Moxifloxacin – Start Date: 7/21/15 Both levofloxacin and moxifloxacin are respiratory fluoroquinolones. Unlike ciprofloxacin, both agents have excellent activity against Streptococcus pneumoniae and can be used for the treatment of community acquired pneumonia (CAP). Another important difference is that levofloxacin has activity against Pseudomonas aeruginosa while moxifloxacin does not. Due to the fact that levofloxacin is available generically for both the IV and oral preparations, the P&T committee decided to replace moxifloxacin with levofloxacin on the hospital formulary. This will result in significant cost savings. Note that ciprofloxacin will remain on formulary for the treatment of Pseudomonas infections, since ciprofloxacin has slightly better activity against SJH Pseudomonas isolates. Although the fluoroquinolone class has FDA indications for a variety of infections, this class of antimicrobials is associated with an increased risk of Clostridium difficile. This includes the NAP1 strain, which can cause severe cases of colitis requiring colectomies and resulting in an increased risk of mortality. For this reason and the increased risk of resistance, fluoroquinolones are NOT the first line option for either pneumonia or urinary tract infections. Approved indications for levofloxacin include: CAP in patients with documented anaphylaxis to the beta-lactam class of antibiotics Other indications will be based on the specific organism and the patient’s allergy history The Antibiotic Stewardship Team reviews every fluoroquinolone order for appropriate use. Auto-substitution conversion of moxifloxacin IV/PO to levofloxacin IV/PO If ordered for Pneumonia Moxifloxacin 400mg IV/PO q 24h Moxifloxacin 400mg IV/PO q 24h Moxifloxacin 400mg IV/PO q 24h And the estimated creatinine clearance is… ≥ 50 ml/min 20-49 ml/min 10-19 ml/min OR hemodialysis Pharmacist will convert to… Levofloxacin 750mg IV/PO q 24h Levofloxacin 750mg IV/PO q 48h Levofloxacin 750mg IV/PO x 1, then 500mg IV/PO q 48h Pneumonia Pathway Revisions The goal of the pneumonia pathway is to ensure patients receive evidence based treatment regimens and appropriate diagnostic tests to improve overall outcomes. The pathway was reviewed with the Infectious Diseases Physicians and the following recommendations were made: Community Acquired Pneumonia: No risk for Pseudomonas Levofloxacin IV/PO replaces Moxifloxacin IV/PO for CAP patients with anaphylaxis to beta-lactam antibiotics. A comment was added to choose doxycycline for atypical coverage in patients with QTc prolongation. There is also data that the use of doxycycline may decrease the risk of Clostridium difficile when combined to ceftriaxone. o Doernberg SB, Winston LG, Deck DH, Chambers HF. Does doxycycline protect against development of Clostridium difficile Infection. Clin Infect Dis 2012;55(5):615-20. A 5 day stop was added to azithromycin therapy. Community Acquired Pneumonia: Pseudomonas risk or Health-Care Associated Pneumonia For Non-ICU patients: There will no longer be double pseudomonas coverage with ciprofloxacin and piperacillin-tazobactam or cefepime, since the 2015 antibiogram shows Pseudomonas isolates have a 91% sensitivity to piperacillin-tazobactam and 97% sensitivity to cefepime. Azithromycin or doxycycline was added for atypical coverage. For ICU patients: The regimen of Piperacillin-tazobactam + ciprofloxacin + Vancomycin was added which is consistent with the sepsis pathway. When vancomycin IV is ordered for MRSA coverage, a MRSA nasal screen by PCR will automatically be ordered. This test is rapid and has a 98-99% negative predictive value. If this test is negative, providers should consider discontinuing vancomycin therapy. Patients will not require isolation while the result is pending. 2015 Antibiogram The 2015 Inpatient and Outpatient Antibiogram is now available electronically on the Pharmacy Website under Pharmacy Reference Materials or on the Antibiotic Stewardship Page. For printed copies, please email Lisa Avery, Pharm.D. @ [email protected] Highlighted Antibiogram Issues E.coli sensitivities to Ciprofloxacin or levofloxacin are only 77%. This makes fluoroquinolones inappropriate empiric therapy for UTIs or intra-abdominal infections. MRSA accounts for 44% of all Staphylococcus aureus isolates. Only 62% of community-wide Streptococcus pneumoniae isolates are sensitive to azithromycin. This is due to the overuse of Z-Paks. New Cephaloporins Added to Restricted Medication List – Restricted to ID The following antibiotics have a “first dose restriction” and may be ordered by Infectious Disease physicians. Avycaz is restricted to carbapenamase producing enterobactericiae (CRE) and Zerbaxa is restricted to resistant pseudomonas isolates. Brand Name FDA Indications Dose Dose Adjustment for Clcr Contraindication Warnings Adverse Drug Reactions Drug Interactions Cost Ceftolozane-tazobactam Zerbaxa Complicated intra-abdominal in combination with metronidazole Ceftazidime-avibactam Avycaz Complicated intra-abdominal in combination with metronidazole Complicated UTI - Pyelonephritis 1.5g IV q 8h 30-50 ml/min 750mg IV q 8h 15-29 ml/min 375mg IV q 8h ESRD on HD 750mg x 1, then 150mg IV q 8h Allergy to piperacillin-tazobactam and other members of the beta-lactam class Decreased efficacy in patients with a creatinine clearance 30 to <50 ml/min Nausea, diarrhea, headache, pyrexia Complicated UTI - Pyelonephritis 2.5g IV q 8h 31-50 ml/min 1.25g IV q 8h 16-30 ml/min 0.94g IV q 12h 6-15 ml/min 0.94g IV q 24h ≤ 5 ml/min 0.94g IV q 48h Allergy to ceftazidime/avibactam None 1.5g = $83 1.5g IV q 8h = $249 per day Decreased efficacy in Clcr 30-50 ml/min CNS – seizures (renal impairment) Vomiting, nausea, constipation, anxiety Avibactam is a substrate of OAT1 and OAT3 transporters. Do not coadminister probenecid. 2.5g = $267 2.5g IV q 8h = $801 per day How to request a nonformulary drug for use in one specific patient (aka Fast Track Process) All requests for nonformulary products will require completion of a fast-track request form located on-line in the forms catalog (Form # 20207). Please alert your pharmacist as soon as possible when considering these products. All requests require Pharmacy & Therapeutics Committee Leadership and VPMA approval before an order for the product can be placed. Retrospective review of all “fast-tracks” will occur at the following P & T meeting. How to request addition or status change to the Formulary Formulary additions, deletions and new policy development or revisions may be requested using the Form #18711. Formulary requests should only be completed by medical or hospital staff; requests from vendors are unacceptable. Meeting Schedule The P & T Committee meets monthly (with some exceptions) on the fourth Tuesday morning each month in Room 201B at 0700. Approvals are forwarded to the next possible Medical Department and Medical Executive Committee meetings. The July P & T Committee meeting has been cancelled. For more information on Antimicrobial actions, please email Lisa Avery, Infectious Disease Pharmacist [email protected] For more information on Pharmacy & Therapeutics Committee actions, please contact Karen Whalen, Drug Information Pharmacist 448-6519.