Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Chagas disease wikipedia , lookup
Neglected tropical diseases wikipedia , lookup
Cryptosporidiosis wikipedia , lookup
Carbapenem-resistant enterobacteriaceae wikipedia , lookup
Gastroenteritis wikipedia , lookup
Anaerobic infection wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Onchocerciasis wikipedia , lookup
West Nile fever wikipedia , lookup
Henipavirus wikipedia , lookup
Leptospirosis wikipedia , lookup
Hepatitis C wikipedia , lookup
Marburg virus disease wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Hepatitis B wikipedia , lookup
Trichinosis wikipedia , lookup
Dirofilaria immitis wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Schistosomiasis wikipedia , lookup
Mass drug administration wikipedia , lookup
Sarcocystis wikipedia , lookup
Neonatal infection wikipedia , lookup
Oesophagostomum wikipedia , lookup
Fasciolosis wikipedia , lookup
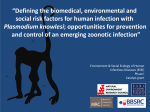
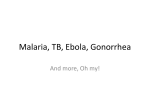
EMERGING INFECTIONS INVITED ARTICLE James M. Hughes and Mary E. Wilson, Section Editors Review of Cases With the Emerging Fifth Human Malaria Parasite, Plasmodium knowlesi Anu Kantele1,2,3 and T. Sakari Jokiranta3 1Division of Infectious Diseases, Department of Medicine, Helsinki University Central Hospital, 2Department of Medicine, University of Helsinki, and of Bacteriology and Immunology, Haartman Institute, University of Helsinki, Helsinki, Finland 3Department Human malaria has been known to be caused by 4 Plasmodium species, with Plasmodium falciparum causing the most-severe disease. Recently, numerous reports have described human malaria caused by a fifth Plasmodium species, Plasmodium knowlesi, which usually infects macaque monkeys. Hundreds of human cases have been reported from Malaysia, several cases have been reported in other Southeast Asian countries, and a few cases have been reported in travelers visiting these areas. Similarly to P. falciparum, P. knowlesi can cause severe and even fatal cases of disease that are more severe than those caused by the other Plasmodium species. Polymerase chain reaction is of value for diagnosis because P. knowlesi infection is easily misdiagnosed as less dangerous Plasmodium malariae infection with conventional microscopy. P. knowlesi infection should be suspected in patients who are infected with malaria in Southeast Asia. If human–mosquito–human transmission were to occur, the disease could spread to new areas where the mosquito vectors live, such as the popular tourist areas in western India. More than half of the world population lives in malaria risk areas in Africa, Central and South America, and South and Southeast Asia, and the annual malariaassociated mortality approaches 1 million, with 2 children dying from the disease every minute worldwide (World Malaria report 2009, WHO). For the past 80 years, human malaria has been known to be caused by 4 Plasmodium species—Plasmodium falciparum, Plasmodium vivax, Plasmodium ovale, and Plasmodium malariae—with P. falciparum being responsible for the most-severe cases. Recently, a fifth Plasmodium species has been recognized as a cause of malaria in humans. The newcomer is Plasmodium knowlesi, which was formerly known to cause malaria only in macaques. Received 9 November 2010; accepted 22 February 2011. Correspondence: Anu Kantele, MD, PhD, Div of Infectious Diseases, Helsinki University Central Hospital, P.O.Box 348, FIN-00029 HUS, Finland (anu.kantele @hus.fi). Clinical Infectious Diseases 2011;52(11):1356–1362 Ó The Author 2011. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please e-mail: [email protected]. 1058-4838/2011/5211-0014$14.00 DOI: 10.1093/cid/cir180 1356 d CID 2011:52 (1 June) d EMERGING INFECTIONS HISTORY First described in 1931 in a longtail macaque (Macaca fascicularis), P. knowlesi was later found to cause naturally acquired malaria in pigtail macaques (Macaca nemestrina) and the mitred leaf monkey (Presbytis melalophos), as well. Experimentally, P. knowlesi infects several other primates, and in 1932, P. knowlesi was proved to infect humans. Iatrogenic P. knowlesi infection was initially considered to be nonhazardous, and therefore, the parasite replaced P. vivax as a pyretic agent in the treatment of neurosyphilis in the early 1930s. This practice was discontinued, however, as a result of patient deaths [1]. It was not until 1965 that the first natural infection of P. knowlesi in humans was reported in an American traveller returning from Peninsular Malaysia [2]. In 1971, another natural infection was suspected in Peninsular Malaysia [3]. Despite extensive studies in Malaysia in the 1960s, no additional reports appeared until 2004, when Singh et al [4] described 120 cases of naturally acquired P. knowlesi infection in humans in Malaysian Borneo. Since then, numerous reports have been published. By analyzing old blood films, P. knowlesi has been shown to have caused malaria in a great number of patients since 1996 [5]. MONKEY MALARIA At least 26 Plasmodium species are known to infect primates, yet natural transmission of a nonhuman Plasmodium species to humans is rare. The host specificity has been shown to be surprisingly strict: eg, Plasmodium reichenowi causing malaria in chimpanzees fails to infect humans [6]. Similarly, P. falciparum causes only mild parasitemia in chimpanzees. These kinds of differences appear to be caused by species-specific erythrocyte recognition profiles [6] or different binding of sporozoites to liver cells [7]. P. knowlesi is clearly not strictly species-specific, because both experimental monkey-to-human and human-tohuman transmission have proved to be possible [8]. Other mechanisms of species specificity of plasmodia are attributable to vector restriction, vector feeding preferences, and vector species specificity. P. knowlesi transmission is vector restricted in that the parasite can be transmitted only by certain Anopheles mosquitoes [1, 9]. At least 2 main vectors in the Anopheles leucosphyrus group, Anopheles latens and Anopheles cracens, are known to be forest feeders, biting both humans and macaques at evening or during the night [9, 10]. Taken together, numerous mechanisms restrict the nonhuman Plasmodium species from infecting humans, yet P. knowlesi has proved to make a significant exception to this rule. In the natural hosts, P. knowlesi causes an asymptomatic lowgrade parasitism or mild disease [4, 10]. It is not known whether human P. knowlesi infections are obtained only from mosquitoes fed on macaques or whether natural human-mosquito-human transmission occurs. The zoonotic nature of the infection is suggested by the lack of case clustering in Sarawakian human settlements, where most cases have been described, and by the fact that most patients have a recent history of working or dwelling in a forest or forest fringe, which is the environment characteristic of the vector mosquitoes [10, 11]. During human infection, gametocytes are formed, but at low levels, which supports the suggestion that transmission is primarily zoonotic [12]. Because of the environmental preference of the natural vector mosquitoes, urban transmission is not likely to occur. The situation might change if human-mosquito-human transmission occurred, because at least one widely distributed urban mosquito species (Anopheles stephensi) has experimentally been shown to be a possible vector for P. knowlesi (reviewed by Coatney et al [1]). CASES IN MALAYSIA In the first study to recognize P. knowlesi as a causative organism of human malaria in Sarawak, Malaysia, the authors investigated cases that were identified by microscopic examination as being due to P. malariae but that had negative polymerase chain reaction (PCR) results [4]. When new primers were applied, 58% of the cases that originally had PCR results negative for P. malariae were found to have positive results for P. knowlesi, resulting in the identification of 120 cases of P. knowlesi infection in humans. Thereafter, P. knowlesi was identified in 266 of the samples from 960 hospitalized Sarawakian patients with malaria [13], in 41 of 49 archived blood-films collected in Sabah [13], and 35 of 47 in Sarawak [5], in Malaysian Borneo, and in a total of 89 cases in Peninsular Malaysia [9, 13, 14]. In 2009, a prospective report on P. knowlesi infections in Sarawak was published that contained the clinical picture and the laboratory findings for 107 patients with P. knowlesi infection during 2006–2008 [15]. Since 2004, 5 fatal cases have been reported [13, 16]. CASES IN OTHER SOUTHEAST ASIAN COUNTRIES After identifying cases in Malaysia, several patients with P. knowlesi infection have been documented in other Southeast Asian countries (Figure 1; Table 2). Diagnosis in all of these cases was based on PCR analysis, but malaria was detected in practically all of the cases using microscopy. In 2004, P. knowlesi malaria was described in a patient who lived in a suburb of Bangkok, Thailand, and who had visited southern Thailand near the Myanmar border [27]. Subsequently, P. knowlesi has been identified in 10 patients from southern and southwestern Figure 1. Plasmodium knowlesi infections reported in humans in Southeast Asia (modified from Cox-Singh and Singh [10]). The gray area indicates the geographic distribution of Anopheles leucosphyrus group mosquitoes, which are the main vectors for P. knowlesi. The figures represent numbers of patients with a reported infection due to P. knowlesi. The figures include both local patients and travelers returning from that area. For 1 traveler, the area in which the infection was obtained remained unclear, because he had visited several countries (Thailand, Indonesia, Peninsular Malaysia, and Vietnam) [17]. EMERGING INFECTIONS d CID 2011:52 (1 June) d 1357 Thailand [28]; 33 patients from Myanmar [29, 30]; 5 patients, including 2 patients with a history of staying in forest areas, from the Philippines [32]; 2 soldiers and 4 other patients from northwestern Singapore [24–26]; 5 patients from central Vietnam [31]; and 1 patient, a gold miner from southern Borneo, in Indonesia [21]. As Sulistyaningsih et al [21] have concluded, it appears to be possible that the parasite is widely distributed throughout Borneo. CASES IN TRAVELERS After the first reported case of P. knowlesi infection in a traveler (Table 2) in 1965 [2], the next case was reported 42 years later. In 2007, a Finnish man was infected during a 4-week visit to Peninsular Malaysia, where he stayed in a jungle area for 5 days [23]. He did not take any malaria prophylaxis, and his illness was originally diagnosed by microscopy as coinfection due to P. falciparum and P. malariae. This and the next few cases were confirmed using PCR and sequencing or P. knowlesi–specific nested PCR. The third reported case was in a Swedish man who had been travelling in Malaysian Borneo for 2 weeks and stayed in a jungle for 1 week. Rapid diagnostic test results for malaria was negative, but microscopic examination revealed low parasitemia with a suspicion of P. malariae infection [18]. The fourth report described a woman from the United States who had visited the Philippines, her native country [33]. The fifth case was in a Malaysian immigrant in the Netherlands [19]. The sixth traveller documented with P. knowlesi infection was an Australian man working 10 days a month near woodlands in Indonesian Borneo in the province located farthest from the Malaysian border [22]. The seventh case was in a Spanish man who had returned from a long tour in Southeast Asia [17]. In addition to these reports, the British health statistics list 1 case of P. knowlesi infection in 2006 in a patient who had visited Brunei [20]. CLINICAL PICTURE AND OUTCOME The clinical picture and outcome of P. knowlesi infection is described in a prospective study involving 107 patients in theSarawak hospital in Malaysia during the period 2006–2008 [15]. The clinical and laboratory profiles of these patients resembled those of patients infected with other Plasmodium species. A Vietnamese report suggests that asymptomatic infections may also occur [34]. In Malaysia, the patients with P. knowlesi infection typically presented with a nonspecific febrile illness with daily fever and chills. Other frequent symptoms included headache, rigors, malaise, myalgia, abdominal pain, breathlessness, and productive cough. Tachypnea, pyrexia, and tachycardia were common clinical signs. All patients had thrombocytopenia at hospital admission or on the following 1358 d CID 2011:52 (1 June) d EMERGING INFECTIONS day, yet none of the patients had clinical coagulopathy. At hospital admission, only a few of the patients had anemia, whereas mild hepatic dysfunction was relatively common. The great majority of patients (94%) experienced no complications, and the infection responded well to chloroquine and primaquine treatment [15]. Applying the World Health Organization criteria for P. falciparum infection, P. knowlesi infection was evaluated as severe in 7% of the cases, with the most frequent complication being respiratory distress with pulmonary rather than metabolic etiology. A strong correlation was found between parasite density and the development of respiratory distress. Parasite density was also strongly and independently associated with renal dysfunction. Two of the patients died, representing a case fatality rate of 1.8% [15]. Phylogenically, P. knowlesi is relatively closely related with P. vivax; therefore, it is not surprising that infections with these 2 species share some common features, such as occasional severity and marked thrombocytopenia [35]. However, disease caused by P. knowlesi is somewhat more severe than disease caused by P. vivax, although also vivax malaria can be severe in a significant number of cases, at least in certain regions (severe malaria in 3%, compared with 7% in individuals with P. knowlesi malaria) [15, 35]. In P. knowlesi infections, neurological symptoms are rare, and no cases of cerebral malaria have been reported [15]. A post-mortem study of a lethal P. knowlesi case suggests, however, that P. knowlesi–infected red cells can sequester in capillaries of the brain, heart, and kidneys [16]. Similarly to P. falciparum, P. knowlesi can cause severe or even fatal disease. It has a short lifecycle of 24 h [1], enabling a rapid progression of the disease (Table 1). The erythrocyte invasion by P. knowlesi is not restricted to young or old cells, which allows high parasitemia, and development of the parasite in erythrocytes is asynchronous. The threshold for hyperparasitemia in P. knowlesi infections is lower than in P. falciparum malaria and, at least theoretically, hyperparasitemia, together with the shorter asexual cycling time, may even render P. knowlesi more virulent in its severe form. In 3 of the 5 reported lethal cases, a high parasitemia was seen (15%, .10%, and .10 parasites per high-power microscope field) [13, 16]. Clinicians treating these patients should be aware of the potential lethal outcome of the infection. TREATMENT As malaria due to P. knowlesi might progress rapidly into severe disease, it should be treated like P. falciparum malaria if the species identification is based on microscopic examination alone or if coinfection with P. falciparum cannot be excluded with certainty using PCR. P. knowlesi itself appears to be susceptible to numerous alternative treatments (Table 1). The majority of Table 1. The 5 Plasmodium-Species Causing Malaria in Humans Plasmodium falciparum Variable Plasmodium knowlesi Plasmodium vivax Plasmodium ovale Plasmodium malariae Main site of distribution, proportion in the endemic area (%) Global, most common in Africa, 80–90 (Africa) Malaysia (and neighboring areas), 1–60 Mostly in Asia, 50–80 Africa, 5–8 Global, 0.5–3 Life threatening yes yes yes no no Red cells and fever cycle, days Infected red cells Parasitemia 2 1 2 2 3 All All Young cells Young cells Old cells Can be high Can be high ,2% ,2% ,2% Liver hypnozoites No Probably no Yes Yes No Treatmenta Combinations with arthemisinine derivatives Probably all the medications listed for the other plasmodia Chloroquine followed by primaquine Chloroquine followed by primaquine Chloroquine Atovaquone plus proguanil Not known, probably Atovaquone plus proguanil Atovaquone plus proguanil Atovaquone plus proguanil Doxycycline Mefloquine Atovaquone plus proguanil Chloroquine (resistance rare) Chloroquine Chloroquine Doxycycline Doxycycline Chloroquine Doxycycline Mefloquine Mefloquine Doxycycline Mefloquine Mefloquine No preventing medication can prevent liver hypnozoites Atovaquone plus proguanil Mefloquine Quinine 6 doxycycline Medical prevention No preventing medication can prevent liver hypnozoites a If a patient with a P. falciparum infection has high parasitemia, poor condition, and/or complications, intravenous medication (artesunate or quinine with or without doxycycline) is recommended. This probably applies also to P. knowlesi infections requiring intravenous medication. Possible use of chloroquine has been suggested as well [36], but this needs to be further explored before a recommendation can be made. Malaysian patients were primarily treated with chloroquine [4, 15, 36], the Finnish patient was treated with quinine and doxycycline [23], the Swedish patient was treated with mefloquine [18], and the American patient was treated with the combination of atovaquone and proguanil [33]. This suggests that P. knowlesi malaria can be treated with all of these agents (Table 1). In general, antimalarial medication should be commenced at once after patients are found to have positive blood smear results, and the species can be identified or confirmed later. In P. knowlesi infection, commencing medication immediately is as important as it is in P. falciparum infection because of the potentially severe nature of both infections and because of the difficulty in distinguishing between these 2 species or determining whether there is a mixed infection on the basis of microscopic examination alone. Two plasmodium species, P. vivax and P. ovale, may become dormant as liver hypnozoites and can cause one or more relapses of disease even years after the original infection if primaquine is not given to eradicate this form of the parasite (Table 1). After the primary treatment, Malaysian patients have been treated with primaquine to eliminate possible hypnozoites [15, 36]; however, there is no evidence from either macaque or human infections on relapses or indicating that that hypnozoites exist in P. knowlesi infection. Therefore, it appears to be unlikely that primaquine administration is beneficial or necessary in P. knowlesi infection. EMERGING INFECTIONS d CID 2011:52 (1 June) d 1359 Figure 2. Examples of challenges in species identification using microscopy. On the left are photos from thin smears from a Finnish tourist with a Plasmodium knowlesi infection after a visit to western Peninsular Malaysia. In the middle are thin smears from patients with Plasmodium falciparum infection, and on the right are thin smears from patients with Plasmodium malariae infection (Giemsa or May-Grünwald-Giemsastaining; original magnification, 31000). DIAGNOSIS Malaria diagnosis is traditionally based on light microscopy of thin and thick blood smears. In experienced laboratories, microscopy is reliable, but even in such laboratories, its sensitivity is always not optimal [37]. In P. knowlesi infections, microscopic examination has been used to identify plasmodia in the samples and to determine the level of parasitemia. Microscopic examination, however, fails to correctly identify the species of P. knowlesi, because its early trophozoites resemble the ring forms of P. falciparum, and its later stages mimic those of P. malariae (Figure 2) [8]. This explains why P. knowlesi infection is usually misidentified as P. falciparum and/or P. malariae infection [2, 5, 12, 13, 23, 25, 28]. Because P. knowlesi malaria is life threatening, this parasite should always be suspected in cases in which microscopic examination suggests P. malariae, but in which the patient has either severe disease, considerable parasitemia (.0.1%; ie, a parasite count of .5000 parasites/lL), or a recent history of visiting woods or their vicinity in Southeast Asia [5]. The PCR techniques that are used for the diagnosis of malaria and are not specifically designed for detection of P. knowlesi fail to detect it [17, 22, 38]. This parasite has been detected only with P. knowlesi–specific PCR assays that use nested PCR [4, 28], 1360 d CID 2011:52 (1 June) d EMERGING INFECTIONS real-time PCR [38], or PCR combined with sequencing [23]. The widely used nested PCR assay (using the primers Pmk8 and Pmk9r), however, occasionally gives false-positive results in either uninfected or P. vivax–infected individuals [21, 31, 39], indicating that a molecular method to test all 5 human malaria species or verification of identification by sequencing of the PCR product is needed [21, 28, 31]. A more specific set of primers has also been suggested [38, 39]. Although PCR analyses can be done by scraping material from microscopy slides, ethylenediaminetetraacetic acid-anticoagulated blood samples should be used to minimize contamination. In several countries, traditional microscopy-based malaria diagnostics have recently been combined with, or at least partially replaced by, the use of malaria rapid diagnostic tests (RDTs). Some of the kits available are based on detection of plasmodium-specific lactate dehydrogenase, whereas others detect histidine-rich protein II (HRP-2) of P. falciparum either alone or in combination with a pan-malarial antigen, aldolase. Currently, no commercially available RDTs are designed to specifically detect P. knowlesi. Performance of these mainly P. falciparum– and P. vivax–targeted RDTs in P. knowlesi infection has been reported in a few cases [18, 25], which suggests that anti-HRP-2 antibodies do not always recognize P. knowlesi [18], whereas anti-aldolase and anti-LDH antibodies are more reliable [19, 40]. In conclusion, these tests are not recommended because of the unreliable results and low sensitivity in detecting P. knowlesi. Because knowlesi malaria can be symptomatic in patients with low parasitaemia, RDTs should detect it with sensitivity of 1 or even ,1 parasite/lL of blood. PREVENTION OF P. KNOWLESI–INFECTION As with the other types of human malaria, prevention of P. knowlesi infection is based on avoiding mosquito bites and taking preventive medication when indicated. The efficacy of these measures against P. knowlesi has not been shown, but it can be assumed that its vector behaves like the vectors of other Anopheles species, and general precautions for avoiding the bites of Anopheles mosquitoes probably apply. Current indoor control measures for malaria do not, however, prevent zoonotic transmission of malaria by vectors that mainly feed in the forest [9, 10]. Zoonotic P. knowlesi infection can, accordingly, continue to be a problem for malaria control, and also poses a significant threat to the renewed efforts aimed at fully eradicating malaria. None of the tourists with reported P. knowlesi infection used preventive medication [18, 19, 22, 23, 33]. Because chloroquine [4, 15], doxycycline [23], mefloquine [18], or atovaquoneproguanil in combination [22] have been successfully used in treatment of the disease, all of these agents could probably be used as preventive medicines against P. knowlesi, as well. Table 2. Reported Human Plasmodium knowlesi Infections Country/area Malaysia/Borneo Local cases Cases in travelers Reference(s) 570 3 [3, 4, 5, 13, 15]; [2, 18, 19] 1 [20] 1 89 1 1 [21, 22] [9, 13, 14, 23] Brunei/Borneo Indonesia/Borneo Malaysia/Peninsular Singapore 6 [24–26] Thailand 11 [27, 28] Myanmar 33 [29, 30] Vietnam 5 Philippines 5 Total 720 [31] 1 [32, 33] 8a a Area of infection in 1 case was unclear (Thailand, Indonesia, Peninsular Malaysia, or Vietnam) [17]. not necessarily linked to the actual spread of the parasite but to the use of more-accurate diagnostic methods. The high number of human cases (Table 2) suggests that P. knowlesi may be more capable of infecting humans than are the other species that cause nonhuman primate malaria. To date, only experimental, and not natural, human-mosquitohuman transmission has been reported [8]. If natural humanmosquito-human transmission occurred, P. knowlesi could spread more widely in Asia. This is made possible by the wide distribution of at least one vector species, Anopheles latens, in Southeast Asia and in the southern parts of the Indian subcontinent, including the popular tourist areas in western India [10] (Figure 1). It remains to be seen whether this kind of spreading has occurred in the past or will occur in the future, but to date, neither human-mosquito-human transmission nor spreading of P. knowlesi has been documented. SIGNIFICANCE AND FUTURE PROSPECTS Acknowledgments As the number of human P. knowlesi cases increases, clinicians and laboratory personnel should be alerted to this emerging— and potentially lethal—cause of malaria [13, 16]. Laboratory personnel have thus far only been trained to identify the 4 traditional Plasmodium species. Numerous cases in several countries may have been misidentified as being due to P. malariae. Moreover, some malaria RDTs have failed to detect P. knowlesi, and all RDTs fail to identify the species [18,19]. Therefore, if rapid and reliable molecular diagnostic methods are not available to establish the diagnosis of P. knowlesi infection, either ordinary malaria microscopic examination or at least superficial microscopic examination together with RDTs appears to be necessary to diagnose malaria in general in patients infected with P. knowlesi. So far, human P. knowlesi infections have been described in high numbers only in Malaysia. The great majority are from Malaysian Borneo [3, 4, 13, 15], yet numerous cases have also been described in Peninsular Malaysia [9, 13, 14, 23]. Due to the reports of P. knowlesi malaria obtained in the neighboring countries, Thailand [27, 28], Singapore [24–26], Brunei [20], Indonesia [21, 22], Myanmar [29, 30], Vietnam [31], and the Philippines [32, 33], it appears that P. knowlesi is a natural parasite of macaques throughout the Southeast Asian region. The wide distribution of human cases shows that P. knowlesi is generally able to infect humans, which is also suggested by the genetic polymorphism of the P. knowlesi identified from human samples [28]. The fact that P. knowlesi is being identified in increasing numbers now may be attributable in some areas to the reduction of cases of P. falciparum and P. vivax infection, whereas the number of cases of P. knowlesi infection remains constant. The availability and use of specific PCR methods to detect P. knowlesi may generate more reports of P. knowlesi infection, and therefore, the increase in the number of reports is Potential conflicts of interest. All authors: no conflicts. References 1. Coatney G, Collins W, Warren M, Contacos P. CD-ROM: the primate malarias [original book published 1971]. Division of Parasitic Diseases (DPD), ed. Atlanta, GA: Centers for Disease Control and Prevention, 2003. 2. Chin W, Contacos PG, Coatney GR, Kimball HR. A naturally acquited quotidian-type malaria in man transferable to monkeys. Science 1965; 149:865. 3. Fong YL, Cadigan FC, Coatney GR. A presumptive case of naturally occurring Plasmodium knowlesi malaria in man in Malaysia. Trans R Soc Trop Med Hyg 1971; 65:839–40. 4. Singh B, Kim Sung L, Matusop A, et al. A large focus of naturally acquired Plasmodium knowlesi infections in human beings. Lancet 2004; 363:1017–24. 5. Lee KS, Cox-Singh J, Brooke G, Matusop A, Singh B. Plasmodium knowlesi from archival blood films: further evidence that human infections are widely distributed and not newly emergent in Malaysian Borneo. Int J Parasitol 2009; 39:1125–8. 6. Martin MJ, Rayner JC, Gagneux P, Barnwell JW, Varki A. Evolution of human-chimpanzee differences in malaria susceptibility: relationship to human genetic loss of N-glycolylneuraminic acid. Proc Natl Acad Sci U S A 2005; 102:12819–24. 7. Rathore D, Hrstka SC, Sacci JB Jr., et al. Molecular mechanism of host specificity in Plasmodium falciparum infection: role of circumsporozoite protein. J Biol Chem 2003; 278:40905–10. 8. Chin W, Contacos PG, Collins WE, Jeter MH, Alpert E. Experimental mosquito-transmission of Plasmodium knowlesi to man and monkey. Am J Trop Med Hyg 1968; 17:355–8. 9. Vythilingam I, Noorazian YM, Huat TC, et al. Plasmodium knowlesi in humans, macaques and mosquitoes in peninsular Malaysia. Parasit Vectors 2008; 1:26. 10. Cox-Singh J, Singh B. Knowlesi malaria: newly emergent and of public health importance? Trends Parasitol 2008; 24:406–10. 11. Tan CH, Vythilingam I, Matusop A, Chan ST, Singh B. Bionomics of Anopheles latens in Kapit, Sarawak, Malaysian Borneo in relation to the transmission of zoonotic simian malaria parasite Plasmodium knowlesi. Malar J 2008; 7:52. 12. Lee KS, Cox-Singh J, Singh B. Morphological features and differential counts of Plasmodium knowlesi parasites in naturally acquired human infections. Malar J 2009; 8:73. EMERGING INFECTIONS d CID 2011:52 (1 June) d 1361 13. Cox-Singh J, Davis TM, Lee KS, et al. Plasmodium knowlesi malaria in humans is widely distributed and potentially life threatening. Clin Infect Dis 2008; 46:165–71. 14. Lee CE, Adeeba K, Freigang G. Human plasmodium knowlesi infections in Klang Valley, Peninsula Malaysia: a case series. Med J Malaysia 2010; 65:63–5. 15. Daneshvar C, Davis TM, Cox-Singh J, et al. Clinical and laboratory features of human Plasmodium knowlesi infection. Clin Infect Dis 2009; 49:852–60. 16. Cox-Singh J, Hiu J, Lucas SB, et al. Severe malaria - a case of fatal Plasmodium knowlesi infection with post-mortem findings: a case report. Malar J 2010; 9:10. 17. Tang T-HT, Salas A, Ali-Tammam M, et al. First case of detection of Plasmodium knowlesi in Spain by real time PCR in a traveller from Southeast Asia. Malar J 2010; 9:219. 18. Bronner U, Divis PC, Farnert A, Singh B. Swedish traveller with Plasmodium knowlesi malaria after visiting Malaysian Borneo. Malar J 2009; 8:15. 19. van Hellemond JJ, Rutten M, Koelewijn R, et al. Human Plasmodium knowlesi infection detected by rapid diagnostic tests for malaria. Emerg Infect Dis 2009; 15:1478–80. 20. Imported malaria cases, Deaths, United Kingdom: 1990–2009. Vol 2010: Health Protection Agency, 2010. Available at: http://www.hpa.org.uk/ Topics/InfectiousDiseases/InfectionsAZ/Malaria/EpidemiologicalData/ malaEpi10CasesandDeaths/. Accessed 16 March 2011. 21. Sulistyaningsih E, Fitri LE, Loscher T, Berens-Riha N. Diagnostic difficulties with Plasmodium knowlesi infection in humans. Emerg Infect Dis 2010; 16:1033–4. 22. Figtree M, Lee R, Bain L, et al. Plasmodium knowlesi in human, Indonesian Borneo. Emerg Infect Dis 2010; 16:672–4. 23. Kantele A, Marti H, Felger I, Muller D, Jokiranta TS. Monkey malaria in a European traveler returning from Malaysia. Emerg Infect Dis 2008; 14:1434–6. 24. Ng OT, Ooi EE, Lee CC, et al. Naturally acquired human Plasmodium knowlesi infection, Singapore. Emerg Infect Dis 2008; 14:814–6. 25. Ong CW, Lee SY, Koh WH, Ooi EE, Tambyah PA. Monkey malaria in humans: a diagnostic dilemma with conflicting laboratory data. Am J Trop Med Hyg 2009; 80:927–8. 26. Jeslyn WP, Huat TC, Vernon L, et al. Molecular epidemiological investigation of Plasmodium knowlesi in humans and macaques in Singapore. Vector Borne Zoonotic Dis 2010; 11:131–5. 1362 d CID 2011:52 (1 June) d EMERGING INFECTIONS 27. Jongwutiwes S, Putaporntip C, Iwasaki T, Sata T, Kanbara H. Naturally acquired Plasmodium knowlesi malaria in human. Thailand Emerg Infect Dis 2004; 10:2211–3. 28. Putaporntip C, Hongsrimuang T, Seethamchai S, et al. Differential prevalence of Plasmodium infections and cryptic Plasmodium knowlesi malaria in humans in Thailand. J Infect Dis 2009; 199:1143–50. 29. Zhu HM, Li J, Zheng H. Human natural infection of Plasmodium knowlesi [in Chinese]. Zhongguo Ji Sheng Chong Xue Yu Ji Sheng Chong Bing Za Zhi 2006; 24:70–1. 30. Jiang N, Chang Q, Sun X, et al. Co-infections with Plasmodium knowlesi and other malaria parasites, Myanmar Emerg Infect Dis 2010; 16:1476–8. 31. Van den Eede P, Van HN, Van Overmeir C, et al. Human Plasmodium knowlesi infections in young children in central Vietnam. Malar J 2009; 8:249. 32. Luchavez J, Espino F, Curameng P, et al. Human infections with Plasmodium knowlesi, the Philippines. Emerg Infect Dis 2008; 14:811–3. 33. Centers for Disease Control and Prevention. Simian malaria in a U.S. traveler–New York, 2008. MMWR Morb Mortal Wkly Rep 2009; 58:229–32. 34. Van den Eede P, Vythilingam I, Ngo DT, et al. Plasmodium knowlesi malaria in Vietnam: some clarifications. Malar J 2010; 9:20. 35. Barcus MJ, Basri H, Picarima H, et al. Demographic risk factors for severe and fatal vivax and falciparum malaria among hospital admissions in northeastern Indonesian Papua. Am J Trop Med Hyg 2007; 77:984–91. 36. Daneshvar C, Davis TM, Cox-Singh J, et al. Clinical and parasitological response to oral chloroquine and primaquine in uncomplicated human Plasmodium knowlesi infections. Malar J 2010; 9:238. 37. Ohrt C, Purnomo , Sutamihardja MA, Tang D, Kain KC. Impact of microscopy error on estimates of protective efficacy in malariaprevention trials. J Infect Dis 2002; 186:540–6. 38. Babady NE, Sloan LM, Rosenblatt JE, Pritt BS. Detection of Plasmodium knowlesi by real-time polymerase chain reaction. Am J Trop Med Hyg 2009; 81:516–8. 39. Imwong M, Tanomsing N, Pukrittayakamee S, Day NP, White NJ, Snounou G. Spurious amplification of a Plasmodium vivax smallsubunit RNA gene by use of primers currently used to detect P. knowlesi. J Clin Microbiol 2009; 47:4173–5. 40. McCutchan TF, Piper RC, Makler MT. Use of malaria rapid diagnostic test to identify Plasmodium knowlesi infection. Emerg Infect Dis 2008; 14:1750–2.