Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
1398
CIRCULATION
VOL 63, No 6, JUNE 1981
diographic assessment of cardiac anatomy and function in
hypertensive subjects. Circulation 59: 623, 1979
24. Antman EM, Green LH, Grossman W: Physiologic determinants of the electrocardiographic diagnosis of left ventricular hypertrophy. Circulation 60: 386, 1979
25. Dunn RA, Pipberger HV, Holt JH Jr, Barnard ACL, Pipberger
HA: Performance of conventional orthogonal and multipledipole electrocardiograms in estimating left ventricular muscle
21. Bennett DH, Evans DW: Correlation of left ventricular mass
determined by echocardiography with vectorcardiographic and
electrocardiographic voltage measurements. Br Heart J 36:
981, 1974
22. McFarland TM, Mohsin A, Goldstein S, Pickard SD, Stein
PD: Echocardiographic diagnosis of left ventricular hypertrophy. Circulation 57: 1140, 1978
23. Savage DD, Drayer JIM, Henry WL, Mathews EC Jr, Ware
JH, Gardin JM, Cohen ER, Epstein SE, Laragh JH: Echocar-
mass.
Circulation 60: 1350, 1979
Quantitation of Human Left Ventricular Mass
and Volume by Two-dimensional Echocardiography:
In Vitro Anatomic Validation
JOSEPH W. HELAK, M.D.,
AND
NATHANIEL REICHEK, M.D.
Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017
SUMMARY The reliability of two-dimensional echocardiographic (2-DE) quantitation of left ventricular
(LV) section area, volume and myocardial mass was assessed in Vitro in 13 postmortem human hearts (LV
weight 115-454 g). The pathologic diagnoses included: two normal, five coronary artery disease with infarction
and/or aneurysm, three valvular heart disease, two cardiomyopathy and one left ventricular hypertrophy.
Hearts were divided into six to 24 short-axis slices (n = 123), imaged in a tank filled with mineral oil and the
images planimetered. Calibrated photographs-and actual LV weight served as reference standards. Estimates
of section LV cavity volume and myocardial volume were derived by multiplying the appropriate area by section thickness. Section LV mass was obtained by multiplying the myocardial volume by myocardial density.
Total LV cavity volume and myocardial mass were derived using Simpson's rule and a short axis area-apical
length method. In absolute terms, 2-DE underestimated LV cavity area but accurately estimated LV myocardial area. Excellent correlations were obtained between 2-DE and photographic standards for section cavity
area (r = 0.95) and volume (r = 0.90). Simpson's rule (r = 0.97) and area-length (r =- 0.82, r = 0.90, excluding one heart with a bizarrely shaped LV cavity secondary to extensive mural thrombus) estimates of total LV
cavity volume also correlated well with reference standards. Similarly, section LV myocardial area correlated
well with photographic myocardial area (r = 0.89) and 2-DE and photographic estimates of section LV mass
correlated well with actual LV weight (r = 0.92 and 0.96). Consequently, total LV mass obtained with Simpson's rule or the area-length method was highly reliable (r = 0.93 and 0.92, respectively). We conclude that 2DE can provide reliable estimates of LV volume and mass using the short-axis Simpson's rule or area-length
methods and appropriate regression corrections. The area-length method is simple enough to permit clinical
application.
TWO-DIMENSIONAL ECHOCARDIOGRAPHY
(2-DE) is a potentially valuable noninvasive tool for
the quantitative assessment of left ventricular (LV)
volume and myocardial mass in man. Validation
studies of 2-DE in several laboratories have demonFrom the Noninvasive Laboratory, Hospital of the University of
Pennsylvania, and Cardiovascular Section, Department of Medicine, the University of Pennsylvania School of Medicine, Philadelphia, Pennsylvania.
Presented in part at the 29th Annual Scientific Sessions of the
American College of Cardiology, March 1980.
Supported in part by a Southeastern Pennsylvania Heart
Association Research Fellowship grant to Dr. Helak and a Commonwealth of Pennsylvania Health Services contract to Dr.
Reichek.
Dr. Helak's present address: Department of Cardiology, Upstate
Medical Center, East Adams Street, Syracuse, New York 13210.
Address for correspondence: Nathaniel Reichek. M.D., Noninvasive Laboratory, Hospital of the University of Pennsylvania. 3400
Spruce Street, Philadelphia, Pennsylvania 19104.
Received May 19, 1980; revision accepted September 24, 1980.
Circulation 63, No. 6, 1981.
strated the accuracy of in vitro canine LV volume and
mass in symmetric and asymmetric ventricles,1-3 LV
volume determination in a beating dog heart
preparation,4' in vivo canine LV volume and mass,6-10
and in vitro human LV cast volume." Moderately
good correlation of human in vivo 2-DE LV volume
and ejection fraction with angiographic and/or
radionuclide methods has also been reported.8 12-18
However, 2-DE assessments of LV volume and mass
have not been validated directly with quantitative
anatomy in man. The present study was designed to
test the accuracy of 2-DE imaging of individual cardiac sections and of derived estimates of total LV
volume and mass in the postmortem human heart.
Methods
Specimen Collection
Thirteen postmortem human hearts, 300-1100 g,
with a wide range of pathologic diagnoses (table 1)
were obtained from the necropsy service. Nine were
QUANTITATION OF LV MASS AND VOLUME/Helak and Reichek
1399
TABLE 1. Age, Sex, Pathologic Diagnosis and Heart Weight
Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017
Pt
1
Sex
M
2
F
3
F
4
F
5
6
F
M
7
M
8
F
9
10
11
12
13
F
M
M
M
-
Age
Pathologic diagnosis
(years)
Rheumatic heart disease involving mitral valve; pros69
thetic aortic valve; biventricular hypertrophy;
coronary artery disease with old anteroseptal
myocardial infaretion.
74
Coronary artery disease with old anteroseptal and
inferior wall infarctions, apical aneurysm.
56
Concentric left ventricular hypertrophy; coronary
artery disease without infarction.
58
Coronary artery disease with old nontransmural
arterolateral and inferior wall infarctions.
60
Normal
54
Severe three-vessel coronary artery disease with
multiple old transmural and nontransmural
infaretions and an apical aneurysm; right
ventricular hypertrophy.
32
Mitral regurgitation due to myxomatous mitral valve
s/p porcine valve replacement; infarcted posterolateral and posteroseptal regions of left ventricle
due to coronary embolus; large left ventricular
mural thrombus.
72
Coronary artery disease with old infarction posterior
left ventricle and possible acute anteroseptal
63
43
37
66
infarction.
Restrictive cardiomyopathy primary amyloidosis
Congestive cardiomyopathy
Aortic stenosis, biventricular hypertrophy
Normal
Concentric left ventricular hypertrophy
formalin-fixed for 24 hours and hand-sectioned in the
short-axis plane into six to 11 sections (0.5-3 cm
thick) as part of the routine autopsy examination.
Four were specially prepared after formalin fixation,
being embedded in a gelatinous base and sectioned in
the short-axis plane using a motorized slicer set at 0.5
cm thickness producing from 13-24 uniform sections
per heart.
The thickness of each short-axis section was directly
measured at three to five sites with a millimeter rule
and the mean thickness recorded. Because the sections
could not be directly planimetered, the superior and
inferior surfaces of each section were photographed
with a calibration scale on a Xerox copier, model 4000
(fig. 1). Each section was then suspended on an 18gauge needle and a specially designed stand placed in a
glass tank filled with mineral oil. Two-dimensional
echocardiographic images were recorded of each section in a short-axis orientation using a Varian VR
3000 phased-array sector scanner with a 2.25-MHz
transducer. The transducer was handheld, 8-10 cm
from the section. Gain, reject, damping and compression controls were adjusted to produce as complete an
image as possible with the least gain. In general,
overall gain and compression were high, regional
(slide-bar) amplification, contrast and damping low.
Total
heart
weight
(g)
1000
LV
weight
(g)
290
450
171
351
149
700
202
400
720
159
223
1010
454
300
116
850
1100
350
202
293
377
115
254
To obtain adequate images in some instances, two adjacent 0.5-cm sections were sutured together with 3-0
silk suture. To obtain slice thickness by 2-DE, sections
were stacked up from base to apex and images
recorded in a projection analogous to the in vivo
apical view. Strong interfaces were generated between
slices and 50% of each interface thickness was included in each slice thickness, which was traced onto
clear plastic and measured on a digitizer. The thickness of the most superior section of each left ventricle
could not be isolated in this view because of the attached great vessels and atria. Therefore, these 2-DE
thicknesses were interpolated using a regression analysis and measured LV section thickness. The 2-DE
images were recorded on a Sanyo ½/2-inch videotape
recorder.
With the corresponding anatomic specimen as a
reference, LV epicardium and endocardium were
highlighted on each of the photographic images (fig.
2A). Four or five representative, calibrated 2-DE images of each section were traced from videotape onto
clear plastic with a fine-tip pen using real-time, slowmotion and stop-frame analysis and a 12-inch television screen. The LV cavity area excluded all endocardial echoes while the thickness of the finest outer line
of epicardial echoes seen anywhere on the section
1400
CIRCULATION
Vo1 63, No 6, JUNE 1981
Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017
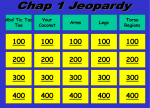
FIGURE 1. Representative short-axis heart section (left) with corresponding calibrated photograph (center)
and two-dimensional echocardiographic image (right).
perimeter was excluded from total LV area throughout the image (fig. 2B). When, occasionally, image
dropout occurred on the lateral margin of the section,
the boundary was extrapolated. The 2-DE images
were traced by blinded observers without knowledge
of other data. Total LV area and LV cavity area were
measured on each photographic and 2-DE image
using a planimetry program validated by comparison
to manual planimetry on irregular test images of
known area and by comparison to calculated area of
circular and rectangular test images of known radius
or linear dimension. Program results were essentially
identical with those of geometric calculation and
manual planimetry. Images were digitized, calculations performed and statistical analysis was made on a
Hewlett-Packard 9025A programmable calculator
equipped with a high-resolution digitizing board
(0.001 mm) and high-speed plotter.
A
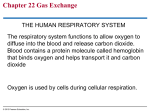
F1GU R 2. (A ) Photographic image shown in figure 1 with endocardium and epicardium of the surface nearest to the camera
outlined. (B) Two-dimensional echocardiographic image shown in figure 1, with total left ventricular (L V) area and L V cavity
area outlined. L V cavity area excludes endocardial echoes, while the thickness of the finest outer line of epicardial echoes seen
anywhere on the scection perimeter is excluded from total L V area throughout the image. The finest lin e of epicardial echoes is
identified bh the arrow.
QUANTITATION OF LV MASS AND VOLUME/Helak and Reichek
Vmuscle
Vcoity
AmT
=
area-length volume was calculated as 5/6 (A pap) L,
where A pap = area at high papillary muscle level and
L = LV length (fig. 4).
-m
V
A
ACT
7rT3
= AT
2
LV Weight
T
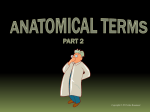
FIGURE 3. Geometric derivation of section volumes from
a single left ventricular slice. V = volume; Am = myocardial area; Ac = cavity area; T= slice thickness.
Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017
For photographic images, the mean of the superior
and inferior surface areas was used to represent the
mean area of each section. For 2-DE images, the
mean of at least four images was used to represent the
section area. Both photographic and 2-DE LV
myocardial areas were determined by subtraction of
LV cavity area from total LV area.
Videotapes of 69 2-DE sections were traced independently by two observers to determine interobserver variation.
Geometric Models
Photographic and 2-DE volumes were determined
for each nonapical section by multiplying the appropriate area (A) (LV myocardium or LV cavity) by
section thickness (T) (fig. 3). The directly measured
section thickness was used to calculate the
photographic volume. Apical section volume was
determined using the formula for an ellipsoidal
volume segment:
rT3
AT
2
6
LV section mass was obtained by multiplying the LV
myocardial volume by the accepted value for density
of myocardium (1.055 g/ml).
Total LV muscle volume and LV cavity volume for
each heart were derived from the 2-DE and photographic images using Simpson's rule. We also tested
an area-length method reported by Wyatt and coworkers to provide accurate LV volume and mass in
the canine left ventricle.7 Simpson's rule merely added
the volume of all sections together (fig. 4), while the
Simpson's Rule
(n-I)
V
=
11
AnT
7rTn3
n
AT
+-
Area Length Method
V= 5/6 APOPL
1401
L
T
Apap
F:-
FIGURE 4. Derivation of total left ventricular myocardial
and cavity volumes using Simpson's rule and short-axis
area-length method. V = volume, n = number of sections;
A = area; T = thickness; AP.P = area at high papillary
muscle level; L = length.
After the photographic and 2-DE images were obtained, the sections were blotted dry, dissected with
removal of the right ventricle, atria, great vessels and
epicardial fat and the LV sections weighed on a triplebeam balance. All section weights were added to
determine total LV weight per specimen.
The specific gravity of portions of four left ventricles weighing 43-79 g was determined by volume
displacement using a 250-ml beaker and 100-ml
graduated cylinder.
Statistics
The 2-DE data, photographic data and LV weights
were compared by standard least-squares linear
regression analysis.
The regression line for each relationship examined
was compared with the line of identity for that
variable using a standard statistical method for comparison of slopes.'9 The regression equations for
Simpson's rule approximations and area-length approximations of the same variable were compared in a
similar manner.
Results
Individual Cardiac Sections
One hundred twenty-three cardiac sections were
studied anatomically, photographically and with 2-DE
to determine LV cavity area and volume and LV
myocardial area and mass as described above.
Section Area and Thickness
The 2-DE LV cavity area showed a close linear correlation with photographic LV cavity area (r = 0.95)
over the range 0-31.5 cm2 (fig. 5A). The least-squares
linear regression equation relating 2-DE LV cavity
area to photographically measured LV cavity area
was A2-DE = 0.76 AphOto-0.1 (SEE = 1.8 cm2). Thus,
in absolute terms, 2-DE markedly underestimated
photographic cavity area.
The 2-DE total LV area also correlated well with
photographic total LV area (r = 0.94) over the range
6.4-85.8 cm2 (fig. 5B). The regression equation relating 2-DE total LV area to photographic total LV area
was A2-DE = 0.96 Aphoto-0.21 (SEE = 6.8 cm2).
The 2-DE LV myocardial area correlated slightly
less well with photographic LV myocardial area
(r = 0.89) (fig. SC). The regression equation relating
2-DE LV myocardial area to photographic LV
myocardial area was myocardial A2-DE = 0.97
myocardial APhoto + 0.98 (SEE = 6.9 cm2 range
6.1-65.4 cm2).
The 2-DE LV section thickness showed a close
linear correlation with actual thickness (r = 0.88) over
VOL 63, No 6, JUNE 1981
CIRCULATION
1402
SECTION LV CAVITY AREA
n-123
r- .E95
S. E. E. -1. 13
so
SECTION LV MYOCARDIAL AREA
90
aS
e30
70
2n
80
E
0
I
IL
X
20
0
50
C-,
C
40
1m
W
n=i23
30
10
r=.
20
5
10
ii
a
0
.'
-0. 120-
y-
a
n1
(i
a
W)
Ri
Ni
-
Y-0.98-.-
V_
PHOTO (cm 2)
0. 70X
0.
ae-
20.97X
c
A
&
&
0.N
m
Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017
94
S.E.E.-6. 8
+
2.00
+
.
1. 50
C
1. 00
40
00
C,-
30
I
20
LIJ
U
50
2.
so
I
1
59
&
S
m0
n1 15
r-. 88
S. E. E. =. 14
r.
70
E
00
n-123
00
(0
m&
SECTION THICKNESS
3.
1 00
0
&
&
PHTO
+PHO TO (cm. )
SECTION TOTAL LV AREA
0
89
S. E.E. =6. 9
0. 50
10
a
N
Y-
-0.
a
a
1t
't
211
0.
9m
a
O
a
0
19
aO
*-
PHOTO (cmi)
ACTUAL
D
B
9
89
0. 13-
0. BSX
Sex
9
ATA
a
hi
19
V)
(Cm. )
t
FiDGURE 5. (A) Comparison of section left ventricular (LV) cavity area by two-dimensional echocardiography (2-DE) (vertical
axis) and by calibratedphotograph (horizontal axis). Regression equation is at lower left. n = number ofslices. (B) Comparison
of section total L V area by 2-DE and by calibrated photograph. (C) Comparison of section L V myocardial area by 2-DE and by
calibrated photograph. (D) Comparison of 2-DE L V section thickness and actual L V section thickness.
(0.3-1.6 cm, fig. 5D). The regression
equation relating 2-DE section thickness to directly
measured thickness was T2-DE = 0.85 T actual ± 0.13
a narrow range
(SEE
= 0. 14 cm).
Section Volume and Mass
absolute terms, 2-DE markedly
weight.
Similarly, photographic section
close correlation (r = 0.96) with
weight over the range 0.3-84 g
overestimated LV
LV mass showed a
actual section LV
(fig. 6B), but the
regression equation relating photographic section LV
directly measured LV section weight was
Mphoto = 1.3 weight + 0.19 (SEE = 6.1 g). Thus, the
photographic method also overestimated LV section
weight. The relationships of 2-DE section LV mass
and photographic section LV mass to actual section
LV weight were not statistically different.
mass to
The 2-DE-section LV cavity volume correlated well
with photographic section LV cavity volume
(r 0.90) over the range 0-63.8 ml. The regression
equation relating 2-DE section LV cavity volume to
photographic section LV cavity volume was V2-DE
=
0.65 Vphoto + 0.56 (SEE = 3.2 ml).
While 2-DE LV section mass correlated well with
actual section LV weight (r 0.92) over the range
0.3-84 g (fig. 6A), the regression equation relating
2-DE section LV mass to directly measured LV weight
Total LV Mass and Volume
=
was M2.DE
=
1.42 weight -1.8 (SEE
=
9.9 g). Thus, in
The 2-DE total LV mass and volume correlated extremely well with total LV weight and photographic
reference standards.
QUANTITATION OF LV MASS AND VOLUME/Helak and Reichek
SECTION LV WEIGHT
A rea-Length Method
1 BCo
140
1 30
100
1210
1 CZ0
0
C 70
n=123
r=0. 92
S. E. E. =9. 9
40
30
20C!
10
G8 68 8
1. 901. 4ZX
A
8
6 a 8
n o hI'
N"
1
y-
88G E8
E
a
N
aUo
M
0
t
a8
0
O
"
(gn.)
ACTUAL
SECTION LV WEIGHT
1 30
Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017
120
110
1 00
90
e0
g
70
m
00
50
cL
n- 123
r=. 96
40
30
S. E. E. =6. 1
20
Area-length estimates of total LV mass and volume
correlated well with reference standards in the 13
study hearts but not as well as Simpson's rule estimates. The 2-DE total LV cavity volume was related
to photographically determined total LV cavity
volume by the equation V2DE = 0.77 VPhOtO + 1.8
(r = 0.82, SEE = 38.4 ml). This relationship was
markedly distorted by one heart (patient 7; table 1)
that contained a large, markedly irregular thrombus
that occupied more than 50% of the LV cavity and
produced a bizarre cavity shape. With this heart excluded, the equation relating area-length 2-DE total
LV cavity volume to photographically determined
total LV cavity volume was V2DE = 1.07 Vphoto
-11.76 (r = 0.90, SEE = 29.0, range 12.4-183.1 ml).
(fig. 8A). The regression equation relating area-length
2-DE total LV mass to photographic total LV mass
was MI-DE = 1.21 MPhOtO -4.61 (r = 0.93, SEE = 71.1
g, range = 146.5-612.6 g) (fig. 8B). This slope did not
differ significantly from unity. In contrast, the equation relating area-length 2-DE total LV mass to actual
total LV weight had a slope much greater than unity:
MI-DE = 1.66 weight -23.83 (r = 0.92, SEE = 74.7 g)
(fig. 8C). Photographically determined area-length
total LV mass showed a similar relationship to actual
total LV weight: MphotO = 1.67 weight -35.86 (r =
0.99, SEE = 29.4 g).
Specific Gravity
10
H
Y-
1403
N
0. 1 9-
m
UD
't
U0
a88s
N
(I
(gm.)
ACTUAL
The specific gravity of the LV myocardium from
hearts in this study determined by volume displacement was 0.964 g/ml.
1. 30X
B
+
FIGLR[ 6.
(A) Comparison of two-dimensional echocardiographic section measurement of left ventricular (LV)
mass (vertical axis) and actual section L V weight (horizontal
axis). (B) Comparison ofphotographic section L V mass and
actual section L V weight.
Simpson's Rule
Thirteen human left ventricles weighing 115-454 g
had photographically determined LV cavity volumes
of 12.4-217.9 ml. The regression equation relating
total 2-DE LV cavity volume to photographically
determined total LV cavity volume was V2-DE = 0.75
Vphoto
-2
(r
=
0.97,
SEE
=
13.9
ml) (fig. 7A).
The re-
gression equation relating 2-DE total LV mass to pho-
tographically determined total LV mass was M2-DE =
1.05 Mphoto -6.1 (r = 0.94, SEE range 180-613 g) (fig.
7B). The regression equation relating 2-DE total LV
mass to actual total LV weight was M2-DE = 1.43
weight -21.8 (r
=
0.93, SEE
=
59.5 g) (fig. 7C). As ex-
pected, photographically determined total LV mass
also correlated well with actual total LV weight
(r = 0.98). The regression equation relating photographic total LV mass to actual total LV weight
M2-DE
=
1.36
weight
-13.3
(SEE
=
26.5
g).
was
Interobserver Variation
Videotapes of 69 2-DE sections from seven hearts
were reviewed and traced independently by two
observers to determine interobserver variation in area
measurement from the same recording. Excellent
linear correlation was obtained for 2-DE section total
LV area (slope = 0.99 r = 0.97, SEE = 4.9 cm2).
Likewise, 2-DE section LV cavity area showed close
linear correlation between observers (slope = 0.90 r =
0.91, SEE = 2.1 cm2). The 2-DE section thickness also
correlated well between observers (r = 0.96,
slope = 0.91, SEE = 0.1 cm). Interobserver variation
in performing the recordings was not assessed.
Discussion
The accuracy of 2-DE assessment of LV volume
and mass has been validated in canine models in
ViVO7-10 and in vitro.1-6 Numerous studies8' 12-18 have
also examined the validity of 2-DE quantitative
assessment of LV volume, LV mass and ejection fraction in man by comparing 2-DE with angiographic
and/or radionuclide methods. Overall, comparing 2DE to angiography, LV end-systolic volume has been
more reliable (r = 0.86-0.96) than either ejection fraction (r = 0.73-0.94) or LV end-diastolic volume (r =
CIRCULATION
1404
VOL 63, No 6, JUNE 1981
SIMPSON'S RULE
SIMPSON'S RULE
225
TOTAL LV CAVITY VOLUME
200
-
650
41
500
175
150
700
n=13
r-. 97
14
sl0
E
TOTAL LV MASS
1
450
+
400
+
S. E. E. =13. 9
125
U)
E
C)'I
1 02
O
75
I
LLI
350
+
300
250
n='3
r=. 94
S. E. E. =54. 7
50
25
50
X
N
Y-
2
u
1\
N
0
04
^0
.4
2
2
N
N
2
N
1. 05X
PHOTO (m 1. )
Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017
700
TOTAL LV WEIGHT
1500
550
500
450
350
U
300
250
n=13
220
r=. 93
S.E. E. =59. 5
150
100
50
a
0
S
S
N
0
N
IX
M
S
t
5
t
U
U
U)
S
a
C
&
G
0
t
a
77
Y- -2413
ACTUAL
C
M
l
0
0
h
t
400
o)
wi
MC)
FIGURE 7. (A) Comparison of Simpson's rule total left
ventricular (L V) cavity volume by two-dimensional echocardiography (2-DE) (vertical axis) and by calibrated
photograph (horizontal axis). (B) Comparison of Simpson's
rule total L V mass by 2-DE and by calibrated photograph.
(C) Comparison of Simpson's rule 2-DE total L V mass and
actual total L V weight.
B50
m
N
PHOTO (gm. )
a
SIMPSON'S RULE
g
N
Y_ - . 13-
-2. 05-
0. 75X
A
a
W
c'
5
In
(gm.)
1. 43x
0.46-0.94). When 2-DE was compared only to biplane
angiography,12' 115 18 the apparent reliability of ejection fraction increased (r = 0.84-0.94) but the
reliability of LV volume estimates was not significantly altered. In a comparison of 2-DE and radionuclide studies to biplane angiography, one study'5
showed no major difference in reliability between 2DE and radionuclide estimates of end-diastolic
volume index, end-systolic volume index or ejection
fraction. However, others have observed a poorer correlation between radionuclide ejection fraction and
angiographic ejection fraction than between 2-DE and
angiographic ejection fraction (2-DE vs angio,
r = 0.94; radionuclide vs angio, r = 0.80).18 Comparisons of 2-DE and radionuclide ejection fractions
have shown correlation coefficients of 0.75 and
0.92. 14,17 Excellent results have been obtained in
canine studies of in vitro and in vivo 2-DE LV mass
,
compared to actual LV weight (r
=
0.86 -0.97).2 8-10
However, comparison of human 2-DE in vivo LV
mass estimates to those of biplane angiography has
given less satisfactory results (r = 0.80).8
Most investigators have concluded that 2-DE ejec-
tion fraction has a close enough correlation with
angiography to allow meaningful clinical application.
However, volume measurements by 2-DE in four
studies'2-14, 18 have underestimated angiographic LV
volume with a large standard error, which limits
clinical applicability. In contrast, one study indicates
that 2-DE can accurately predict angiographic LV
volume.'5 The 2-DE estimation of LV mass has
appeared to have limited clinical applicability.8
This inconsistency in conclusions is not surprising,
given the many variables that must influence the
results reported. A fundamental problem is the inherent limitation of 2-DE image resolution, which is
accentuated by the need to trace images using stopframe analysis, and results in limited accuracy of
boundary identification of endocardium and epicardium. A second problem relates to the many different
geometric formulas for estimating LV volume used in
different studies (table 2). Moreover, even when
similar geometric methods are used, the 2-DE data are
often derived from different 2-DE projections. Finally,
use of angiographic and radionuclide methods to
validate quantitative 2-DE can be misleading because
these methods also indirectly estimate quantitative
anatomy. This was demonstrated by Bommer et al.11
in a recent study comparing angiographic and 2-DE
estimates of LV volume to direct measurements of
LV casts and working LV models in vitro. When
compared to this independent reference system, angiography appeared no more accurate than 2-DE. A
previous report from our laboratory20 comparing Mmode echocardiographic LV mass estimates to
anatomic weight also showed the importance of using
an anatomic reference rather than angiography for
QUANTITATION OF LV MASS AND VOLUME/Helak and Reichek
AREA LENGTH
TOTAL LV MASS
AREA LENGTH
E00
250
TOTAL LV CAVITY VOLUME
1405
700
200
600
500
150
-4
400
E
n=12
r-, 90
S.E.E. =29.6
100
C3
sI
w0
°
U
u
n=13
r-. 93
S. E. E. =71. 1
300
200
1 00
Y-
-
1 . 76-
^4
T4
N
N
y-
PHOTO (m l. )
1. 21X
l. 07X
A
-4. 51-.-
0N
0
0
0
0
In
D
h
09
&
m
U
U
0
(D
PHOTO (,gm. )
B
FIGURE 8. (A) Comparison of area-length total left ventricular (L V) cavity volume by two-dimensional echocardiography (2-DE) (vertical axis) and by calibrated
photograph (horizontal axis). One heart with a large
irregular thrombus occupying greater than 50% of the LV
cavity was excluded from this analysis (see Results). (B)
Comparison of area-length total L V mass by 2-DE and by
calibrated photograph. (C) Comparison of area-length 2-DE
total L V mass and actual total L V weight.
AREA LENGTH
Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017
900
TOTAL LV WEIGHT
700
600
500
al
400
0
I
LIL
300
n=13
92
S. E. E.
200
r=.
=74. 7
100
V-
-23. E331
s
ACTUAL
s
F
@
(gm.)
esesx
C
validation whenever possible. ]In that study, several
echo LV mass methods valiidated previously by
angiography correlated relativetly poorly with actual
LV weight, while the optimal method obtained by
direct comparison to LV weight was far more reliable.
To better define the limitatiorns of the 2-DE method
itself in man, we chose to asset ss the quantitative accuracy of 2-DE imaging of the,area of individual cardiac short-axis sections obtainled from postmortem
human hearts. Short-axis sections were selected
because they generally provide optimal endocardial
imaging, and thus, should have the greatest potential
for accurate quantitation. The 2-DE data were compared to two direct anatomic rteference standards: an
in vitro photographic method 1for sectional LV area
and volume and the actual LV soection weight. Derived
estimates of total LV cavity volume and mass obtained using Simpson's rule and an area-length
method shown7 to be potentiallly clinically applicable
were also compared with the photographic and LV
weight standards. Direct compairison of photographic
and 2-DE image areas permittec assessment of the impact of image properties per se on quantitation.
Conversely, use of the Simpson s rule and area-length
approximation
for
both
2-DE
and
photographic
methods made it possible to assess the impact of the
geometric method independent of a particular image
type. A wide range of pathologic findings, including
myocardial infarction, LV
aneurysm
and
severe
LV
dilation,
present in this series.
Our results show that, in this in vitro system, excellent correlations are obtained between 2-DE and
photographic standards for section LV cavity area and
volume. Thus, Simpson's rule estimates of total LV
cavity volume are also reliable. Area-length estimates
of total LV cavity volume also correlate well with our
reference standard when cavity shape is not bizarrely
distorted. In one heart, a huge irregular thrombus did
markedly affect the area-length volume estimate, but
a second heart (no. 10) with an ordinary apical thrombus was accurately assessed. Moreover, myocardial
infarction (five hearts), LV dilatation (five hearts) or
LV aneurysm (two hearts) did not invalidate the arealength volume estimate. Therefore, this simple arealength method may give reliable results in the common types of LV shape distortion that are clinically
was
encountered. Volume and mass estimates based on
long-axis, four-chamber and two-chamber views,
which include more of the LV perimeter, would
probably deal more effectively with abnormalities of
LV shape than a short-axis area-length method.
However, endocardial identification may not be as
reliable as in short axis. Unfortunately, in the present
study, the sectioning method, which permitted direct
comparison of echo image with original target, also
precluded evaluation of other 2-DE views. The
reliability of 2-DE volume estimates obtained using
VOL 63, No 6, JUNE 1981
CI RCU LATION
1406
TABLE 2. Summary of Geometric Formulas, Two-dimensional Echocardiographic Projections and Reference Methods Used
in Different Studies to Approximate Left Ventricular Volume
Authors
Bommer et al.11
Starling et al.18
2-1) E projections
Biplane, apical
Biplanie, apical
Reference method
GeometXic formiilas
Simpson's ruile
Simpson's ruile
Biplane anigiography
Biplane angiography and
radionuclide niethod
Carr et al.12
Long axis
Short axis
Axial (RAO equi-ivalent)
lleimiaxial (4-chamber)
V
Li L2 L3
6
1-, from image with longest
apparent long axis
L2 from same view as
L,3 from orthogonal view
Biplane angiography anid
silngle-planie angiography
Schiller et al.13
Short axis, mnitral leaflet
tips (equiivalentt to LAO)
Two-chamber apical view (RAO
Simpsoii's rulle
Biplane angiography
Folland et al.14
Short axis, mitral leaflet tips
Short axis, base of pIapillartmuscle
M\odified Simpsoni's ruile
lPlipsoid using biplanie data
Ellipsoid uising sinigle-plane data
Hemisphere-cylinder model
M\lodified ellipsoid model
V _ 4 /3 w L/2 Dr f2 1D 2
Biplane angiography,
radionuclide ventriculograms
equiivalent)
Apical view (4-chamber)
Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017
Chaudry et a116
Quinones et al.17
Short axis, mitral valve tip
apical view (RAO equiivalent)
Measure short axis at base,
mid-LV anld dist al LV in
4-chamber view and
4-chsamb)er
apicalapical
apical R{AO equivalent view
Measuire short axis at base
and mid-LV in long axis
Estimate fractional shortening
of LV long axis from apical
contraction
Abbreviations: IIAO
=
right aniterior obliquie; LAO
Dd2
- ---2 +
1)d2
=
J)D2
left anterior oblique; LV
either method we tested appears to be comparable
statistically to that reported for angiographic methods
in vitro.21' 22 However, in absolute terms, 2-DE underestimates LV cavity volume as compared to Simpson's rule photographic estimates. This suggests that
underestimation is related to the properties of the echo
image. The relatively thick endocardial echo display
probably encroaches on the cavity area. This problem
is compounded in heavily trabeculated areas or those
containing papillary muscle, where fine extensions of
LV cavity may actually be obliterated by thick endocardial echoes. Echo line thickness is gain-dependent,
but images used in this study were all done at the
lowest gain that provided a complete image. Also,
problems of this type may be heavily dependent on the
2-DE instrument used. Validation of quantitation obtained with one type of 2-DE system may not therefore be applicable to others.
Using Simpson's rule, 2-DE reliably predicts actual
LV weight (r = 0.93). Results are similar using the
area-length method (r - 0.92). The reliability of the 2DE estimates of LV mass in this in vitro system is
similar to that noted in a canine in vitro study.2
However, 2-DE LV mass appears to be less accurate
than biplane angiographic LV mass has been reported
to be when compared to LV weight in vitro.21 In absolute terms, 2-DE systematically overestimates LV
weight (slope = 1.43 for Simpson's rule, 1.66 for area-
I)d2 , AL
Single-plane angiography
Single-plane angiographv,
Gated blond pool imaging
left ventricuilar.
length). Similar overestimation occurs when photographic images are used to estimate LV mass with
either Simpson's rule or area-length geometry, so the
major problem is not due to 2-DE imaging. One component of the overestimate is the unexpectedly low
specific gravity of our formalin-fixed, oil-immersed
sections. However, the reduction in specific gravity accounted for only 22% of the mean overestimate of LV
weight. We conclude that most of the LV mass overestimate results from the geometric methods used.
The Simpson's rule approximation, the best available
geometric method, ignores the irregularity of the
trabeculated endocardial surface, which can be
marked in hearts which are fixed at small cavity
volume, and can vary throughout the thickness of even
a thin section of LV. Inclusion of small recesses of the
LV cavity in LV mass probably results. Because postmortem LV volume is often smaller than in vivo enddiastolic volume, this problem may be less important
in vivo. In any event, use of a regression relationship
compensates for the problem.
Because of the many differences between in vitro
and in vivo 2-DE, estimates of in vivo human LV mass
must also be compared to anatomic LV weight, as has
been done with M-mode echocardiography20 and
biplane angiography.23 The 2-DE LV volume methods
evaluated in this study must also be compared with in
vivo angiographic volumes. Moreover, further evalua-
QUANTITATION OF LV MASS AND VOLUME/Helak and Reichek
tion in vitro and in vivo of other geometric approaches
is clearly necessary. However, this quantitative in
vitro study provides a useful basis for such efforts,
demonstrates the limitations of quantitative 2-DE
imaging with present instrumentation, and shows the
potential clinical applicability of a simple short-axis
area-length method to the human left ventricle for
quantitation of both mass and volume.
Acknowledgment
The authors acknowledge the technical assistance of Theodore
Plappert and Ali Muhammad, the assistance of Drs. Eugene
Pearlman and Karl Weber in providing pathologic material, the
secretarial assistance of Patricia Wyatt and the support and encouragement of Dr. John Kastor, Chief of the Cardiovascular Section.
References
Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017
1. Kohn MS, Schapira JN, Beaver WL, Popp RL: In vitro estimation of canine left ventricular volumes by phased array sector
scan. (abstr) Clin Res 26: 244A, 1978
2. Wyatt HL, Heng M, Meerbaum S, Davidson R, Lee SS, Corday E: Quantitative left ventricular analysis in dogs with the
phased array sector scan. (abstr) Circulation 56 (suppl III):
152, 1977
3. Wyatt HL, Heng MK, Meerbaum S, Hestenes J, Davidson R,
Corday E: Quantification of volumes in asymmetric left ventricles by 2-D echocardiography. (abstr) Circulation 57 (suppl
II): 11-188, 1978
4. Eaton LW, Maughan WL, Shoukas AA, Weiss JL: Accurate
volume determination in the isolated ejecting canine left ventricle by two-dimensional echocardiography. Circulation 60: 320,
1979
5. Eaton LW, Maughan WL, Weiss JL: Accurate volume determination in the isolated ejecting canine heart from a limited
number of two-dimensional echocardiographic cross-sections.
(abstr) Am J Cardiol 45: 470, 1980
6. Gueret P, Wyatt HL, Meerbaum S, Corday E: A practical twodimensional echocardiographic model to assess volume in the
ischemic left ventricle. (abstr) Am J Cardiol 45: 471, 1980
7. Wyatt HL, Heng MK, Meerbaum S, Hestenes JD, Cobo JM,
Davidson RM, Corday E: Cross-sectional echocardiography. I.
Analysis of mathematic models for quantifying mass of the left
ventricle in dogs. Circulation 60: 1104, 1979
8. Schiller N, Skioldebrand C, Schiller E, Mavroudis C, Silverman N, Rahimtoola S, Lipton M: In vivo assessment of left
ventricular mass by two-dimensional echocardiography. (abstr)
Circulation 59 (suppl II): 11-18, 1979
9. Salcedo EE, Gockowski K, Tarazi RC: Left ventricular mass
11-
1407
and wall thickness in hypertension. Am J Cardiol 44: 936, 1979
10. Gueret P, Meerbaum S, Wyatt HL, Zwehl W, Corday E:
Determination of left ventricular stroke volume by crosssectional echocardiography. (abstr) Circulation 59 (suppl II):
11-152, 1979
11. Bommer W, Chun T, Kwan OL, Neumann A, Mason DT,
DeMaria AN: Biplane apex echocardiography versus biplane
cineangiography in the assessment of left ventricular volume
and function: validation by direct methods. (abstr) Am J Cardiol 45: 471, 1980
12. Carr KW, Engler RL, Forsythe JR, Johnson AD, Gosink B:
Measurement of left ventricular ejection fraction by mechanical
cross-sectional echocardiography. Circulation 59: 1196, 1979
13. Schiller NB, Acquatella H, Ports TA, Drew D, Goerke J,
Ringertz H, Silverman NH, Brundage B, Botvinick EH,
Boswell R, Carlsson E, Parmley WW: Left ventricular volume
from paired biplane two-dimensional echocardiography. Circulation 60: 547, 1979
14. Folland ED, Parisi AF, Moynihan BS, Jones DR, Feldman CL,
Tow DE: Assessment of left ventricular ejection fraction and
volumes by real-time, two-dimensional echocardiography. Circulation 60: 760, 1979
15. Schiller N, Botvinick E, Cogan J, Greenberg B, Acquatella H,
Glantz S: Noninvasive methods are reliable predictors of contrast angiographic left ventricular volumes. (abstr) Circulation
56 (suppl III): 111-221, 1977
16. Chaudry KR, Ogawa S, Pauletto FS, Hubbard FE, Dreifus LS:
Biplane measurements of left and right ventricular volumes
using wide angle cross-sectional echocardiography (abstr) Am J
Cardiol 41: 391, 1978
17. Quinones MA, Reduto LA, Nelson JG, Ribeiro LG, Young JB,
Winters WL Jr, Miller RR: A new simplified method for determining left ventricular ejection fraction by two-dimensional
echocardiography. (abstr) Circulation 60 (suppl II): 11-153,
1979
18. Starling M, Crawford M, Levi B, Sorenson S, Richards K,
O'Rourke R: Comparative efficacy of cross-sectional echocardiography and gated equilibrium radionuclide angiography for
assessing left ventricular size and performance. (abstr) Am J
Cardiol 45: 403, 1980
19. Dixon WJ, Massey FJ Jr: Introduction to Statistical Analysis.
New York, McGraw-Hill, 1969, p 206
20. Devereux RB, Reichek N: Echocardiographic determination of
left ventricular mass in man: anatomic validation of the
method. Circulation 55: 613, 1977
21. Rackley CE, Dodge HT, Coble YD Jr, Hay RE: A method for
determining'left ventricular mass in man. Circulation 29: 666,
1964
22. Kennedy JW, Reichenbach DD, Baxley WA, Dodge HT: Left
ventricular mass. Am J Cardiol 19: 221, 1967
23. Dodge HT, SandIer HH, Ballew DW, Lord JD Jr: The use of
biplane angiocardiography for the measurement of left ventricular volume in man. Am Heart J 60: 762, 1960
Quantitation of human left ventricular mass and volume by two-dimensional
echocardiography: in vitro anatomic validation.
J W Helak and N Reichek
Downloaded from http://circ.ahajournals.org/ by guest on June 17, 2017
Circulation. 1981;63:1398-1407
doi: 10.1161/01.CIR.63.6.1398
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1981 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is located on
the World Wide Web at:
http://circ.ahajournals.org/content/63/6/1398.citation
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally
published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the
Editorial Office. Once the online version of the published article for which permission is being requested is
located, click Request Permissions in the middle column of the Web page under Services. Further
information about this process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/