Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cardiovascular disease wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Heart failure wikipedia , lookup
Cardiac surgery wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Coronary artery disease wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
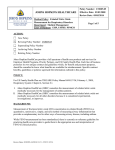
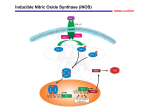
Vascular Endothelial Dysfunction and Mortality Risk in Patients With Chronic Heart Failure Stuart D. Katz, MD; Katarzyna Hryniewicz, MD; Ingrid Hriljac, MD; Kujtim Balidemaj, MD; Clarito Dimayuga, MD; Alhakam Hudaihed, MD; Aleksandr Yasskiy, MD Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Background—Endothelial function is known to be impaired in subjects with chronic heart failure (CHF), but the association between endothelial function and subsequent mortality risk in CHF has not been previously reported. Methods and Results—Biomarkers of endothelial function in the systemic arterial circulation (flow-mediated dilation [FMD] in the brachial artery) and the pulmonary circulation (exhaled nitric oxide [NO] production during submaximal exercise) were prospectively assessed in 259 subjects with New York Heart Association class II–III CHF. In subjects with FMD measurements (n⫽149), there were 12 deaths and 5 urgent transplantations over a median follow-up period of 841 days. In subjects with exhaled NO production measurements (n⫽110), there were 18 deaths and 1 urgent transplantation over a median follow-up period of 396 days. Both decreased FMD and decreased exhaled NO production were associated with increased risk of death or urgent transplantation after adjustment for other known CHF prognostic factors (age, etiology of CHF, functional class, left ventricular ejection fraction) in Cox multivariate proportionalhazards models (adjusted hazard ratio [HR] estimate for a 1% decrease in FMD⫽1.20; 95% confidence interval [CI], 1.03 to 1.45; P⫽0.027; adjusted HR estimate for a 1-ppb/min decrease in exhaled NO production⫽1.31, 95% CI, 1.01 to 1.69, P⫽0.04). Conclusions—Endothelial dysfunction in CHF, as assessed by FMD in the brachial artery and exhaled NO production during submaximal exercise, is associated with an increased mortality risk in subjects with both ischemic and nonischemic CHF. (Circulation. 2005;111:310-314.) Key Words: nitric oxide 䡲 endothelium 䡲 heart failure 䡲 survival E ndothelium-dependent, nitric oxide (NO)–mediated vasodilation in response to hormonal agonists and/or shear stress is decreased in the skeletal muscle, coronary, and pulmonary circulations of patients with chronic heart failure (CHF) when compared with healthy subjects.1–3 Impaired endothelium-dependent vasodilation in patients with CHF is attributable to decreased activity of the L-arginine–NO synthetic pathway, increased degradation of NO by reactive oxygen species, and hyporesponsiveness in vascular smooth muscle.4 – 6 Impaired endothelial function is known to be associated with reduced exercise hyperemia and impaired functional capacity,7,8 but its association with clinical outcomes has not been previously reported. The present study was undertaken to prospectively determine the association of 2 biomarkers of endothelial function, flow-mediated dilation (FMD) in the brachial artery and exhaled NO production during submaximal exercise, and subsequent mortality risk in subjects with CHF. Methods Study Population Two hundred fifty-nine ambulatory subjects with CHF were sequentially recruited in 2 separate cohorts: 149 subjects for determination of FMD measurements and 110 subjects for determination of exhaled NO production during submaximal exercise. Eligible subjects had stable New York Heart Association (NYHA) functional classification II–III symptoms ⱖ3 months and left ventricular ejection fraction ⱕ40%. Patients with exercise-limiting coronary artery disease or peripheral vascular disease, renal disease (serum creatinine ⬎3.0 mg/dL), liver disease (liver enzyme tests ⬎3 times the upper limit of normal), chronic lung disease, or chronic inflammatory diseases were excluded. Background therapy with digoxin, diuretics, angiotensin-converting enzyme inhibitors, nitrates, and/or -adrenergic receptor blockers was discontinued on the morning of testing. Study protocols were approved by the Columbia University and Yale University Ethical Review Committees. All subjects provided written, informed consent before participation. Brachial Artery Ultrasound Imaging Endothelium-dependent, flow-mediated dilation of the brachial artery was determined with high-resolution ultrasound imaging (Ad- Received April 30, 2004; revision received September 15, 2004; accepted September 24, 2004. From the Department of Internal Medicine (S.D.K., K.H., A.H., A.Y.), Yale University School of Medicine, New Haven, Conn, and the Department of Medicine (I.H., K.B., C.D.), Columbia University College of Physicians and Surgeons, New York, NY. Correspondence to Stuart D. Katz, MD, Yale University School of Medicine, 135 College St, Ste 301, New Haven, CT 06510. E-mail [email protected] © 2005 American Heart Association, Inc. Circulation is available at http://www.circulationaha.org DOI: 10.1161/01.CIR.0000153349.77489.CF 310 Katz et al vanced Technology Laboratories) adapted from published guidelines as previously described.9,10 Brachial artery diameter was determined as the mean of 5 measurements from a single cardiac cycle at end-diastole at rest and 60 to 75 seconds after release of a 5-minute forearm cuff occlusion. FMD was calculated as the percent change in brachial artery diameter after forearm cuff release compared with the resting brachial artery diameter. Brachial artery blood flow velocity (cm/s) was determined with a 1.2-mm, pulsed-Doppler sampling volume in the vessel lumen midline with software correction for the incident angle of 60° at rest and for the first 15 seconds after forearm cuff release. The mean blood flow velocity over 5 cardiac cycles is reported. Determination of NO Production in Expired Gases Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Subjects breathed by mouth through a low-resistance, 3-way valve from a 500-L reservoir of NO-free air with a nose clip to exclude nasopharyngeal sources of NO.11 In a preliminary study of 10 CHF subjects, inhalation of aerosolized NG-monomethyl-L-arginine did not alter exhaled NO production when compared with placebo, confirming a lower-airway source for exhaled NO in these patients. NO in expired gases (ppb) was measured with a calibrated chemiluminescent NO analyzer (Sievers model 280). Ventilation (L/min) was simultaneously measured with a calibrated pneumotachometer. NO production (ppb/min) was calculated as the product of the phase-corrected NO concentration and the ventilation signals. Because minute ventilation has been previously reported to influence NO mass transfer from alveoli,11,12 all exhaled NO production measurements were determined at submaximal work rates individually adjusted to correspond to a standardized minute ventilation of 20 L/min. Subjects continued steady-state submaximal exercise at the target work rate for 5 minutes until a plateau in NO production was present. The average exhaled NO production in the last minute of exercise is reported. Patient Outcomes Determination Patient outcomes (death, urgent cardiac transplantation, or no event) were determined for all patients by direct contact with the patient, his/her family, or physician. Subjects of the cohort with exhaled NO production measurements were enrolled between January 1998 and January 1999, and vital status was determined for all subjects of the cohort as of August 1, 1999. Subjects of the cohort with FMD measurements were enrolled between May 2000 and January 2003, and vital status was determined for all subjects of the cohort as of May 16, 2003. Endothelial Function and Mortality in CHF 311 TABLE 1. Clinical Characteristics of 149 Study Subjects in Cohort With FMD Measurements Age, y All Subjects (n⫽149) Survivors (n⫽132) Nonsurvivors (n⫽17) 54⫾1 54⫾1 57⫾3 Sex, % male 84 84 82 Etiology, % ischemic 33 29 65 Class II 51 55 23 Class III 49 45 76 0.25⫾0.01 0.25⫾0.01 0.25⫾0.04 Diabetes 20 17 38 Hypertension 25 24 38 Hyperlipidemia 27 25 44 Never 41 42 34 Past history 48 48 53 Current 11 10 13 100 100 100 55 56 47 NYHA class, % Left ventricular ejection fraction Comorbidities, % Smoking Medications, % RAS inhibitors -Blockers Nitrates 4 2 18 Brachial artery diameter, mm 4.11⫾0.06 4.13⫾0.06 4.03⫾0.15 FMD, % 2.31⫾0.27 2.55⫾0.29 0.47⫾0.60 Rest MBFV, cm/s 6.8⫾0.3 7.0⫾0.4 5.9⫾0.8 Peak MBFV, cm/s 50⫾1.9 51⫾1.2 48⫾4.7 RAS indicates renin-angiotensin system; MBFV, mean blood flow velocity. All other abbreviations are as defined in text. value of 1.79%, subjects with lower values of FMD had significantly more events (n⫽13) than did subjects with higher values of FMD (n⫽4, Figure 1; P⫽0.01, log-rank test). In Cox proportional-hazards models adjusted for other Data Analysis All values are presented as mean⫾SEM. Survival data were analyzed by the Kaplan-Meier method, log-rank tests for univariate analyses, and Cox proportional-hazards models for multivariate analyses (Stata biostatistical software, version 8.0).13 Known prognostic indicators (age, etiology of CHF, NYHA class, left ventricular ejection fraction) were included in all Cox multivariate models. Proportional-hazards assumptions were tested in final models based on analysis of Schoenfeld residuals.14 With an assumed annual event rate of 20%, 1-year accrual with 2-year follow-up, and 2-tailed ␣⫽0.05, the power to detect 2-fold and 3-fold risk differences in groups above and below the median value was 63% and 94%, respectively, for the 110 subjects with exhaled NO production measurements and 76% and 98%, respectively, for the 149 subjects with FMD measurements. For all analyses, a probability value ⬍0.05 was used to infer statistical significance. Results FMD Cohort Clinical characteristics of survivors and nonsurvivors are provided in Table 1. There were 12 deaths and 5 urgent transplantations over a median follow-up period of 841 days. When grouped by FMD responses above or below the median Figure 1. Kaplan-Meier plot showing proportion of survivors over time in subjects with FMD above (dashed line) and below (solid line) median value of 1.79%. Subjects with lower FMD values had more events (n⫽13) than did subjects with higher FMD values (n⫽4; P⫽0.01, by log-rank test). Abbreviations are as defined in text. 312 Circulation January 25, 2005 TABLE 2. Clinical Characteristics of 110 Subjects With Measurements of Exhaled NO Production During Submaximal Exercise Age, y All Subjects (n⫽110) Survivors (n⫽91) Nonsurvivors (n⫽19) 58⫾1 58⫾1 58⫾3 Sex, % male 82 80 89 Etiology, % ischemic 56 53 57 Class II 54 54 53 Class III 46 46 47 0.25⫾0.01 0.25⫾0.01 0.26⫾0.03 Diabetes 34 33 37 Hypertension 35 42 34 Hyperlipidemia 29 29 32 Never 40 41 33 Past history 56 55 61 4 4 7 NYHA class, % Left ventricular ejection fraction Comorbidities, % Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Smoking Current Medications, % 100 100 100 -Blockers RAS inhibitors 56 55 63 Nitrates 19 19 19 4.3⫾0.19 4.5⫾0.22 3.6⫾0.43 21⫾0.6 21⫾0.7 22⫾1.2 Exhaled NO, ppb/min Ventilation, L/min Abbreviations are as defined in text and in the footnote to Table 1. known prognostic factors, decreased FMD remained significantly associated with increased mortality risk when considered as a continuous variable (adjusted hazard ratio [HR] estimate for a 1% decrease in FMD⫽1.20; 95% confidence interval [CI], 1.03 to 1.45; P⫽0.027) or dichotomized at the median value (adjusted HR estimate for below median FMD⫽3.45; 95% CI, 1.10 to 11.1; P⫽0.033). Exhaled NO Production Cohort Clinical characteristics of survivors and nonsurvivors are provided in Table 2. There were 18 deaths and 1 urgent transplantation over a median follow-up period of 396 days. When grouped by exhaled NO production responses above or below the median value of 4.1 ppb/min, subjects with lower values of NO production had more events (n⫽13) than did subjects with higher values of NO production (n⫽6, Figure 2; P⫽0.05 by log-rank test). In Cox proportional-hazards models adjusted for other known prognostic factors, decreased exhaled NO production was significantly associated with increased mortality risk when considered as a continuous variable (adjusted HR estimate for a 1-ppb/min decrease in exhaled NO production⫽1.31; 95% CI, 1.01 to 1.69; P⫽0.04) or dichotomized at the median value (adjusted HR estimate for below median exhaled NO production⫽2.82; 95% CI, 1.04 to 7.63; P⫽0.04). Discussion The present findings demonstrate that impaired vascular endothelial function, as evidenced by decreased FMD in the Figure 2. Kaplan-Meier plot showing proportion of survivors over time in subjects with exhaled NO production above (dashed line) and below (solid line) median value of 4.1 ppb/min. Subjects with lower values of NO production had more events (n⫽13) than did subjects with higher values of NO production (n⫽6; P⫽0.05, by log-rank test). Abbreviations are as defined in text. brachial artery and decreased exhaled NO production during submaximal exercise, is associated with increased mortality risk in CHF subjects after adjustment for other known clinical prognostic factors. Previous experimental and clinical studies have demonstrated impaired endothelium-dependent vasodilation in coronary, skeletal muscle, and pulmonary circulations in patients with CHF.1–3,15,16 In the present study, FMD was used as an indirect biomarker of endothelial function, because this response is partly dependent on shear stress–induced release of NO.17 FMD is also regulated by local prostaglandin production, by the effects of local metabolic conditions on hemoglobin-NO interactions, and by systemic effects related to inflammation, sympathetic activation, and deconditioning.18 –23 The present study design cannot determine which regulatory component(s) of the FMD response might be linked to disease progression in CHF. The relative roles of endothelial cell dysfunction and vascular smooth muscle dysfunction cannot be discerned from our study, because nitroglycerin responses were not recorded. FMD in the brachial artery is closely associated with endotheliumdependent vasomotion in the coronary circulation and is thought to be associated with proinflammatory and prothrombotic changes in endothelial cell phenotype.24 –26 In subjects with ischemic CHF, the association between endothelial dysfunction and mortality could be related to an increased risk of ischemic events, as has been previously described in patients with coronary artery disease and peripheral vascular disease.27 Other mechanisms are also likely contributory, because the observed association between endothelial function and mortality was independent of CHF etiology. Endothelial dysfunction in the coronary microcirculation could contribute to disease progression by inducing local areas of ischemia and/or necrosis.28 Endothelial dysfunction may be also be linked to vasculature-dependent changes in ventricular loading conditions that could promote ventricular remodeling and disease progression.29 Katz et al Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 NO increases in response to exercise in the healthy human and is thought to play an important role in the normal regulation of smooth muscle tone in pulmonary airways and blood vessels.11,30 –33 Experimental and clinical studies have demonstrated that NO may be derived from endothelial, epithelial, and inflammatory cells present throughout the respiratory tract.11,34 –36 Studies in isolated lung preparations and the intact human respiratory tract have demonstrated that a portion of NO in expired gases is derived from the lower respiratory tract, including alveolae.37– 40 Increased exhaled NO production in response to exercise may be attributed to increased shear stress–induced release of NO from alveolar endothelial cells and increased exercise hyperventilationdependent mass transport of NO from alveoli.11,41,42 Airway inflammation may also contribute to exhaled NO production.36,43,44 In patients with CHF, decreased exhaled NO production during exercise is associated with increased pulmonary vascular resistance and decreased maximal aerobic capacity.41,45– 48 Decreased exhaled NO production in patients with CHF may be attributed to decreased diffusion/transport of NO from lower-airway sources and/or a reduced rate of cellular production of NO in the lower respiratory tract.4,40,49 –52 Increased mortality risk in association with decreased exhaled NO production could be related to autonomic dysregulation of ventilation during exercise, progression of right ventricular dysfunction in response to increased pulmonary vascular resistance, or other hemodynamic factors associated with decreased aerobic capacity.41,47,48,53 Interpretation of our findings is potentially limited by several considerations. Although our findings with 2 biomarkers of endothelial function and subsequent mortality risk are internally consistent in our study cohorts, the observational nature of the study does not allow one to draw conclusions regarding a causal link between endothelial dysfunction and mortality, because unmeasured confounders may have contributed to the observed associations. Our study sample was recruited from a tertiary referral heart failure and transplantation center and therefore may not be representative of CHF patients in the general community. The sample size and relatively small number of events limited the number of variables in our regression models and provided sufficient statistical power to detect only large risk differences with wide CIs. Although our reported associations were adjusted for several known prognostic factors, we were unable to adjust our findings for other important prognostic indicators, including left ventricular end-diastolic diameter, peak aerobic capacity, implantable cardioverter-defibrillator use, and biomarkers of neurohormonal activation, because these data were unavailable for all of our subjects. Additional work in a larger study sample is warranted to determine whether endothelial dysfunction is independently associated with mortality after adjustment for these other known prognostic factors. Additional data on the association between endothelial function and cardiovascular disease–specific mortality and major cardiac disease–related morbidities, including nonfatal myocardial infarction and hospitalization for CHF, are also needed. Although discontinued for 12 to 24 hours before all study measurements, background medications may have contributed to our findings. Endothelial Function and Mortality in CHF 313 In conclusion, these data provide the first evidence of an association between markers of endothelial function and subsequent clinical outcomes in patients with CHF. Additional work is needed to determine the underlying mechanisms and potential therapeutic implications of these findings. Acknowledgments This study was supported in part by an American Heart Association (Heritage Affiliate) Grant-In-Aid and NHLBI grants HL K24-04024 (S.D.K.) and HL R01-51433 (S.D.K.). References 1. Katz SD, Biasucci L, Sabba C, Strom JA, Jondeau G, Galvao M, Solomon S, Nikolic SD, Forman R, LeJemtel TH. Impaired endothelium-mediated vasodilation in the peripheral vasculature of patients with congestive heart failure. J Am Coll Cardiol. 1992;19:918 –925. 2. Treasure CB, Vita JA, Cox DA, Fish RD, Gordon JB, Mudge GH, Colucci WS, Sutton MGSJ, Selwyn AP, Alexander RW, Ganz P. Endothelium-dependent dilation of the coronary microvasculature is impaired in dilated cardiomyopathy. Circulation. 1990;81:772–779. 3. Porter TR, Taylor DO, Cycan A, Fields J, Bagley CW, Pandian NG, Mohanty PK. Endothelium-dependent pulmonary artery responses in chronic heart failure: influence of pulmonary hypertension. J Am Coll Cardiol. 1993;22:1418 –1424. 4. Katz SD, Khan T, Zeballos GA, Mathew L, Potharlanka P, Knecht M, Whelan J. Decreased activity of the L-arginine–nitric oxide metabolic pathway in patients with congestive heart failure. Circulation. 1999;99: 2113–2117. 5. Bauersachs J, Bouloumie A, Fraccarollo D, Hu K, Busse R, Ertl G. Endothelial dysfunction in chronic myocardial infarction despite increased vascular endothelial nitric oxide synthase and soluble guanylate cyclase expression: role of enhanced vascular superoxide production. Circulation. 1999;100:292–298. 6. Maguire SM, Nugent AG, McGurk C, Johnston GD, Nicholls DP. Abnormal vascular responses in human chronic cardiac failure are both endothelium dependent and endothelium independent. Heart. 1998;80: 141–145. 7. Katz SD, Krum H, Khan T, Knecht M. Exercise-induced vasodilation in forearm circulation of normal subjects and patients with congestive heart failure: role of endothelium-derived nitric oxide. J Am Coll Cardiol. 1996;28:585–590. 8. Nakamura M, Ishikawa M, Funakoshi T, Hashimoto K, Chiba M, Hiramori K. Attenuated endothelium-dependent peripheral vasodilation and clinical characteristics in patients with chronic heart failure. Am Heart J. 1994;128:1164 –1169. 9. Corretti MC, Anderson TJ, Benjamin EJ, Celermajer D, Charbonneau F, Creager MA, Deanfield J, Drexler H, Gerhard-Herman M, Herrington D, Vallance P, Vita J, Vogel R. Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: a report of the International Brachial Artery Reactivity Task Force. J Am Coll Cardiol. 2002;39:257–265. 10. Katz SD, Balidemaj K, Homma S, Wu H, Wang J, Maybaum S. Acute type 5 phosphodiesterase inhibition with sildenafil enhances flowmediated vasodilation in patients with chronic heart failure. J Am Coll Cardiol. 2000;36:845– 851. 11. Phillips CR, Giraud GD, Holden WE. Exhaled nitric oxide during exercise: site of release and modulation by ventilation and blood flow. J Appl Physiol. 1996;80:1865–1871. 12. Chirpaz-Oddou MF, Favre-Juvin A, Flore P, Eterradossi J, Delaire M, Grimbert F, Therminarias A. Nitric oxide response in exhaled air during an incremental exhaustive exercise. J Appl Physiol. 1997;82:1311–1318. 13. Collet D. Modelling Survival Data in Medical Research. London, England: Chapman & Hall; 1994. 14. Schoenfeld DA. Partial residuals for the proportional hazards regression model. Biometrika. 1982;69:239 –241. 15. Kaiser L, Spickard RC, Olivier NB. Heart failure depresses endotheliumdependent responses in canine femoral artery. Am J Physiol. 1989;256: H962–H967. 16. Wang J, Seyedi N, Xiao-Bin X, Wolin MS, Hintze TH. Defective endothelium-mediated control of coronary circulation in conscious dogs after heart failure. Am J Physiol. 1994;266:H670 –H680. 314 Circulation January 25, 2005 Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 17. Joannides R, Haefeli WE, Linder L, Richard V, Bakkali EH, Thuillez C, Luscher TF. Nitric oxide is responsible for flow-dependent dilatation of human peripheral conduit arteries in vivo. Circulation. 1995;91: 1314 –1319. 18. Hingorani AD, Cross J, Kharbanda RK, Mullen MJ, Bhagat K, Taylor M, Donald AE, Palacios M, Griffin GE, Deanfield JE, MacAllister RJ, Vallance P. Acute systemic inflammation impairs endothelium-dependent dilatation in humans. Circulation. 2000;102:994 –999. 19. Delp MD, Laughlin MH. Regulation of skeletal muscle perfusion during exercise. Acta Physiol Scand. 1998;162:411– 419. 20. Laughlin MH. Endothelium-mediated control of coronary vascular tone after chronic exercise training. Med Sci Sports Exerc. 1995;27: 1135–1144. 21. Sun D, Huang A, Smith CJ, Stackpole CJ, Connetta JA, Shesely EG, Koller A, Kaley G. Enhanced release of prostaglandins contributes to flow-induced arteriolar dilation in eNOS knockout mice. Circ Res. 1999; 85:288 –293. 22. Cosby K, Partovi KS, Crawford JH, Patel RP, Reiter CD, Martyr S, Yang BK, Waclawiw MA, Zalos G, Xu X, Huang KT, Shields H, Kim-Shapiro DB, Schechter AN, Cannon RO 3rd, Gladwin MT. Nitrite reduction to nitric oxide by deoxyhemoglobin vasodilates the human circulation. Nat Med. 2003;9:1498 –1505. 23. Katz SD, Yuen J, Bijou R, LeJemtel TH. Training improves endothelium-dependent vasodilation in resistance vessels of patients with heart failure. J Appl Physiol. 1997;82:1488 –1492. 24. Anderson TJ, Uehata A, Gerhard MD, Meredith IT, Knab S, DeLaGrange D, Lieberman EH, Ganz P, Creager MA, Yeung AC, Selwyn AP. Close relation of endothelial function in the human coronary and peripheral circulations. J Am Coll Cardiol. 1995;26:1235–1241. 25. Ross R. Atherosclerosis—an inflammatory disease. N Engl J Med. 1999; 340:115–126. 26. Libby P. Current concepts of the pathogenesis of the acute coronary syndromes. Circulation. 2001;104:365–372. 27. Mancini GB. Vascular structure versus function: is endothelial dysfunction of independent prognostic importance or not? J Am Coll Cardiol. 2004;43:624 – 628. 28. Canetti M, Akhter MW, Lerman A, Karaalp IS, Zell JA, Singh H, Mehra A, Elkayam U. Evaluation of myocardial blood flow reserve in patients with chronic congestive heart failure due to idiopathic dilated cardiomyopathy. Am J Cardiol. 2003;92:1246 –1249. 29. Nakamura M. Peripheral vascular remodeling in chronic heart failure: clinical relevance and new conceptualization of its mechanisms. J Card Fail. 1999;5:127–138. 30. Matsumoto A, Hirata Y, Momomura S, Fujita H, Yao A, Sata M, Serizawa T. Increased nitric oxide production during exercise. Lancet. 1994;343:849 – 850. 31. Bauer JA, Wald JA, Doran S, Soda D. Endogenous nitric oxide in expired air: effects of acute exercise in humans. Life Sci. 1994;55:1903–1909. 32. Kane DW, Tesauro T, Koizumi T, Gupta R, Newman JH. Exerciseinduced pulmonary vasoconstriction during combined blockade of nitric oxide synthase and -adrenergic receptors. J Clin Invest. 1994;93: 677– 683. 33. Cremona G, Higenbottam TW, Bower EA, Wood AM, Stewart S. Hemodynamic effects of basal and stimulated release of endogenous nitric oxide in isolated human lungs. Circulation. 1999;100:1316 –1321. 34. Shaul PW, North AJ, Wu LC, Wells LB, Brannon TS, Lau KS, Michel T, Margraf LR, Star RA. Endothelial nitric oxide synthase is expressed in cultured human bronchiolar epithelium. J Clin Invest. 1994;94: 2231–2236. 35. Kobzik L, Bredt DS, Lowenstein CJ, Drazen J, Gaston B, Sugarbaker D, Stamler JS. Nitric oxide synthase in human and rat lung: immunocyto- 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. chemical and histochemical localization. Am J Respir Cell Mol Biol. 1993;9:371–377. Barnes PJ. Nitric oxide and airway disease. Ann Med. 1995;27:389 –393. Persson MG, Wiklund NP, Gustafsson LE. Endogenous nitric oxide in single exhalations and the change during exercise. Am Rev Respir Dis. 1993;148:1210 –1214. Kharitonov SA, Chung KF, Evans D, O’Connor BJ, Barnes PJ. Increased exhaled nitric oxide in asthma is mainly derived from the lower respiratory tract. Am J Respir Crit Care Med. 1996;153:1773–1780. Massaro AF, Mehta S, Lilly CM, Kobzik L, Reilly JJ, Drazen JM. Elevated nitric oxide concentrations in isolated lower airway gas of asthmatic subjects. Am J Respir Crit Care Med. 1996;153:1510 –1514. Cremona G, Higenbottam T, Takao M, Hall L, Bower EA. Exhaled nitric oxide in isolated pig lungs. J Appl Physiol. 1995;78:59 – 63. Adachi H, Oshima S, Sakurai S, Toyama T, Hoshizaki H, Taniguchi K, Ito H. Nitric oxide exhalation correlates with ventilatory response to exercise in patients with heart disease. Eur J Heart Fail. 2003;5: 639 – 643. Takahashi M, Ishida T, Traub O, Corson MA, Berk BC. Mechanotransduction in endothelial cells: temporal signaling events in response to shear stress. J Vasc Res. 1997;34:212–219. Chua TP, Lalloo UG, Worsdell MY, Kharitonov S, Chung KF, Coats AJ. Airway and cough responsiveness and exhaled nitric oxide in nonsmoking patients with stable chronic heart failure. Heart. 1996;76: 144 –149. Kharitonov SA, Yates D, Robbins RA, Logan-Sinclair R, Shinebourne EA, Barnes PJ. Increased nitric oxide in exhaled air of asthmatic patients. Lancet. 1994;343:133–135. Adachi H, Nguyen PH, Belardinelli R, Hunter D, Jung T, Wasserman K. Nitric oxide production during exercise in chronic heart failure. Am Heart J. 1997;134:196 –202. Clini E, Volterrani M, Pagani M, Bianchi L, Porta R, Gile LS, Giordano A, Ambrosino N. Endogenous nitric oxide in patients with chronic heart failure (CHF): relation to functional impairment and nitrate-containing therapies. Int J Cardiol. 2000;73:123–130. Hare JM, Nguyen GC, Massaro AF, Drazen JM, Stevenson LW, Colucci WS, Fang JC, Johnson W, Givertz MM, Lucas C. Exhaled nitric oxide: a marker of pulmonary hemodynamics in heart failure. J Am Coll Cardiol. 2002;40:1114 –1119. Sumino H, Sato K, Sakamaki T, Masuda H, Nakamura T, Kanda T, Nagai R. Decreased basal production of nitric oxide in patients with heart disease. Chest. 1998;113:317–322. Cremona G, Higenbottam T, Borland C, Mist B. Mixed expired nitric oxide in primary pulmonary hypertension in relation to lung diffusion capacity. Q J Med. 1994;87:547–551. Hyde RW, Geigel EJ, Olszowka AJ, Krasney JA, Forster RE 2nd, Utell MJ, Frampton MW. Determination of production of nitric oxide by lower airways of humans—theory. J Appl Physiol. 1997;82:1290 –1296. Massaro AF, Drazen JM. Exhaled nitric oxide during exercise: site of release and modulation by ventilation and blood flow. J Appl Physiol. 1996;80:1863–1864. Agnoletti L, Curello S, Bachetti T, Malacarne F, Gaia G, Comini L, Volterrani M, Bonetti P, Parrinello G, Cadei M, Grigolato PG, Ferrari R. Serum from patients with severe heart failure downregulates eNOS and is proapoptotic: role of tumor necrosis factor-␣. Circulation. 1999;100: 1983–1991. Chua TP, Ponikowski P, Harrington D, Anker SD, Webb-Peploe K, Clark AL, Poole-Wilson PA, Coats AJ. Clinical correlates and prognostic significance of the ventilatory response to exercise in chronic heart failure. J Am Coll Cardiol. 1997;29:1585–1590. Vascular Endothelial Dysfunction and Mortality Risk in Patients With Chronic Heart Failure Stuart D. Katz, Katarzyna Hryniewicz, Ingrid Hriljac, Kujtim Balidemaj, Clarito Dimayuga, Alhakam Hudaihed and Aleksandr Yasskiy Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017 Circulation. 2005;111:310-314; originally published online January 17, 2005; doi: 10.1161/01.CIR.0000153349.77489.CF Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2005 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/111/3/310 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/