Survey
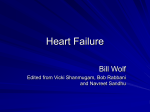
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Management of acute coronary syndrome wikipedia , lookup
Artificial heart valve wikipedia , lookup
Coronary artery disease wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Heart failure wikipedia , lookup
Jatene procedure wikipedia , lookup
Cardiac surgery wikipedia , lookup
Myocardial infarction wikipedia , lookup
Electrocardiography wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Clinical Science (2002) 102, 515–522 (Printed in Great Britain) Left ventricular long-axis changes in early diastole and systole: impact of systolic function on diastole Gabriel W. YIP*, Yan ZHANG*, Peggy Y. TAN†, Mei WANG*, Pik-Yuk HO*, L.-AH . BRODIN‡ and John E. SANDERSON* *Division of Cardiology, Department of Medicine and Therapeutics, The Chinese University of Hong Kong, Prince of Wales Hospital, Shatin, N.T., Hong Kong SAR, China, †Department of Anaesthesia and Intensive Care, The Chinese University of Hong Kong, Prince of Wales Hospital, Shatin, N.T., Hong Kong SAR, China, and ‡Department of Clinical Physiology, Karolinska Institute, Huddinge University Hospital, SE-141 86, Huddinge, Sweden A B S T R A C T Impaired long-axis motion is a sensitive marker of systolic myocardial dysfunction, but no data are available that relate long-axis changes in systole with those in diastole, particularly in subjects with diastolic dysfunction and a ‘ normal ’ left ventricular (LV) ejection fraction. A total of 311 subjects (including 105 normal healthy volunteers) aged 20–89 years with variable degrees of systolic function (LV ejection fraction range 0.15–0.84) and diastolic function were studied using tissue Doppler echocardiography and M-mode echocardiography to determine mean mitral annular amplitude and peak velocity in systole and early and late diastole. The LV systolic mitral annular amplitude (SLAX, where LAX is long-axis amplitude) and peak velocity (Sm) correlated well with the respective early diastolic components (ELAX and Em) and late diastolic (atrial) components (ALAX and Am). A non-linear equation fitted better than a linear relationship (non-linear model : SLAX against ELAX, r2 l 0.67 ; Sm against Em, r2 l 0.60 ; SLAX against ALAX and Sm against Am, r2 l 0.42). After adjusting for age, sex and heart rate, linear relationships of early diastolic (ELAX, r2 l 0.70 ; Em, r2 l 0.60) and late diastolic (ALAX, r2 l 0.61 ; Am, r2 l 0.64) longaxis amplitudes and velocities with the respective values for SLAX and Sm were found, even in those subjects with apparently ‘ isolated ’ diastolic dysfunction. Long-axis changes in systole or diastole did not correlate with Doppler mitral velocities. We conclude that ventricular long-axis changes in early diastole are closely related to systolic function, even in subjects with diastolic dysfunction. ‘ Pure ’ or isolated diastolic dysfunction is uncommon. INTRODUCTION Movement along the left ventricular (LV) long axis is due to longitudinally oriented subendocardial myocardial fibres, and constitutes an important part of global LV performance [1–4]. It was recognized by Hamilton and Romf in 1932 [5] that the heart is relatively fixed with respect to the chest wall ; LV long-axis changes can, therefore, be measured by changes in the position of the atrio–ventricular plane, and the extent of shortening is Key words: early diastole, echocardiography, long-axis function, systolic function. Abbreviations: LV, left ventricular ; LVEF, left ventricular ejection fraction ; ARP, abnormal relaxation pattern in diastole ; DT, deceleration time ; IVRT, isovolumic relaxation time ; LAX, long-axis amplitude ; S , systolic mitral annular displacement ; LAX E , early diastolic mitral annular displacement ; A , late diastolic (atrial) mitral annular displacement ; S , systolic mitral annular LAX LAX m velocity ; E , early diastolic mitral annular velocity ; A , late diastolic (atrial) mitral annular velocity. m m Correspondence : Professor J. E. Sanderson (e-mail jesanderson!cuhk.edu.hk). # 2002 The Biochemical Society and the Medical Research Society 515 516 G. W. Yip and others not modified by changes in the short (minor) axis. Abnormal LV long-axis function has been reported to be an early sign of ischaemia, and occurs in the absence of other major disturbances of global LV performance [6–8]. Changes in the long axis in systole and diastole can be readily quantified by M-mode echocardiography and tissue Doppler echocardiography, which allow the amplitude as well as the velocity of the ring motion to be measured. The mitral annular motion supplements the use of mitral Doppler inflow patterns to assess LV diastolic function, although the concordance between the two is frequently disrupted, especially in various disease states [9–13]. We were interested to determine if disturbances of early diastolic long-axis motion could occur independently of systolic function, i.e. whether ‘ isolated ’ diastolic dysfunction exists, at least in the long axis. We reasoned that this was unlikely, because LV recoil in early diastole, which creates the ‘ suction ’ effect, is dependent on the stored energy from the previous systole, and this is a major contribution to filling of the ventricle in the normal heart. Impaired contraction of the left ventricle during systole will lead to reduced recoil and suction, and therefore reduced early diastolic filling. Changes in ventricular compliance will affect function more at end-diastole, changing the pressure–volume relationship, rather than during early diastolic filling. We investigated this hypothesis using spectral tissue Doppler imaging, which is capable of high temporal resolution, to measure apically directed myocardial velocities during diastole, which were then related to the annular amplitude and velocity in systole and other standard measurements of global ejection fraction, in a large group of subjects with a wide range of LV systolic function and diastolic dysfunction. These results were presented in part at the XXI Congress of the European Society of Cardiology, Barcelona, Spain, on 29 August 1999. METHODS Study subjects A total of 311 subjects (156 females and 155 males) aged between 20 and 89 years (mean age 59.4 years) were recruited, comprising 105 normal healthy volunteers (mean age 47.6 years ; range 20–84 years) and 206 patients with a wide range of values for LV ejection fraction (LVEF) (mean 0.56 ; range 0.12–0.84). The healthy volunteers had no history of cardiovascular symptoms, or of hypertension, diabetes mellitus, hypercholesterolaemia or peripheral vascular disease, and had normal findings on two-dimensional echocardiography. All subjects had normal sinus rhythm without bundle branch block or significant valvular or pericardial disease. The # 2002 The Biochemical Society and the Medical Research Society Table 1 Major disease entities in 206 patients Abbreviations : MI, myocardial infarction ; CVA, cerebral vascular accident ; TIA, transient ischaemic attack ; PVD, peripheral vascular disease. Prevalence Disease No. % Hypertension Coronary artery disease Diabetes mellitus Dilated cardiomyopathy History of previous MI Previous history of CVA, TIA or PVD Paroxysmal atrial fibrillation End-stage renal failure 82 47 47 30 29 12 10 2 39.8 22.8 22.8 14.6 14.1 5.8 4.9 1.0 remaining 206 subjects had a variety of cardiac diseases (Table 1). Recording of echocardiograms Echocardiograms were obtained using GE-VingMed System 5 echocardiographic equipment (GE-VingMed Sound AB, Horten, Norway) and a 3.5 mHz multiphase-array probe. Subjects lay in the left lateral decubitus position. Echocardiographic techniques and calculations of the various cardiac dimensions were performed according to the recommendations of the American Society of Echocardiography [14–17]. Doppler mitral inflow velocities at the tip of the mitral leaflets were recorded in the LV apical four-chamber view. Diastolic parameters were measured for at least three beats. These parameters included peak early mitral valve filling velocity (E wave), peak atrial filling velocity (A wave), E\A ratio and deceleration time (DT). The isovolumic relaxation time (IVRT) was measured by pulsewave Doppler sampled between the anterior mitral leaflet and the LV outflow tract [18]. The LV diastolic mitral flow pattern was characterized as a normal pattern, an abnormal relaxation pattern (ARP), a pseudonormal pattern or a restrictive filling pattern, as described previously [19–21]. An ARP was characterized by a prolonged DT ( 240 ms), a reversed E\A ratio and a prolonged IVRT ( 100 ms). A restrictive filling pattern was characterized by a short DT ( 140 ms), a large E\A ratio ( 2) and a short IVRT ( 70 ms). A pseudonormal pattern was defined by a relatively normal DT (140–240 ms), a reversed pulmonary venous flow pattern with predominant systolic forward rather than diastolic flow, and a pulmonary venous atrial reversal wave duration that is 30 ms longer than the mitral A wave [22]. The diastolic flow patterns give a fair estimation of increasing LV filling pressures in the presence of a stiffer left ventricle. The ARP is seen early with impaired LV relaxation, and is recognized by a decrease in early Left ventricular long axis in diastole and systole Table 2 Baseline echocardiographic characteristics of the 105 normal subjects and of the total study population of 311 subjects LVEF(2D), LVEF measured by the two-dimensional modified Simpson’s method ; LVEF(avpd), LVEF measured by the atrio–ventricular plane method ; LVEDd, LV end-diastolic diameter ; FS, fractional shortening. Normal subjects (n l 105) Total population (n l 311) Parameter Mean S.D. S.E.M. Minimum Maximum Mean S.D. S.E.M. Minimum Maximum Age (years) Heart rate (beats/min) LVEF LVEF (avpd) LVEDd (cm) SLAX (cm) ELAX (cm) Sm (cm/s) Em (cm/s) FS 47.13 71.68 0.69 0.71 4.54 1.37 0.87 6.54 8.34 0.36 14.52 10.17 0.06 0.08 0.50 0.14 0.18 1.00 2.06 0.05 1.41 1.12 0.01 0.01 0.05 0.01 0.02 0.10 0.21 0.01 20 53 0.54 0.53 3.48 1.05 0.49 4.73 4.57 0.26 84 109 0.84 0.90 5.45 1.74 1.33 9.24 12.83 0.50 59.45 72.10 0.56 0.57 4.90 1.13 0.67 5.15 5.76 0.29 16.54 13.61 0.17 0.18 0.93 0.32 0.23 1.79 2.81 0.11 0.94 0.93 0.01 0.01 0.06 0.02 0.01 0.10 0.16 0.01 20 45 0.12 0.13 2.90 0.33 0.18 1.08 0.73 0.05 89 115 0.84 0.90 9.26 1.74 1.33 9.24 12.83 0.53 transmitral LV filling (E wave) and an increased proportion of filling during atrial contraction (A wave). As the left ventricle becomes less compliant and the LV filling pressure is high, the pseudonormal pattern is seen with a relatively normalized DT. With further decrease in LV compliance, LV filling has restrictive features characterized by rapid early filling with high filling pressures, very little atrial contribution and a poor prognosis. The mean mitral annular displacement in systole (SLAX,where LAX is long-axis amplitude), early diastole (ELAX) and late diastole due to atrial contraction (ALAX) were obtained by M-mode echocardiography, by placing a cursor at the septal, lateral, anterior and inferior aspects of the mitral annulus in the apical view. Similarly, pulsed-wave tissue Doppler echocardiography was performed with the same machine with a sample volume located at four different positions of the mitral annulus. Mean peak systolic (Sm), peak early diastolic (Em) and late diastolic (atrial contraction) (Am) mitral annular velocities were obtained. All images were acquired during end-expiration. Attention was given to ensuring appropriate velocity range settings (high enough pulse repetition frequency) to avoid aliasing within the tissue Doppler images. Each measurement of mitral annular motion was recorded for three cardiac cycles, and corresponding mean measurements were analysed with an off-line Microsoft NT workstation. LVEF was obtained using a modified biplane Simpson method from apical two- and four-chamber views, and also by using the atrio–ventricular plane displacement method described by Willenheimer et al. [23]. Statistical analysis Velocity, amplitude and timing comparisons were made among all three types of recording of mitral Doppler inflow patterns and longitudinal mitral annular amplitudes and velocities in the same patient. The mitral inflow velocity indices and the mitral ring excursions and velocities in whole cardiac cycle were also related to the LVEF. The means were compared using Student’s t test or ANOVA as appropriate. r# values were calculated using multiple linear regression for a linear relationship and the non-linear regression method for an exponential relationship. Inter- and intra-observer reliability were obtained for analysis of the above parameters using results from 30 randomly chosen patients by inter- and intra-class correlation and the Bland–Altman methods [24]. The acquired images were analysed independently by two blinded observers to obtain the inter-observer reliability. These calculations were made using the statistical package SPSS for Windows, version 9.0 (SPSS Inc.) for IBMcompatible computers. A P value of 0.05 was taken as significant. Results are given as meanspS.E.M. RESULTS Baseline characteristics Table 2 summarizes the clinical, Doppler, M-mode echocardiographic, tissue Doppler and haemodynamic parameters for all subjects. The range of LVEF values varied from 0.18 to 0.88. Heart rate averaged 72.1p 0.9 beats\min. There was no significant difference in ages between males and females in the whole cohort (males, 57.48p16.61 years ; females, 57.87p1.44 years ; P l 0.85). The mean LV end-diastolic diameter increased progressively with worsening diastolic mitral inflow patterns and LVEF (Table 3). There was a good correlation between LVEF measured by the modified Simpson’s two-dimensional method and by the atrio– # 2002 The Biochemical Society and the Medical Research Society 517 G. W. Yip and others Table 3 Distribution of age, sex and LV end-diastolic dimension (LVEDd) of 311 subjects by Doppler mitral inflow pattern RFP, restrictive filling pattern ; PN, pseudonormal pattern. Values for age and LVEDd are meanspS.E.M. The LVEDd for healthy controls and patients with a normal inflow pattern was obtained by combining data for these two groups. Patients No. of subjects Sex Female Male Age (years) LVEDd (cm) Healthy controls Normal pattern ARP PN RFP Overall 105 (33.7 %) 30 (9.6 %) 126 (40.5 %) 23 (7.4 %) 27 (8.7 %) 311 7 (4.5 %) 16 (10.3 %) 63.57p2.41 5.83p0.25 11 (7.1 %) 16 (10.3 %) 59.00p2.81 5.97p0.20 156 155 59.40p0.94 4.90p0.06 65 (41.6 %) 40 (25.8 %) 47.13p1.41 4.66p0.06 15 (9.6 %) 15 (9.7 %) 65.30p2.34 4.66p0.06 58 (37.2 %) 68 (43.9 %) 67.54p1.26 4.86p0.11 Table 4 Corrected r 2 values for different types of regression analyses Slax Regression analysis was performed (a) for the relationships of SLAX with ELAX and ALAX, and (b) for the relationships of Sm with Em and Am in 311 subjects, with and without adjustment for age, heart rate and sex. Non-linear regression is in form a[1kexp(bX )], where X is the independent variable ; a and b are constants. (a) r 2 versus SLAX Elax ELAX ALAX Linear regression without constant Non-linear regression Without adjustment With adjustment Without adjustment With adjustment 0.5086 0.2955 0.6898 0.6076 0.6706 0.4160 0.6973 0.6125 (b) r 2 versus Sm Sm 518 Em Am Linear regression without constant Non-linear regression Without adjustment With adjustment Without adjustment With adjustment 0.2470 0.3411 0.5787 0.6377 0.5983 0.4194 0.5992 0.6380 Em Figure 1 Linear and non-linear correlations between SLAX and ELAX (upper panel) and Sm and Em (lower panel) without correction for age, sex and heart rate ventricular plane displacement method (r# l 0.82, P 0.001). origin moderately with ALAX (r# l 0.42). When corrected for age, sex and heart rate, similar but linear correlations of ELAX (r# l 0.70) and ALAX (r# l 0.61) with SLAX were observed (Table 4a). Relationships between systolic and diastolic LAX values Relationships between systolic and diastolic velocities (tissue Doppler echocardiography) In M-mode long-axis measurements, SLAX was correlated through the origin well in a non-linear fashion with ELAX (r# l 0.67) (Figure 1, upper panel), and through the Sm was correlated non-linearly through the origin with Em (r# l 0.60) (Figure 1, lower panel) and Am (r# l 0.42). When corrected for age, sex and heart rate, similar but # 2002 The Biochemical Society and the Medical Research Society Left ventricular long axis in diastole and systole Table 5 Relationships between parameters of mitral ring motion and heart rate or LV end-diastolic diameter (LVEDd) r 2 values were obtained by linear regression. Table 7 Normal ranges for mitral annular amplitude and velocity measurements in different age groups of adult Chinese DTLAX, deceleration time of ELAX ; IVRTm, IVRT in mitral annular velocity. r2 ELAX ALAX Sm Em Am 0.0003 0.0053 0.0090 0.0089 0.1054 0.0099 0.1376 0.0382 0.0161 0.0074 0.2359 0.0032 SLAX (cm) 30 31–50 50 Overall 1.48 1.40 1.30 1.37 0.09 0.15 0.10 0.14 0.03 0.02 0.02 0.01 (1.42, 1.54) (1.36, 1.44) (1.27, 1.33) (1.35, 1.40) linear correlations of Em (r# l 0.60) and Am (r# l 0.64) with Sm were observed (Table 4b). ELAX (cm) 30 31–50 50 Overall 1.08 0.90 0.75 0.87 0.12 0.15 0.14 0.18 0.03 0.02 0.02 0.02 (1.00, 1.15) (0.86, 0.95) (0.70, 0.79) (0.83, 0.90) ALAX (cm) 30 31–50 50 Overall 0.45 0.53 0.55 0.53 0.05 0.08 0.07 0.08 0.02 0.01 0.01 0.01 (0.41, 0.48) (0.51, 0.55) (0.53, 0.58) (0.51, 0.54) DTLAX (s) 30 31–50 50 Overall 0.11 0.12 0.12 0.12 0.016 0.013 0.012 0.014 0.004 0.002 0.002 0.001 (0.10, 0.12) (0.12, 0.12) (0.12, 0.13) (0.12, 0.12) Sm (cm/s) 30 31–50 50 Overall 7.28 6.73 5.93 6.50 0.53 1.06 0.91 1.06 0.15 0.15 0.15 0.11 (6.95, 7.61) (6.44, 7.03) (5.63, 6.23) (6.29, 6.71) Em (cm/s) 30 31–50 50 Overall 10.77 8.88 6.76 8.32 1.09 1.69 1.65 2.09 0.32 0.24 0.27 0.21 (10.08, 11.47) (8.41, 9.36) (6.21, 7.31) (7.91, 8.74) Am (cm/s) 30 31–50 50 Overall 6.11 7.45 7.80 7.42 1.18 1.31 1.44 1.43 0.34 0.18 0.24 0.14 (5.36, 6.86) (7.08, 7.82) (7.32, 8.28) (7.14, 7.70) IVRTm (s) 30 31–50 50 Overall 55.50 66.15 72.10 67.07 9.63 12.37 16.42 14.55 2.78 1.73 2.70 1.46 (49.38, 61.62) (62.67, 69.63) (66.62, 77.57) (64.18, 69.96) Heart rate LVEDd Relationships between mitral inflow velocities and LV long-axis variables (Table 3) Neither LV long-axis velocities nor amplitudes correlated with their corresponding Doppler mitral inflow indices. Approx. 85 % of patients were diagnosed with diastolic dysfunction based on mitral inflow velocities and pulmonary vein patterns, as described above. The majority (61 %) had an ARP with LVEF 0.45, i.e. within the ‘ normal ’ range. However, the relationship between systolic and diastolic long-axis measurements (amplitude and velocities) still held in this group, who therefore were characterized by diastolic dysfunction and a ‘ normal ’ LVEF. Age group (years) Relationships between mitral ring motion and age in healthy adults Systolic and early diastolic mitral ring motion decreased and late diastolic ring motion increased with advancing age, but not with increasing heart rate or LV enddiastolic dimension ; gender had no effect (Table 5). The age-related changes in the mitral annular parameters between 20 and 84 years of age were calculated from linear regression equations, and are shown in Table 6. The normal ranges of these parameters in adult Chinese are shown in Table 7. Table 6 Mean S.D. S.E.M. 95 % Confidence interval for mean SLAX Changes between 20 and 84 years of age for some LV dimensions calculated from linear regression equations Change between 20 and 84 years Parameter Expected at age 20 Expected at age 84 Absolute % Linear correlation with age (r ) SLAX (cm) Sm (cm/s) ELAX (cm) Em (cm/s) ALAX (cm) Am (cm/s) 1.49 7.48 1.09 10.99 0.48 6.57 1.22 5.22 0.56 4.82 0.60 8.53 k0.28 k2.26 k0.53 k6.17 0.12 1.96 k18 k30 k49 k56 25 30 k0.44 k0.49 k0.67 k0.67 0.35 0.31 P value 0.001 0.001 0.001 0.001 0.001 0.002 # 2002 The Biochemical Society and the Medical Research Society 519 520 G. W. Yip and others Reliability of mitral annular displacement and velocity measurements The intra-class correlations for various mitral annular motion parameters by the same observer were between 0.8 and 0.9. The inter-observer correlations for same parameters were between 0.7 and 0.9. Using the Bland– Altman method, the mean difference between observations was 5 % of the mean value of the observations for measurements of amplitude, duration and velocity. DISCUSSION Our results support a close link between contraction and relaxation, especially during early diastole. They illustrate that the heart, as a muscular pump, functions in the same way as an isolated cardiac muscle ; a decrease in the force of shortening and re-lengthening during relaxation of an afterloaded twitch are parts of one activity cycle, i.e. part of one contraction–relaxation cycle (or ‘ systole ’) [25]. Both experimental and clinical studies suggest that the normal left ventricle contracts to a volume less than its equilibrium volume, hence compressing elastic cardiac elements, which creates early diastole-restoring forces that produce a ‘ suction ’ effect that lowers LV minimal pressure and increases early filling [26]. Active relaxation is an important component, like its systolic counterpart contraction ; it is an active, energy (ATP)-dependent process that depends on systolic and diastolic loads, the non-uniformity of the load, and the passive elastic characteristics of the ventricle. However, the restoring forces (among other factors), stored as potential energy generated during contraction, also influence diastolic relaxation. These restoring forces are related to the amount of systolic deformation. Of course, it is impossible from the results of the present study to determine the relative contributions of active relaxation and elastic recoil to early diastolic filling. It is likely that both are dependent on the extent of systolic function. In disease states, LV filling is generated predominantly by the increased pressure gradient from the left atrium to the left ventricle due to increased left atrial pressure and also stiffness, rather than by LV elastic recoil and active relaxation. This explains the discordance between the long-axis and mitral inflow velocities ; the former reflects systolic function, while the latter reflects the left atrium– left ventricle pressure gradient. In our study, a non-linear equation fitted better than a linear one for both long-axis amplitudes and velocities. However, when corrected for age, sex and heart rate, a linear relationship was seen. Furthermore, the fact that heart rate had little influence on long-axis mitral annular velocities indicates that myocardial velocities are less dependent on preload, as suggested by previous studies [4–10]. Short-axis shortening, as reflected by fractional shortening, does not # 2002 The Biochemical Society and the Medical Research Society compensate fully for the long-axis change in patients with declining LVEF. Our results also provide an explanation for observations from previous studies, which have used tissue Doppler echocardiography to differentiate restrictive cardiomyopathy from constrictive pericarditis [8,9], and normal from pseudonormal Doppler mitral inflow patterns [10]. The differences are in fact related to the degree of systolic LV dysfunction rather than to individual absolute myocardial velocities. Patients with restrictive cardiomyopathy tend to have poorer (albeit within the ‘ normal ’ range) systolic function, as do those with a pseudonormal diastolic mitral pattern. The most common cause of a decrease in the early diastolic lengthening rate is a low overall amplitude of the ring motion, which is characteristic of systolic LV disease [13]. Our results also question the notion of ‘ diastolic ’ heart failure. It appears unlikely that a pure abnormality of diastolic function will exist, or alternatively that the majority of those with abnormal filling will also have some degree of systolic dysfunction that can be detected by analysing the long axis, but not the LVEF. This distinction is important, as diastolic heart failure is the commonest form of heart failure in many communities [27,28]. Clearly, the total excursion of the mitral valve annulus during systole must equal that which occurs in diastole, as the mitral valve ring returns to the same position with every beat. However, this does not hold for the velocities or for the relative balance between early and late diastole. The degree of motion during atrial systole will depend both on the extent of the excursion during ventricular systole, which stretches the pectinate muscles, and the amount of movement during early diastole. The balance between early diastolic and late diastolic amplitudes and velocities will vary with different disease states and with the strength of systolic function. In addition, the effect of atrial systole is to draw the mitral valve ring around the blood in the atrium, which is thereby transferred into the ventricle. In contrast, during systole the movement of the mitral valve ring downwards will increase the atrial volume, creating a suction effect, which draws blood from the pulmonary veins [29]. Thus atrial filling is also dependent on ventricular systolic function. Indeed, in our study there was a correlation between the systolic component and the atrial component of mitral ring motion. Age has a marked effect on the balance between early and late diastolic filling. Previous studies have shown that LVEF at rest in adults is unchanged or increased slightly with advancing age [30–32]. However, the long axis, as reflected by mitral ring motion, decreases by up to 20 %, whereas the short axis increases by up to 18 %, with increasing age in normal adults [33]. These changes are independent of systolic blood pressure, LV wall thickness, heart rate or sex. Our study showed similar results, with decreases of approx. 18 % in SLAX and 30 % in Sm. A Left ventricular long axis in diastole and systole similar diminution was seen in the early diastolic motion, with 49 % and 56 % decreases in ELAX and Em respectively, but with an increase in the atrial component of mitral ring motion (25–30 %). Study limitations All previous known limitations of Doppler echocardiography will apply to the present study. These include the following. (1) Tissue Doppler echocardiography measures myocardial velocity relative to the ultrasound beam. Thus the smaller the angle between the Doppler beam and the incident surface, the greater the accuracy of the velocity measurement that is obtained. Further, the direction of movement measured in the present study was longitudinal from the base towards the LV apex, the latter being relatively fixed throughout the cardiac cycle [23]. (2) The velocity data acquired with colour Doppler echocardiography are mean velocities. They are only slightly different from temporal data obtained over several cycles. The mean velocities have the additional advantage of reducing the noise effect during measurement. The noise effect is reduced further by taking an average of multiple measurement of a similar heart rate. (3) Artefacts caused by thickening, translational motion of the heart, and motion caused by breathing are inevitably present. Breathing artefacts can be minimized by image acquisition during expiration. The issue of translational movement is still unresolved. The Doppler sample site was fixed and did not track the myocardium being sampled, and hence the same portion of the myocardium was not sampled throughout the cardiac cycle. However, as the sampled myocardium moved up to just more than 10 mm, it is very likely that the adjoining myocardium sampled at different parts of the cardiac cycle with a fixed sample volume would move at similar velocities, especially in the longitudinal direction. Although the healthy volunteers included in the present study had no evidence of cardiac disease, a small possibility of incipient subclinical myocardial or coronary ischaemia in this control population cannot be excluded. The heart rates of the whole group were fairly constant (mean 72.6p1.1 beats\min), and the effect of heart rate on the measurements was minimal. However, the effect of loading conditions on myocardial velocities has not been addressed in this within-patient study, as comparisons were made using instantaneous recordings. ated predominantly by the increased left atrium–left ventricle pressure gradient due to increased left atrial pressure and also stiffness, rather than by LV elastic recoil and active relaxation. Early diastolic function is therefore tightly coupled to the previous systole, even in those subjects with an apparently normal LVEF and evidence of diastolic dysfunction from Doppler mitral flow studies. Isolated early diastolic dysfunction in the presence of truly normal systolic function is probably very rare. ACKNOWLEDGMENTS This research was funded by a Direct Grant for Research, Faculty of Medicine, Chinese University of Hong Kong, Hong Kong SAR, China. We thank Dr Derek Gibson for his help and advice, and we are grateful to Mr K. K. Wong, Centre for Clinical Trials and Epidemiological Research, Chinese University of Hong Kong, for statistical advice and helpful assistance. REFERENCES 1 2 3 4 5 6 7 8 9 Conclusions Analysis of long-axis excursion provides different information from Doppler mitral inflow velocities. The LV long-axis change in early filling correlates strongly with LV systolic function. In disease states, the discordance between the long-axis parameters and the Doppler mitral inflow indices becomes apparent, as LV filling is gener- 10 Henein, M. Y. and Gibson, D. G. (1999) Normal long axis function. Heart 81, 111–113 Jones, C. J. H., Raposo, L. and Gibson, D. G. (1990) Functional importance of the long axis dynamics of the human left ventricle. Br. Heart J. 63, 215–220 Simonson, J. S. and Schiller, N. B. (1989) Descent of the base of the left ventricle : an echocardiographic index of left ventricular function. J. Am. Soc. Echocardiogr. 2, 25–35 Pai, R. G., Bodenheimer, M. M., Pai, S. M., Koss, J. H. and Adamick, R. (1991) Usefulness of systolic excursion of the mitral annulus as an index of left ventricular systolic function. Am. J. Cardiol. 67, 222–224 Hamilton, W. F. and Romf, J. H. (1932) Movements of the base of the ventricle and the relative constancy of the cardiac volume. Am. J. Physiol. 102, 559–565 Henein, M. Y., Priestly, K., Davarshvili, T., Buller, N. and Gibson, D. G. (1993) Improved left ventricular subendocardial function following successful coronary angioplasty. Br. Heart J. 69, 501–506 Henein, M. Y., Rosano, G. M. C., Underwood, R., Poole-Wilson, P. A. and Gibson, D. G. (1994) Relations between resting ventricular long axis function, the electrocardiogram, and myocardial perfusion imaging in syndrome X. Br. Heart J. 71, 541–547 Garcia, M. J., Rodriguez, L., Ares, M. A., Griffin, B. P., Thomas, J. D. and Klein, A. L. (1996) Differentiation of constrictive pericarditis from restrictive cardiomyopathy : assessment of left ventricular diastolic velocities in the longitudinal axis by Doppler tissue imaging. J. Am. Coll. Cardiol. 27, 108–114 Rajagopalan, N., Garcia, M. J., Rodriguez, L., Murray, R. D. and Klein, A. L. (1998) Comparison of Doppler echocardiographic methods to differentiate constrictive pericarditis from restrictive cardiomyopathy. J. Am. Coll. Cardiol. 31, 164A Rodriguez, L., Garcia, M. J., Ares, M. A., Griffin, B. P., Nakatani, S. and Thomas, J. D. (1996) Assessment of mitral annular dynamics during diastole by Doppler tissue imaging : comparison with mitral Doppler inflow in subjects without heart disease and in patients with left ventricular hypertrophy. Am. Heart J. 131, 982–987 # 2002 The Biochemical Society and the Medical Research Society 521 522 G. W. Yip and others 11 12 13 14 15 16 17 18 19 20 Sohn, D. W., Chai, I. H., Lee, D. J. et al. (1997) Assessment of mitral annulus velocity by Doppler tissue imaging in the evaluation of left ventricular diastolic function. J. Am. Coll. Cardiol. 30, 474–480 Palka, P., Lange, A., Fleming, A. D. et al. (1997) Differences in myocardial velocity gradient measured throughout the cardiac cycle in patients with hypertrophic cardiomyopathy, athletes and patients with left ventricular hypertrophy due to hypertension. J. Am. Coll. Cardiol. 30, 760–768 Henein, M. Y. and Gibson, D. G. (1999) Long axis function in disease. Heart 81, 229–231 Henry, W. L., De Maria, A., Gramiak, R. et al. (1980) Report of the American Society of Echocardiography Committee on nomenclature and standards in 2-D echocardiography. Circulation 62, 212–217 Sahn, D. J., De Maria, A., Kisslo, J. and Weyman, A. (1978) Recommendations regarding quantitation in M-mode echocardiography : results of a survey of echocardiographic measurements. Circulation 58, 1072–1083 Schiller, N. B., Shah, P. M., Crawford, M. et al. (1989) Recommendations for quantitation of the left ventricle by two-dimensional echocardiography. American Society of Echocardiography Committee on Standards, Subcommittee on Quantitation of Two-Dimensional Echocardiograms. J. Am. Soc. Echocardiogr. 2, 358–367 Schiller, N. B. (1991) Two-dimensional echocardiographic determination of left ventricular volume, systolic function, and mass. Summary and discussion of the 1989 recommendations of the American Society of Echocardiography. Circulation 84 (Suppl.), I280–I287 Myreng, Y. and Smiseth, O. A. (1990) Assessment of left ventricular relaxation by Doppler echocardiography : A comparison of isovolumic relaxation time and transmitral flow velocities with the time constant of isovolumic relaxation. Circulation 81, 260–266 Rakowski, H., Appleton, C., Chan, K. L. et al. (1996) Canadian consensus recommendations for the measurement and reporting of diastolic dysfunction by echocardiography : from the Investigators of Consensus on Diastolic Dysfunction by Echocardiography. J. Am. Soc. Echocardiog. 9, 736–760 Oh, J. K., Appleton, C. P., Hatle, L. K., Nishimura, R. A., Seward, J. B. and Tajik, A. J. (1997) The noninvasive assessment of left ventricular diastolic function with two-dimensional and Doppler echocardiography. J. Am. Soc. Echocardiogr. 10, 246–270 21 22 23 24 25 26 27 28 29 30 31 32 33 Nishimura, R. A. and Tajik, A. J. (1997) Evaluation of diastolic filling of left ventricle in health and disease : Doppler echocardiography is the clinician’s Rosetta stone. J. Am. Coll. Cardiol. 30, 8–18 Yamamoto, K., Nishimura, R. A., Burnett, Jr, J. C. and Redfield, M. M. (1997) Assessment of left ventricular end-diastolic pressure by Doppler echocardiography : contribution of duration of pulmonary venous versus mitral flow velocity curves at atrial contraction. J. Am. Soc. Echocardiogr. 10, 52–59 Willenheimer, R., Cline, C., Erhardt, L. and Israelsson, B. (1997) Left ventricular atrio-ventricular plane displacement : An echocardiographic technique for rapid assessment of prognosis in heart failure. Heart 78, 230–236 Bland, J. M. and Altman, D. G. (1986) Statistical methods for assessing agreement between two methods of clinical measurement. Lancet i, 307–310 Brutsaert, D. L. and Sys, S. U. (1989) Relaxation and diastole of the heart. Physiol. Rev. 69, 1228–1315 Robinson, T. F., Factor, S. M. and Sonnenblick, E. H. (1986) The heart as a suction pump. Sci. Am. 254, 84–91 Vasan, R. S., Benjamin, E. J. and Levy, D. (1995) Prevalence, clinical features and prognosis of diastolic heart failure : an epidemiologic perspective. J. Am. Coll. Cardiol. 26, 1565–1574 Yip, G. W. K., Ho, P. P. Y., Woo, K. S. and Sanderson, J. E. (1999) Comparison of frequencies of left ventricular systolic and diastolic heart failure in Chinese living in Hong Kong. Am. J. Cardiol. 84, 563–567 Keren, G., Sonnenblick, E. H. and LeJemtel, T. H. (1988) Mitral annulus motion. Relation to pulmonary venous and transmitral flows in normal subjects and in patients with dilated cardiomyopathy. Circulation 78, 621–629 Bauer, R., Busch, U., van de Flierdt, E. et al. (1988) Altersabha$ ngkeiten der Herzfunktion bei Herzgesunden (Age-related heart function in patients with healthy hearts). Z. Kardiol. 77, 632–641 Pfisterer, M. E., Battler, A. and Zaret, B. L. (1985) Range of normal values for left and right ventricular ejection fraction at rest and during exercise assessed by radionuclide angiography. Eur. Heart J. 6, 647–655 Port, S., Cobb, F. R., Coleman, E. and Jones, R. H. (1980) Effect of age on the response of the left ventricular ejection fraction to exercise. N. Engl. J. Med. 303, 1133–1137 Wandt, B., Bojo$ , L., Hatle, L. and Wranne, B. (1998) Left ventricular contraction pattern changes with age in normal adults. J. Am. Soc. Echocardiogr. 11, 857–863 Received 18 June 2001/9 October 2001; accepted 22 November 2001 # 2002 The Biochemical Society and the Medical Research Society