Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Butyric acid wikipedia , lookup
Fatty acid synthesis wikipedia , lookup
Pharmacometabolomics wikipedia , lookup
Metalloprotein wikipedia , lookup
Microbial metabolism wikipedia , lookup
Fatty acid metabolism wikipedia , lookup
Specialized pro-resolving mediators wikipedia , lookup
Evolution of metal ions in biological systems wikipedia , lookup
Citric acid cycle wikipedia , lookup
LABORATORY INVESTIGATION
MYOCARDIAL ISCHEMIA
Delineation of myocardial oxygen utilization with
carbon-11-labeled acetate*
MICHAEL BROWN, M.B.B.S., DAVID R. MARSHALL, B.S., BURTON E. SOBEL, M.D.,
STEVEN R. BERGMANN, M.D., PH.D.
AND
Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017
ABSTRACT Although positron-emission tomography (PET) with labeled fatty acid delineates infarct
size and permits qualitative assessment of fatty acid utilization, quantification of oxidative metabolism
is limited by complex alterations in the pattern of utilization of fatty acid during ischemia and
reperfusion. Because metabolism of acetate by myocardium is less complex than that of glucose or
palmitate, we characterized kinetics of utilization of radiolabeled acetate in 37 isolated rabbit hearts
perfused with modified Krebs-Henseleit buffer and performed a pilot tomographic study in man.
Results of initial experiments with carbon-14-labeled acetate ("4C-acetate) indicated that the steadystate extraction fraction of acetate averaged 61.5 + 4.0% in control hearts (n = 4), 93.6 ± 0.9%
in hearts rendered ischemic (n = 4), and 54.8 + 4.0% in hearts reperfused after 60 min of ischemia
(n = 3). Oxidation of "4C-acetate, assessed from the rate of efflux of "4CO2 in the venous effluent,
correlated closely with the rate of oxygen consumption under diverse metabolic conditions (r = .97,
p < .001). In addition, no significant differences were observed between rates of efflux of total 14C
in all chemical species (reflecting total clearance of tracer from myocardium) and efflux of 4'CO2.
Clearance of 1 1C-acetate, measured externally with gamma probes in normal and ischemic myocardium,
correlated closely with clearance of "4C-acetate measured directly in the effluent (r = .99, p < .001)
and with overall myocardial oxygen consumption (r = .95, p < .001). Accumulation and clearance
of 1 'C-acetate from human myocardium with PET demonstrated kinetics comparable to those seen with
radiolabeled acetate in vitro. Thus externally detectable clearance of 1 1 C-acetate provides a quantitative
index of myocardial oxidative metabolism despite variation in the pattems of intermediary metabolism
that confounds interpretation of results with conventionally used tracers such as glucose and fatty acid.
Circulation 76, No. 3, 687-696, 1987.
POSITRON-EMISSION TOMOGRAPHY (PET) of
myocardium with tracers of intermediary metabolism
such as carbon-11-labeled palmitate (1 C-palmitate)
delineates infarct size. 1-3 However, quantification of
overall, regional oxidative metabolism has been elusive because of changes in contributions of energy
utilization from specific substrates to net oxygen consumption under diverse conditions . Thus, as we have
recently demonstrated, shifts from fatty acid to glucose
From the Cardiovascular Division, Department of Internal Medicine,
Washington University School of Medicine, St. Louis.
Supported in part by NIH grant HL 17646, SCOR in Ischemic Heart
Disease. Dr. Brown is supported by the Heart Research Foundation of
South Australia.
Address for correspondence: Michael Brown, M.B.B.S., Cardiovascular Division, Washington University School of Medicine, 660 S.
Euclid Ave., Box 8086, St. Louis, MO 63110.
Received Jan. 21, 1987; revision accepted May 28, 1987.
Presented in part at the 59th Annual Scientific Sessions of the American Heart Association, Dallas, November 1986.
*All editorial decisions for this article, including selection of reviewers and the final disposition, were made by a guest editor. This procedure
applies to all manuscripts with authors from the Washington University
School of Medicine.
Vol. 76, No. 3, September 1987
oxidation and from aerobic to anaerobic glycolysis in
hearts rendered ischemic preclude accurate estimation
of oxidative metabolism by residue detection of any one
of the tracers conventionally used in PET such as 18Fdeoxyglucose or "C-palmitate evaluated in isolation.5
Quantification of regional oxidative metabolism with a
single tracer would be useful to delineate the extent and
distribution of jeopardized ischemic myocardium,
objectively evaluate its response to interventions such
as coronary thrombolysis or angioplasty, and characterize effects of physiologic and pharmacologic interventions designed to salvage ischemic tissue or metabolic function. Judging from information available
and results of previous studies,4-8 we considered the
possibility that overall citric acid cycle flux and hence
overall oxidative metabolism could be measured externally from the rate of myocardial clearance of radiolabeled acetate.
Citric acid cycle flux is not estimable from measurements of myocardial utilization of radiolabeled palmitate for several reasons, including the dependence of
687
BROWN et al.
additional pilot study was performed to
the feasibility of imaging human myocardium
with PET and "C-acetate.
Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017
fatty acid utilization on the availability and/or inhibi-
tracer. An
tory effects of alternative substrates.9 Backdiffusion of
nonmetabolized "C-palmitate in the presence of myocardial ischemia contributes up to 50% of the total
clearance of radioactivity from the myocardium and
thereby overestimates overall rates of oxidation.7 In
addition, preferential inhibition of /8-oxidation occurs
with ischemia,8 dissociating rates of /3-oxidation from
rates of citric acid cycle turnover. Similar difficulties
are encountered with glucose or glucose analogs. Thus
glucose labeled with "C undergoes disparate metabolic
fates depending on physiologic conditions, including
incorporation into glycogen; conversion to constituents
of lipid, carbohydrate, and protein intermediates; anaerobic glycolysis; and flux through the citric acid cycle.
Metabolism of deoxyglucose labeled with fluorine- 18
is somewhat more constrained but indicative only of
glucose uptake rather than myocardial oxygen utilization per se. The kinetics of both tracers are influenced
markedly by arterial glucose concentration, neurohumoral environment, and prevailing concentrations of
other substrates.9
To overcome limitations inherent in the use of
labeled glucose or fatty acid alone for assessment of
myocardial oxidation, we performed the present study
with acetate, which is readily oxidized to CO2 via the
citric acid cycle'0- 13 and exhibits essentially one pathway of metabolism in the heart. 14 We considered it
likely that these characteristics would make radiolabeled acetate particularly suitable as a tracer for quantification of net myocardial oxidative metabolism in
selected regions of the heart under diverse conditions.
Although "C-acetate has been used in preliminary
studies of experimental animals and patients, kinetics
have not been related to oxidative metabolism.'5-17
Accordingly, the present study was undertaken to
determine whether externally detected clearance of
"C-acetate would provide a quantitative index of myocardial oxidative metabolism. Because of the short
half-life of "C (20.4 min), "4C-acetate was used in
initial studies in which the biochemical fate of tracer
was defined. Subsequent results were obtained by
external detection of radioactivity from "C-acetate.
Our objectives were to (1) define the extraction of
14C-acetate under diverse conditions of metabolism and
flow, (2) determine relationships between the rate of
efflux of 14CO2 in venous effluents, reflecting oxidation
of "4C-acetate, and oxygen consumption, and (3) define
relationships between the externally detectable clearance of myocardial "C radioactivity and myocardial
oxygen consumption in isolated perfused rabbit hearts
subjected to defined flow, oxygenation, and delivery of
assess
688
Methods
Male New Zealand rabbits weighing 3 to 5 pounds were
stunned with a blow to the head. Heart were rapidly excised and
perfused with nonrecirculating, oxygenated (95% 02/5% C02)
modified Krebs-Henseleit perfusate containing 400 gM albumin, 400 gM palmitate, 5 mM glucose, and 70 mU/liter insulin.
Hearts were paced at a rate of 180 beats/min with a right atrial
bipolar electrode. Left ventricular pressure was monitored continuously with a fluid-filled latex balloon inserted through the left
atrium. The first derivative of left ventricular pressure (dP/dt)
and coronary perfusion pressure were also recorded. The left
ventricular pressure-time index was calculated from the product
of the area under the left ventricular systolic pressure curve and
heart rate. 18 The pulmonary artery was cannulated for collection
of coronary venous effluent. Oxygen utilization was calculated
from the product of arteriovenous oxygen content difference per
milliliter of perfusate and flow, normalized for heart weight. 18
Experimental procedure. To determine the steady-state
extraction fraction of 14C-acetate and production of '4C02 under
diverse conditions, 1 hearts were perfused with 20 MCi/liter
l-14C-acetate (specific activity 56 mCi/mmol; New England
Nuclear) over a period of 30 min.
The extraction fraction was calculated from the arteriovenous
14C-acetate difference as a percentage of arterial '4C-acetate.
High-pressure liquid chromatography (see below) was used to
separate 14C-acetate, which was then quantified by gamma
counting. Conditions investigated were normal flow (20 ml/min,
n = 4) and reduced flow (2 ml/min, n 4) with and without
the addition of 50 gM of unlabeled sodium acetate. The extraction fraction was measured at 20 to 30 min in control hearts and
at both 10 and 30 min in ischemic hearts. The extraction fraction
was also measured in hearts reperfused at control flow rates after
60 min of ischemia (n = 3), 20 to 30 min after commencement
of '4C-acetate infusion.
In 16 additional hearts studied under control conditions, with
hypoxia (flow rate of 20 ml/min with hypoxic media), with
ischemia, or with reperfusion after ischemia, the rate of oxidation of 14C-acetate was determined based on the measured rate
of efflux of 14C02 in the venous effluent over a 40 min interval
after a 2 min infusion of 15 ,uCi 14C-acetate. The 2 min infusion
interval was selected based on results in pilot studies of the
arterial time-activity curve after intravenous administration of
tracer in vivo.
After the completion of these initial studies. 0.5 mCi ' Cacetate and 15 ,uCi 14C-acetate were infused simultaneously over
2 min in 10 hearts. Clearance of ' 'C radioactivity was measured
externally by residue detection, and the rates of efflux of total
14C and '4CO2 were determined in the effluent over 20 to 40 min.
In four of these hearts, the "C myocardial residue-time activity
curve was determined at three different workloads induced by
changing preload and heart rate (low and medium workload) and
by infusion of isoproterenol (5 X 10-7M, high workload).
Measurement of "4CO2 radioactivity. Coronary venous
effluent was collected at 1 min intervals into tubes containing
sodium hydroxide to trap 14CO2. Total 14C radioactivity was
determined by placing 1 ml of perfusate in 1 ml of Protosol (New
England Nuclear) and adding 1 0 ml of Aquasol II (New England
Nuclear) before /3-scintillation spectrometry. A duplicate sample was treated with 0.25 ml of 5N HCl and allowed to stand
overnight on ice (to minimize loss of "4C-acetate) before spectrometry. Assay of standards verified greater than 99.9% loss of
14C-bicarbonate and greater than 98% retention of 14C-acetate
CIRCULATION
LABORATORY INVESTIGATION-MYOCARDIAL ISCHEMIA
Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017
under these conditions. The 14C02 content per milliliter of
perfusate was calculated as the difference between total and
residual radioactivity after treatment with HCl.
Measurement of "'C-labeled metabolites in venous effluent. To characterize conversion of labeled acetate to metabolites
other than labeled C02, albumin was precipitated in samples of
venous effluent with an equal volume of 10% perchloric acid.
The samples were centrifuged, and supematant fractions were
allowed to stand on ice overnight for dissipation of 14Co2.
Samples were stored at - 700 C. Metabolites were separated with
a SpectraPhysics high-pressure liquid chromatography (HPLC)
system (San Jose, CA) and detected with a Waters Differential
Refractometer. Optimal separation of standards was accomplished with two organic acid columns in sequence (Biorad
Aminex HPX 87H and Benson 0A850) with 0.O0N H2S04 at
a flow rate of 0.5 ml/min.'9 Retention times of individual citric
acid cycle intermediates were determined, as were those for
pyruvate, lactate, acetoacetate and ,3-hydroxybutyrate. Because
retention times for some species overlapped, additional separation for acetate and acetoacetate was accomplished with a C 18
reverse-phase column (LiChrosorb RP 18, E. Merk, Darmstadt,
W. Germany) in combination with an organic acid column.
Fractions of effluent separated on the basis of measured retention
times of each standard were collected for assay of radioactivity.
Lactate and glucose were assayed conventionally with commercially available enzymatic assay kits (Behring Diagnostic,
La Jolla, CA). Utilization and production of substrate were
calculated from the product of arteriovenous concentration differences and flow and normalized for heart weight. Myocardial
lipid was extracted by the Bligh and Dyer procedure,20 and the
percentage of 14C radioactivity in the lipid phase relative to total
myocardial radioactivity was determined.
Synthesis of "C-acetate. A modification of the method
developed by Pike et al.2' was used to prepare ''C-acetate.
"C-labeled carbon dioxide was prepared by the 14N (p,a) "C
reaction in the Washington University Medical Center cyclotron
and bubbled through 3 ml of a 0. IM solution of methylmagnesium bromide (Aldrich Chemical Co., Milwaukee) in diethyl
ether. The product was hydrolyzed with 6 ml of 6N hydrochloric
acid. An additional 6 ml of diethyl ether was then added. The
sample was vortexed, and the organic layer was allowed to
separate from the aqueous layer. The latter was discarded, and
10 ml of 0.9% sodium bicarbonate was added to the organic layer
and vortexed. After separation, the aqueous layer was transferred and bubbled with nitrogen at 500 C. Sterility was maintained by serial filtration through 0.45 and 0.2 ,um filters. Radiochemical purity, determined by HPLC, was consistently
greater than 96%. Estimated specific activity was greater than
1 Ci/mmol.
Residue detection of `C activity. Annihilation photons were
detected with two sodium iodide crystals placed 180 degrees
apart across the heart. Coincidence counts were detected with
an Ortec fast coincidence counter. Singles counts from one
sodium iodide crystal and coincidence counts from both were
recorded on-line with a Digital Equipment Corp. RX-08 minicomputer. Data were subsequently decay-corrected off-line.
Clearance data were fitted with a multiexponential curve-fitting
routine. Although an attempt was made to fit biexponential
solutions to all data, only monoexponential solutions were
apparent in ischemic and hypoxic hearts. The biological halftime (t½A) was calculated from the rate constant (k) and the
relationship t'A = In2/k. The relative magnitude of each phase
of a biexponential fit was calculated by back-extrapolation of the
monoexponential slope of each phase to the time of completion
of infusion of `1C-acetate as a percentage of the sum of both
phases at that time.
Statistical analyses. Data are expressed as mean ± SD.
Multiple comparisons of unpaired and paired samples were
analyzed by analysis of variance followed by t tests corrected for
the number of comparisons by the Bonferroni method.22 Linear
regression was calculated by the least-squares method.
Results
Hemodynamics, flow, and
oxygen
consumption. He-
modynamics and substrate utilization for steady-state
studies (group 1) and clearance studies (group 2) with
14C-acetate are presented in table 1. Hemodynamics
were constant throughout the interval of evaluation in
control hearts. Flow was reduced by 85% to 90% in
ischemic hearts, and myocardial oxygen consumption
was diminished proportionately. Heart rate diminished
by approximately 40% because of atrioventricular
block. Hearts reperfused after 60 min of ischemia
TABLE 1
Hemodynamic variables, oxygen consumption, and glucose and lactate utilization during studies of 14C-acetate extraction (group 1) and
radiolabeled acetate clearance (group 2)
HR
(beats!
min)
Group 1
Control (n=4)
Ischemia (n = 4)
Reperfusion (n=3)
Group 2
Control (n= 10)
Ischemia (n =10)
Hypoxia (n =3)
Reperfusion (n = 3)
LVEDP dP/dt (mm
(mm Hg) Hg/sec)
LVPTI
(mm Hg/
Flow
sec/min)
(ml/g/min)
MVO2
(ml/g/min)
193±7
117 ± 44A
184±7
10±2
7±3
12±8
870±150
200 ± 60A
935±140
2360±660
680± 300A
1920±30
4.04±0.58
0.61 ± 0.22A
4.37±0.76
0.061±0.013
0.009 ± 0.004A
0.057±0.011
187± 19
86 ± 12A
185 ±5
190±4
8±4
9±2
8±2
13 ± 5
970± 180
140 ± 50A
530 ± 58A
2580±490
5.35±0.93
0.069±0.01
0.008 ±0.OO1A
0.0l1 ± 0.002A
0.055 ±0.006
910± 170
550± 260A
0.48 0.1A
1100 ± 740A
2050±620
4.73 ±0.92
4.62 ±0.41
Values are mean ± SD.
HR = heart rate; LVEDP = left ventricular end-diastolic pressure; dP/dt
pressure-time index; MVO2 = myocardial oxygen consumption.
Ap < .01 compared with control.
Vol. 76, No. 3,
September 1987
±
=
Glucose
Lactate
uptake
(mg/g/min)
production
(mg/g/min)
0.099±0.067
0.095 0.021
0.040±0.018
0.21 ±0.26
0.055 ± 0.014
0.435 ±0.044
0.147 ±0.138
first derivative of left ventricular pressure; LVPTI
0.076±0.019
0.091 ±0.035
0.389 ± 0.071A
0.083 ± 0.111
=
left ventricular
689
BROWN et al.
Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017
exhibited left ventricular pressure-time index values
and oxygen consumption similar to those in control
hearts but at marginally higher left ventricular enddiastolic pressure.
Utilization of glucose was depressed in ischemic
hearts. However, the reduction was not statistically
different compared with control hearts in part because
of the increased extraction fraction of glucose at low
flow. Also, glucose utilization varied considerably in
control hearts because of low extraction fraction at high
flow rates. Lactate production was significantly higher
in hypoxic compared with control hearts.
Steady-state utilization of acetate. The steady-state
extraction fraction of 14C-acetate was determined in 1 1
isolated rabbit hearts subjected to a wide range of flow
and altered metabolic states. Extraction fraction of
14C-acetate in hearts perfused at a control flow rate of
20 ml/min with media without added unlabeled sodium
acetate averaged 63.4 ± 9.5%. In ischemic hearts it
averaged 94.9 ± 1.1%. Addition of a physiologic
concentration (50 ,uM) of unlabeled sodium acetate had
no effect on the extraction fraction (59.6 + 1.6% in
control hearts, 93.4 + 0.7% in ischemic hearts). Thus,
in hearts perfused with media with or without unlabeled
acetate, the extraction fraction was significantly higher
with ischemia (p < .001). The extraction fraction of
'4C-acetate remained constant throughout the interval
of ischemia. Hearts reperfused at a flow of 20 ml/min
after 60 min of ischemia exhibited extraction fractions
similar to those in controls (54.8 ± 4.0%; n = 3,
p= NS).
Steady-state production of '4C02 resulting from oxidation of 14C-acetate in control and reperfused hearts
generally occurred within 15 min after onset of perfusion with 14C-acetate and accounted for 86 + 7% of
14C-acetate uptake. The rate of production of 14C02 in
ischemic hearts continued to increase throughout the
period of perfusion but appeared to reach steady state
by 25 min. The delay to equilibrium was presumably
caused by the slower rate of turnover of the citric acid
cycle during ischemia.
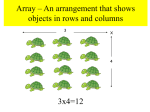
Rate of oxidation of "4C-acetate. The rate of efflux of
'4C02 in venous effluent was characterized under a
variety of conditions after a 2 min infusion of 14Cacetate. Efflux of' 4C02 reached a maximum 2.3 + 0.8
min after the end of the infusion in control hearts (n =
10) but was delayed to 1 1.8 ± 2.6 min in ischemic
hearts (n = 10). Efflux was subsequently biexponential
in control and reperfused hearts (Figure 1, a), consisting of a dominant rapid phase and a smaller slower
phase of efflux. Efflux was monoexponential in ischemic and hypoxic hearts (figure 1, b). The half-times
690
108 - a
c
._
E
E 107 =
C
_
E
CL
U
106
=
Uw
D 105 _
° Totcol 14 C
W_
0
28X_
14C02 (y-2209000&e0
+
120600e-009x )
104 -
_
L_
105
E
16
24
TIME (Min)
1
1
32
40
b
0o
0 00
°O
£
0I
E
1..
*O
0 0
Q
U
U
8
104
LL
0
O Total 14C
C
-J
LL
H- l0 3
8
16
14CO2 (y=32050e 0036)
24
32
40
TIME (Min)
FIGURE 1. Efflux of total 4C and '4CO2 as a function of time after
14C-acetate from (a) one control heart and (b) one ischemic heart. Efflux
of 4CO2 was biexponential in all control hearts and monoexponential
in all ischemic hearts as shown on these examples with the solid lines
fitted from peak efflux. Rate constants for the rapid phase (0.28 min- ')
and slow phase (0.09 min-') in the control and in the ischemic heart
(0.036 min-1) are shown. The rate of efflux of total `'C is very similar
to the rate of "`CO2 efflux.
of efflux calculated from the rapid phase were 3.2 +
0.9 min for control (n = 7), 1.9 + 0.4 min for
isoproterenol-stimulated (n = 3), 15.0 ± 0.4 min for
ischemic (n = 10), 9.3 + 2.2 min for hypoxic (n 3), and 3.1 ± 0.2 min for reperfused hearts (n = 3).
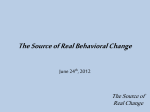
The rates of efflux of 14C02 under the diverse conditions studied correlated closely with the rate of oxygen
consumption in each heart (figure 2, r = .97, p <
.001). The rate of efflux also correlated closely with
indexes of cardiac work such as left ventricular pressure-time index (r = .86, p < .001) and left ventricular
dP/dt (r = .97, p < .001). Studies during hypoxia
showed a relationship between oxygen consumption
and rate constant of the rapid phase of efflux of 14C02
similar to that seen in all other studies, indicating that
the reduced rate constant seen with ischemia was
caused by impaired oxygen delivery rather than
reduced clearance as a result of low flow per se.
CIRCULATION
LABORATORY INVESTIGATION-MYOCARDIAL ISCHEMIA
0.4F
0
tn
z 0.3
z0.2
0
*0
l
0 .1
U
.
!R
0.1
y - 3.61x + 0.01
r -0.97
0
n=26
I
0
0.02
0.04
0.06
0.08
0.10
0.12
Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017
OXYGEN CONSUMPTION (ml /gm/m)in)
FIGURE 2. Correlation between myocardial oxygen consumption and
the rate constant of the rapid phase of venous efflux of 14C02. The latter
is indicative of the rate of oxidation of "4C-acetate (r = .97, p < .001).
Prediction of "4CO2 efflux based on total venous efflux of
14C radioactivity. The rate of efflux of total 14C radioactivity in the venous perfusate was used to estimate the
rate of '4CO2 efflux, which in turn was used to determine whether acetate oxidation could be measured
externally by residue detection of myocardial "C-acetate. Because dynamic studies with PET define total
clearance of tracer from myocardium but not clearance
of "'CO2 specifically, this comparison was performed
to identify potential limitations of estimating oxidation
of "C-acetate from analysis of myocardial residue
time-activity curves.
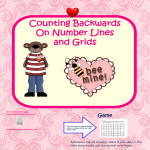
Half-times of the rapid phase of "4CO2 efflux and
total "'C efflux were almost identical in control hearts
whether or not stimulation with isoproterenol was used
(figure 3). A similar concordance was seen in reperfused hearts and in hypoxic hearts (figure 3). In ischemic hearts, the half-times for "4CO2 efflux (15.8 ± 4.8
min) were slightly longer than those for total 14C efflux
20
J
(14.7 ± 3.4 min) although the difference was not
statistically significant. This modest discrepancy was
attributable to a lower fraction of '4C02 comprising
total 14C radioactivity in the venous effluent (figure 4).
In control and reperfused hearts, nearly all radioactivity (96.0 ± 1.1%) in the venous effluent was in
the form of 4CO2 during the first 20 min (figure 4). In
contrast, in ischemic hearts, 14C02 contributed 75.7 ±
7.2% of total venous radioactivity during the period of
monoexponential clearance of "4CO2 10 to 30 min after
the completion of the infusion of "4C-acetate (figure 4).
Thus, despite the presence of backdiffused "4C-acetate
or metabolites of "4C-acetate in the venous effluent of
ischemic hearts, the disparity between calculated
14C02 efflux and total "4C efflux was small.
Metabolites of "4C-acetate. The metabolites in the
venous effluent were separated by HPLC to determine
whether radioactivity that was not accounted for by
14CO2 was attributable to backdiffused "4C-acetate or
to metabolites. In the effluent from a control heart, 4
min after the completion of the infusion of 14C-acetate
96% of the venous effluent was in the form of "'CO2.
Nonmetabolized "4C-acetate comprised 19% of non"4CO2 activity (thus 0.8% of total effluent radioactivity). Thirty-five percent of non-CO2 activity was attributable to ketones, specifically 14C-,3 hydroxybutyrate
(24%) and 14C-acetoacetate (11%). In ischemic hearts
at 4 min after the completion of tracer infusion, 44%
of venous effluent was in the form of 14CO2. Backdiffused "4C-acetate contributed 3.3 ± 1.3% of non14"C2 activity, whereas 14C-,3 hydroxybutyrate accounted for 73.7 ± 6.4% and "4C-acetoacetate for 0.7
± 1.2% (n = 3). After 14 min, 80% of total radioactivity was in the form of "4CO2. Of non-'4C02 activity, 1 ± 0.9% was attributable to "4C-acetate, whereas
"4C-,3 hydroxybutyrate comprised 40.6 ± 10.6% and
14C-acetoacetate 3.6 ± 2.7%. The remaining 14C
metabolites were largely citrate, succinate, and lactate
14CO2
Total 14C
l=J 2-10 Min
c 16
10-20 Min
_ 20-30 Min
- 100
412
U 80
0
0 60
X
-a
X
Ischemia Reperfusior
Isoproterenol Hypoxia
FIGURE 3. Half-times of the rapid phase of 14Co2 (open bars) and total
14C efflux (hatched bars) over a wide range of flows and metabolic
conditions. The half-time of "4CO2 efflux was inversely proportional to
workload and oxygen consumption. No significant difference was found
Control
between the half-times for 14CO2 and for total 14C efflux within each
group.
Vol. 76, No. 3, September 1987
40
20
00 0
Control
Hypoxia
Ischemia
Reperfusion
FIGURE 4. Contribution of 14CO2 radioactivity to total venous radioactivity during the intervals shown after completion of infusion of
"4C-acetate. Limited myocardial release of metabolites of "'C-acetate
occurred in hypoxic and ischemic hearts as discussed in the text.
691
BROWN et al.
TABLE 2
Percentage of total non-"CO2 venous radioactivity due to labeled metabolites after a 2 min infusion of "4C-acetate in three
ischemic hearts
Time
Acetate
Hydroxybutyrate
Acetoacetate
Citrate
Succinate
Lactate
2-4 min
12-14 min
3.3 1.3
1.0 0.9
73.7 6.4
40.6 10.6
0.7 1.2
3.6 2.7
5.7 2.6
12.0 3.3
3.4 + 2.5
20.2 ± 9.8
13.8 ± 1.8
4.6 + 4.7
Values are means ± SD. In control hearts, nearly all radioactivity (96.0 ± 1 .1 %) in the venous effluent was in the form of
14CO0. In ischemic hearts, 2 to 4 min after 14C-acetate infusion 44% of effluent was in the form of 14CO'. This production
increased to greater than 80% (see figure 4) after 14 min.
Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017
with percentages of radioactivity increasing in each
from 6 to 12 min after completion of the infusion with
'4C-acetate (table 2).
The distribution of the 14C label between the aqueous
and lipid fraction of myocardium was determined in
four hearts after completion of the 14C-acetate clearance studies. The percentage of total radioactivity in the
lipid fraction of two control hearts (0% and 12.6%) did
not differ significantly from those in two ischemic
hearts (2.8% and 5.5%).
External assessment of clearance of "C-acetate. Clearance of "C-acetate was measured in six control and
four ischemic hearts by analysis of externally detected
myocardial residue time-activity curves and compared
with the clearance of 14C-acetate measured by direct
assay of radioactivity in the effluent. In control hearts,
1"C-acetate clearance was measured at 14 workloads
and compared with oxygen consumption. The decline
in myocardial residue counts as a function of time was
biphasic (figures 5, a and b) and data from control
hearts could be closely fitted with biexponential solutions. The biexponential clearance of the myocardial
residue suggested that the "C label was present within
the myocardial cell in at least two separate pools, one
clearing rapidly and one slowly. The relative size of
each was approximated from the size of each phase of
the biexponential curve. Clearance was predominantly
due to the rapid phase, since the slowly clearing pool
accounted for only 7.4 + 3.0% of total "C radioactivity. No significant change in the size of this pool was
seen with changes in cardiac work or oxygen consumption. The rate constant of the initial phase of
clearance increased with increased workload in parallel
with increased oxygen consumption (figure 5, a and b).
No change in the rate constant of the late phase was seen
with increased workload (t',2 28.5 + 16.0 min).
The myocardial residue time activity curve in four
ischemic hearts, analyzed over the same interval as that
used to calculate 14Co2 efflux (i.e., 10 to 40 min after
"C-acetate infusion), was monoexponential (figure
5, c).
692
In all hearts, the rate constant of the initial phase of
the residue clearance was very similar to and correlated
closely with total efflux of 14C (figure 6, a, r = .99,
p < .001). Consistent with the close correlations
between the rate of total 14C efflux, 14Co2 efflux and
oxygen consumption, "C-acetate clearance and oxygen consumption correlated closely as well (figure 6,
b; r = .95, p < .001).
"C-acetate residue curves in ischemic hearts were
analyzed over the interval in which efflux of "CO2 was
monoexponential. Thus the first 10 min of the residue
curve were excluded. However, sampling intervals
would be difficult to discern in clinical studies from
inspection of residue curves only. To determine the
error involved when an earlier interval was used, we
analyzed rates during the first 20 min of the residue
curves in ischemic hearts as well. No significant differences were observed for half-times from this interval
(19.9 ± 2.5 min compared with 20.3 ± 1.9 min).
Thus, although oxidation of acetate and production of
CO2 are retarded with ischemia, the interval selected
for calculation of rate constant does not appear to be
critical.
PET. Although this study was designed primarily to
characterize the suitability of radiolabeled acetate as a
tracer for use in estimating myocardial oxygen consumption under diverse conditions in isolated perfused
hearts, its ultimate objective was to initiate development of an approach applicable to intact hearts in vivo
in experimental animals23 and in patients evaluated by
PET. Accordingly, the feasibility of imaging human
myocardium after intravenous administration of 0.3 to
0.4 mCi/kg "C-acetate was explored. Images of "1C
acetate accumulation in myocardium were readily
acquired over brief imaging intervals averaging 60 to
120 sec. Myocardial residue time activity curves were
generated from regions of interest encompassing the
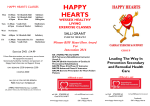
left ventricular wall in one midventricular slice. Rapid
clearance of "C-acetate from arterial blood resulted in
excellent contrast between the left ventricular wall and
cavity (figure 7). The half-time of clearance of 1"C
CIRCULATION
LABORATORY INVESTIGATION-MYOCARDIAL ISCHEMIA
105
a
b
0
z
0
LI,
0
U
z
0 104
U
w
cL
LLI
W
a-
I-
Z 103
z
0
0
U~
U
y=30271e 0213x + 1779e 0032x
-
lul
4
+
8
12
16
20
24
TIME (Min)
106
TIME (Min)
c
Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017
z
0
U
ui
lU
LI
bU
z 104
0
U
E
lull
y-= 133 865,60O3.
8
16
24
32
40
TIME (Min)
FIGURE 5. Externally detected myocardial residue time-activity curves after infusion of "C-acetate. Clearance from a control
heart (a) before and (b) after stimulation with isoproterenol was biexponential as shown by the solid line. The rate constant of
the rapid phase increased from 0.23 to 0.49 min-' with isoproterenol. Clearance from the ischemic heart (c) was monoexponential. Fits were made to coincide with the monoexponential efflux of "CO2, from 14 to 40 min in this example, as shown
by the solid line.
radioactivity from myocardium was 10.5 min in this
example from a normal subject. In view of these
results, it appears likely that quantitative estimation of
clearance of "C-acetate from selected regions of myocardium and hence estimation of regional myocardial
oxygen consumption will be possible in patients within
the spatial and temporal limitations of the particular
tomographic instruments used.
Discussion
Although acetate is a substrate known to be utilized
readily by the heart, the low concentrations of acetate
in human plasma (ranging from 25 to 100 ,uM)24' 25
dictate a low contribution of acetate to total myocardial
substrate utilization. Nevertheless, acetate is oxidized
readily by the heartl0- 12 and is capable of sustaining
energy production when provided as a sole substrate.
Availability of acetate also diminishes utilization of
glucose and palmitate.°0' 1 Metabolism of acetate,
Vol. 76, No. 3, September 1987
after activation to acetyl coenzyme A (CoA), is predominantly oxidative via the citric acid cycle. We
postulated that the rate of oxidation of labeled acetyl
CoA would indicate overall citric acid cycle flux. The
latter would be an index of oxygen consumption and
energy production, since oxidative phosphorylation is
closely coupled to the citric acid cycle. However,
minor changes in the ratio of citric acid cycle flux to
oxygen consumption will result from variation in the
proportions of individual substrates utilized by the
heart. The extent of this variation is small, however,
as shown by calculations of oxygen consumption
resulting from complete oxidation of each major substrate serving as the source of acetyl CoA for the citric
acid cycle. For example, oxidation of glucose, lactate,
and palmitate consume 3.0, 3.0, and 2.9 moles of
oxygen per mole of acetyl CoA utilized, respectively.
With palmitate as the reference, oxygen consumption
calculated from citric acid cycle flux would be over693
BROWN et al.
*c
51
0.s -a
ui
LU
U
z
< 0.4
0
LU
! 0.33F
ui
U
0
U1 WW
U- 2.
:=) 0.2
z
0.1
_
z
y
- 1.05 x - 0.01
r
- 0.99
n=10
0
U
4
0.1
0.3
0.2
0.4
0.5
RATE CONSTANT OF TOTAL 14C EFFLUX (Minr1)
*
0
Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017
0
0.4
00
._J
0.3
z
9-.c
Z
U)
0
0.2 _
0
0
0
*
0.1
y 3.89x-0.02
/ r 0.95
=
n
=
18
'A
0D2
0.10
0.04
0.06
0.08
0.12
OXYGEN CONSUMPTION (mi/gmn/min)
FIGURE 6. a, Correlation between the rate constants for total 14C
efflux and the rate constants of the "C residue time-activity curve from
10 hearts. Both rate constants were calculated from the rapid phase of
biexponential curves. b, Correlation between myocardial oxygen consumption and the rate constant of the rapid phase of the externally
detected myocardial residue time-activity curves in 18 studies after
D
infusion of
`C-acetate.
estimated by 4% if glucose were the only substrate
utilized. The same overestimation would be encountered if lactate were the only substrate utilized.
The rate of efflux of 14C02 after '4C-acetate infusion
from myocardium perfused with media containing
physiologic concentrations of glucose, palmitate, and
acetate was found to correlate very closely with myocardial oxygen consumption. Despite some backdiffusion of '4C-acetate and modest efflux of labeled
metabolites other than CO2 with ischemia, the rate of
efflux of total 14C activity correlated very closely with
efflux of "4CO2. Thus the rate of clearance of the
myocardial residue after '4C-acetate correlated closely
with myocardial oxygen consumption.
Metabolism of acetate. The pathways involved in ace694
tate metabolism are limited in comparison with those
involved in glucose or fatty acid metabolism. In contrast to the incorporation into lipid or conversion to
ketone bodies in the liver, oxidation is the predominant
mode of metabolism in myocardium. After the activation of acetate to acetyl CoA in the mitochondria,
acetyl CoA is oxidized via the citric acid cycle. Rapid
expansion of the normally small acetyl CoA pool by
utilization of acetate may result in the reversible conversion to acetylcarnitine, providing a larger storage
pool in the cytoplasm. In mitochondria, acetyl CoA can
be incorporated into fatty acids by de novo synthesis
or chain elongation. However, the extent of either is
less than 1% in normoxic hearts.'2 Although the rate
of incorporation can increase up to 12-fold in isolated
perfused rat hearts with hypoxia, 26 incorporation into
lipid as a percentage of total intracellular pool is small.
Results with hearts from our study indicate that in
ischemic hearts, in which lipid incorporation would be
expected to be maximal, the majority of the 14C label
remains in aqueous rather than the organic phase of
extracts. Thus incorporation into lipid is minimal.
Studies with 13C-acetate and magnetic resonance spectroscopy have shown incorporation of label into amino
acids via citric acid cycle intermediates (e.g., into
glutamate from a-ketoglutarate).27' 28 Possibly the
slow phase of the "C residue curve represents metabolism of either fatty acids or amino acids containing the
"C label.
The conversion of pyruvate to acetyl CoA is essentially irreversible in animal tissues,29 limiting the diversity of metabolic end products of radiolabeled acetate.
This is a major disadvantage of acetate as a tracer of
overall oxidative metabolism in comparison with other
tracers such as glucose, pyruvate, or lactate from which
production and subsequent release of metabolites such
as labeled alanine can distort relationships between
clearance of the tracer and oxygen consumption. No
equilibration between 13C-acetate and alanine has been
found by magnetic resonance spectroscopy in the
nonischemic perfused rat heart,27 suggesting that no
exchange occurs with pyruvate.
The heart, unlike other organs such as the liver, does
not generally produce ketone bodies.30 ' We identified production of small quantities of 14C-fl hydroxybutyrate and acetoacetate in both normoxic and ischemic hearts consistent with analyses of pig heart
extracts,32 isolated rat heart mitochondria,33 and dog
hearts rendered hypoxic.
Implications for PET. Myocardial extraction of 14Cacetate was high despite the high flow rates required for
normoxic perfusion of isolated hearts with buffer soluCIRCULATION
LABORATORY INVESTIGATION-MYOCARDIAL ISCHEMIA
FIGURE 7. Misdventricular tomographic recon~
struction from a normal subject 3 to 8 min after bolus
intravenous injection of 23 mCi of ''C-acetate.
Excellent contrast between rnvocardium and lung or
blood pool is observed. The lateral left ventricular
wall is to the right, apex is to the top. and septum is
to the left.
Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017
tions not containing erythrocytes. It is high also in
human subjects.35 Extraction increased further to 94%
in ischemic hearts in our study because of the increased
residence time of the tracer in the vasculature. Uptake
was not diminished by increasing the concentration of
acetate to that found in plasma in vivo.
Backdiffusion of '4C-acetate was modest even in
ischemic hearts. In contrast, ''C-palmitate backdiffusion from ischemic canine hearts constitutes approximately 50% of efflux of radioactivity from the heart.7
Although release of labeled ketone bodies contributed
20% to 30% of total radioactivity in the venous effluent
from ischemic hearts once maximum 14C02 production
had been reached, it constituted approximately 39%
during the first 10 min. Because the efflux of '4CO2
from 14C-acetate was delayed by ischemia, analysis of
the residue curve earlier could potentially introduce
error. However, we found that selection of the portion
of the residue time-activity curve in ischemic hearts
was not critical.
The high extraction fraction of ''C-acetate and the
rapid decline of blood pool radioactivity in vivo augur
well for tomographic imaging of the heart with " Cacetate. The increased extraction fraction in ischemic
myocardium should facilitate tomography even when
delivery is limited by low blood flow. Synthesis of
"C-acetate is rapid with high radiochemical purity and
high yields. Preliminary results with intravenous "Cacetate in canine23 and human myocardium document
high-quality imaging and rapid clearance of the blood
pool radioactivity. Because myocardial residue timeactivity curves can be measured easily with serial PET
images and regional activity quantified over time,
metabolism of ''C-acetate and hence myocardial oxyVol. 76. No. 3. September 1987
gen consumption should be quantifiable. Further validation of the approach developed will require extensive studies in vivo and evaluation of potential effects
of changes of concentrations of substrates in plasma.
Nevertheless, results of the present study suggest that
PET with "C-acetate should permit accurate estimation of regional myocardial oxidative metabolism
noninvasively.
We thank Joanne Markham for assistance with mathematical
modeling, Jim Bakke for technical assistance, and Becky Parrack for preparation of the typescript.
References
1. Weiss ES. Hoffman EJ. Phelps ME. Welch MJ. Henry PD. TerPogossian MM. Sobel BE: External detection and visualization of
myocardial ischemia with ''C-substrates in vitro and in vivo. Circ
Res 39: 24. 1976
2. Weiss ES. Ahmed SA. Welch MJ. Williamson JR. Ter-Pog,ossian
MM. Sobel BE: Quantification of infarction in cross sections of
canine myocardium in vivo with positron emission transaxial tomography and ''C-palmitate. Circulation 55: 66. 1977
3. Sobel BE. Weiss ES. Welch MJ. Siegal BA. Ter-Pogossian MM:
Detection of remote myocardial infarction in patients with positron
emission transaxial tomography and intravenous ''C-panlmitate.
Circulation 55: 853. 1977
4. Opie LH. Owen P. Riemersma RA: Relative rates of oxidation of
glucose and free fatty acids by ischemic and nonischemic myocardium after coronary artery ligation in the dog. Eur J Clin Invest
3: 419. 1973
5. Myears DW, Sobel BE, Bergmann SR: Substrate utilization in
ischemic and reperfused canine myocardium: quantitative considerations. Am J Physiol (in press)
6. Taegtmeyer H, Roberts AFC. Raine AEG: Energy metabolism in
reperfused heart muscle: metabolic correlates to return of function.
J Am Coil Cardiol 6: 864. 1985
7. Fox KAA. Abendschein DR. Ambos HD. Sobel BE. Bergmann SR:
Efflux of metabolized and nonmetabolized fatty acid from canine
myocardium. Circ Res 57: 232. 1985
8. Whitmer JT. Idell-Wenger JA. Rovetto MJ. Neely JR: Control of
fatty acid metabolism in ischemic and hypoxic hearts. J Biol Chem
253: 4305. 1978
9. Bergmann SR. Fox KAA. Geltman EM. Sobel BE: Positron emission tomography of the heart. Prog Cardiovasc Dis 28: 165, 1985
10. Williamson JR: Effects of insulin and starvation on the metabolism
695
BROWN et al.
11.
12.
13.
14.
15.
16.
17.
Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017
18.
19.
20.
21.
696
of acetate and pyruvate by the perfused rat heart. Biochem J 93: 97,
1964
Williamson JR: Glycolytic control mechanisms. I. Inhibition of
glycolysis by acetate and pyruvate in the isolated perfused rat heart.
J Biol Chem 240: 2308, 1965
Randle PJ, England PJ, Denton RM: Control of the tricarboxylate
cycle and its interactions with glycolysis during acetate utilization
in rat heart. Biochem J 117: 677, 1970
Taegtmeyer H, Hems R, Krebs HA: Utilization of energy-providing
substrates in the isolated working rat heart. Biochem J 186: 701,
1980
Williamson DH, Hems R: Metabolism and function of ketone
bodies. In Bartley W, editor: Essays in cell metabolism. New York,
1970, John Wiley & Sons, p 257
Allan RM, Selwyn AP, Pike VW, Eakins MN, Maseri A: In vivo
experimental and clinical studies of normal and ischemic myocardium using "C-acetate. Circulation 62(suppl III): 111-74, 1980
(abst)
Allan RM, Pike VW, Maseri A, Selwyn AP: Myocardial metabolism of `C-acetate: experimental and patient studies. Circulation
64(suppl IV): IV-75, 1981 (abst)
Selwyn AP, Allan RM, Pike V, Fox K, Maseri A: Positive labeling
of ischemic myocardium: a new approach in patients with coronary
disease. Am J Cardiol 47: 481, 1981 (abst)
Bergmann SR, Clark RE, Sobel BE: An improved isolated heart
preparation for external assessment of myocardial metabolism. Am
J Physiol 236: H644, 1979
Benson JR, Woo DJ: Polymeric columns for liquid chromatography. J Chromatogr Sci 22: 386, 1984
Bligh EG, Dyer WJ: A rapid method of total lipid extraction and
purification. Can J Biochem Physiol 37: 911, 1959
Pike VW, Eakins MN, Allan RM, Selwyn AP: Preparation of
[ 1- "C] acetate - an agent for the study of myocardial metabolism
by positron emission tomography. Int J Appl Radiat Isot 33: 505,
1982
22. Wallenstein S, Zucker CL, Fleiss JL: Some statistical methods
useful in circulation research. Circ Res 47: 1, 1980
23. Brown MA, Myears DW, Marshall DR, Sobel BE, Bergmann SR:
Assessment of regional myocardial oxygen utilization by positron
tomography with "C-acetate. J Am Coll Cardiol 9: 73, 1987 (abst)
24. Bergmeyer HU, Moellering H: Enzymatische Bestimmung von
acetat. Biochem Z 344: 167, 1966
25. Bartelt U, Katterman R: Enzymatic determination of acetate in
serum. J Clin Chem Clin Biochem 23: 879, 1985
26. Harris P, Gloster J: The effects of acute hypoxia on lipid synthesis
in the rat heart. Cardiology 56: 43, 1971/72
27. Bailey IA, Gadian DG, Matthews PM, Radda GK, Seeley PJ:
Studies of metabolism in the isolated, perfused rat heart using 13C
NMR. FEBS Letters 123: 315, 1981
28. Neurohr KJ, Barrett EJ, Shulman RG: In vivo carbon-13 nuclear
magnetic resonance studies of heart metabolism. Proc Natl Acad Sci
USA 80: 1603, 1983
29. Lehninger AL: Principles of biochemistry. New York, 1982, Worth
Publishing Co., p 437
30. Bremer J, Osmundsen H: Fatty acid oxidation and its regulation.
In Numa S, editor: Fatty acid metabolism and its regulation.
Amsterdam, 1984, Elsevier Science Publishers, p 113
31. Bieber LL, Fiol CJ: Fatty acid and ketone metabolism. Circulation
72(suppl IV): IV-9, 1985
32. Stern JR, Coon MJ, Del Campillo A: Enzymatic breakdown and
synthesis of acetoacetate. Nature 171: 28, 1953
33. LaNoue K, Nicklas WJ, Williamson JR: Control of citric acid cycle
activity in rat heart mitochondria. J Biol Chem 245: 102, 1970
34. Whereat AF, Chan A: Effects of hypoxemia and acute coronary
occlusion on myocardial metabolism in dogs. Am J Physiol 223:
1398, 1972
35. Lindeneg 0, Mellemgaard K, Fabricius J, Lundquist F: Myocardial
utilization of acetate, lactate and free fatty acids after injection of
ethanol. Clin Sci 27: 427, 1964
CIRCULATION
Delineation of myocardial oxygen utilization with carbon-11-labeled acetate.
M Brown, D R Marshall, B E Sobel and S R Bergmann
Downloaded from http://circ.ahajournals.org/ by guest on June 16, 2017
Circulation. 1987;76:687-696
doi: 10.1161/01.CIR.76.3.687
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1987 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is located on
the World Wide Web at:
http://circ.ahajournals.org/content/76/3/687
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally
published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the
Editorial Office. Once the online version of the published article for which permission is being requested is
located, click Request Permissions in the middle column of the Web page under Services. Further
information about this process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/