Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
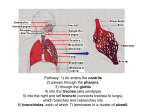
9/13/16 Respiratory system Dr. Dinithi Peiris Dept. of Zoology 1 Respiration n n n n Ventilation: Movement of air into and out of lungs External respiration: Gas exchange between air in lungs and blood Transport of oxygen and carbon dioxide in the blood Internal respiration: Gas exchange between the blood and tissues 2 1 9/13/16 Function of the respiratory system Regulation of blood pH: Altered by changing blood carbon dioxide levels Voice production: Movement of air past vocal folds makes sound and speech Olfaction: Smell occurs when airborne molecules drawn into nasal cavity Protection: Against microorganisms by preventing entry and removing them 3 Divisions of respiratory system n Upper tract n n Nose, pharynx and associated structures Lower tract n Larynx, trachea, bronchi, lungs 4 2 9/13/16 Nose & pharynx n Nose n n n External nose Nasal cavity n Functions n n n n n Passageway for air Cleans the air Humidifies, warms air Smell Along with paranasal sinuses are resonating chambers for speech Pharynx n Common opening for digestive and respiratory systems n Three regions n Nasopharynx n Oropharynx n Laryngopharynx 5 Larynx n Functions n Maintain an open passageway for air movement n Epiglottis and vestibular folds prevent swallowed material from moving into larynx n Vocal folds are primary source of sound production 6 3 9/13/16 Tracheobronchial Tree n Conducting zone n n n n Trachea to terminal bronchioles which is ciliated for removal of debris Passageway for air movement Cartilage holds tube system open and smooth muscle controls tube diameter Respiratory zone n n Respiratory bronchioles to alveoli Site for gas exchange 7 Airways Condition Air Before It Reaches The n Warm air to body temperature n Humidify air n Filter foreign material n Ciliated epithelial line the trachea and bronchi n Secrete mucus and dilute saline solution 8 4 9/13/16 Inspiration n n Air flows due to pressure gradients created by a pump. During inspiration the muscles of the thoracic cage contract, moving the rib cage n n Thoracic cavity expands (increased volume) pressure decreases Air movement ceases when pressure inside is equal to pressure outside 9 Inspiratory Muscles n n External intercostals and scalene muscles contract and pull ribs upward and out (expanding lungs Diaphragm, intercostals and scalenes are the primary muscles for breathing during rest. n During increased ventilation, other muscles of the chest and abdomen may be used 10 5 9/13/16 Expiration n n At the end of inspiration, impulses from somatic motor neurons to the inspiratory muscles cease and the muscles relax. Elastic recoil of the lungs returns the diaphragm and rib cage to their original relaxed position. n n Passive expiration Volume of thoracic cavity and lungs decreases and air pressure increases. 11 Exercise n n During exercise pressure differences become greater occurs when ventilation is greater than 30-40 breaths per minute Active expiration— n Uses intercostals muscles and abdominal muscles. 12 6 9/13/16 Ventilatory Muscles n n Internal intercostals muscles line the inside of the rib cage. n Contracted—pull ribs inward, reducing volume of the thoracic cavity. Internal and external intercostals acts as antagonistic muscle groups to alter the position and volume of the rib cage during ventilation. 13 Ventilatory Muscles n Diaphragm has no antagonistic forces (stays relaxed in active expiration), so abdominal muscles contract and pull the lower rib cage inward to decrease abdominal volume. n Displaced intestines and liver push the diaphragm up into the thoracic cavity, decreasing volume even more. 14 7 9/13/16 Breathing 15 Breathing 16 8 9/13/16 E expenditure for breathing n n n About 3-5% of the body s energy expenditure is used for quiet breathing. During exercise energy required for breathing increases substantially. Factors that influence amount of work needed for breathing: Compliance Resistance Surfactant 17 Compliance The ease with which the lungs and thorax expand during pressure changes n Greater compliance = greater ease of expansion n n § A high-compliance lung stretches easily and requires less force from the inspiratory muscles to stretch it Diseases which decrease compliance also increase the energy required for breathing; asthma, bronchitis, pulmonary edema 18 9 9/13/16 Resistance n n n n n Length of the system (constant) Viscosity of the substance flowing through the system (constant) Radius of the tubes (main variable) ~ 90% of airway resistance due to trachea and bronchi—rigid structures with smallest total crosssectional area (supported by cartilage and bone—so they don t move as easily). Mucus accumulation can increase resistance 19 Resistance n Bronchiole constriction (decrease air flow) 1. Parasympathetic N.S. (muscarinic R) 2. Histamine (paracrine) Bronchiole dilation (increase air flow) 1. Sympathetic N.S. (β2 R) 2. CO2 (paracrine) 20 10 9/13/16 Surfactant n Mixture of lipo-proteins n n n n E.g. DPPC (dipalmitoyl phosphoticylcholine) Alveoli have a natural tendency to collapse Surfactant helps prevent collapse by decreasing the surface tension If surfactant production decreases (pneumonia) high pressures may be required to maintain lung expansion 21 Pulmonary function tests n n n Quantifies air moving during quiet breathing and during maximum effort n Determine health of lungs Spirometer—instrument measures volume of air moving with each breath Obstructive lung disease is when air flow during expiration is diminished due to narrowing of the bronchioles n chronic bronchitis 22 11 9/13/16 Lung Volumes n n IRV n IC VC TV 4 Volumes 4 Capacities TLC Sum of 2 or more lung volumes ERV FRC RV RV Tidal Volume (TV) n IRV IC VC TV TLC Volume of air inspired and expired during normal quiet breathing ERV FRC RV RV 12 9/13/16 Inspiratory Reserve Volume (IRV) n IRV IC VC TV TLC ERV FRC RV RV The maximum amount of air that can be inhaled after a normal tidal volume inspiration Expiratory Reserve Volume (ERV) n IRV IC VC TV TLC Maximum amount of air that can be exhaled from the resting expiratory level ERV FRC RV RV 13 9/13/16 Residual Volume (RV) n IRV IC VC TV Volume of air remaining in the lungs at the end of maximum expiration TLC ERV FRC RV RV Vital Capacity (VC) n IRV IC VC TV TLC ERV n FRC RV n RV n Volume of air that can be exhaled from the lungs after a maximum inspiration FVC: when VC exhaled forcefully SVC: when VC is exhaled slowly VC = IRV + TV + ERV 14 9/13/16 Inspiratory Capacity (IC) n IRV IC VC TV TLC ERV FRC RV n Maximum amount of air that can be inhaled from the end of a tidal volume IC = IRV + TV RV Functional Residual Capacity (FRC) n IRV IC VC TV TLC n ERV FRC RV RV n Volume of air remaining in the lungs at the end of a TV expiration The elastic force of the chest wall is exactly balanced by the elastic force of the lungs FRC = ERV + RV 15 9/13/16 Total Lung Capacity (TLC) n IRV IC VC TV TLC ERV FRC RV n Volume of air in the lungs after a maximum inspiration TLC = IRV + TV + ERV + RV RV Pulmonary Function Tests n Evaluates 1 or more major aspects of the respiratory system n Lung volumes n Airway function n Gas exchange 16 9/13/16 Indications n n n n n Detect disease Evaluate extent and monitor course of disease Evaluate treatment Measure effects of exposures Assess risk for surgical procedures Total pulmonary ventilation n Total pulmonary ventilation = Ventilation rate X tidal volume 12 X 500 = 6 L / min n n Anatomical dead space (air remains in conducting air ways) = 150 ml Alveolar ventilation = ventilation rate X [tidal volume – dead space] 12 X [500 – 150] = 4200 ml / min 34 17 9/13/16 Total pulmonary ventilation n Physiological dead space = anatomical dead space – vol. of nonfunctional alveoli Normally, PDS = ADS n Respiratory disease- alveolar walls begin to degenerate and increase the PDS by 10X ADS 35 Minute volume / ventilation n n Minute volume- TV X RR (amount of gas inhaled and exhaled in one minute) Minute alveolar ventilation- amount of inspired gas available for gas exchange during one minute; (TV – DS) X RR 36 18 9/13/16 Blood flow n During rest some capillaries in the lungs are closed off n n blood diverted to other capillaries During exercise the closed capillaries will open maximum oxygenation 37 Atmospheric gases concentration n n n n n n Nitrogen- 78.62% or 597 torr Oxygen- 20.84% or 159 torr Carbon dioxide- 0.5% or 0.3 torr Water vapor- 6.2% or 3.7 torr Combined partial pressure of gases equal to 100% or 760 torr @ sea level Measured in mm HG; 1 torr = 1mm Hg 38 19 9/13/16 Atmospheric gases composition n Nitrogen- 74.9% or 569 torr n Oxygen- 13.7% or 104 torr n Carbon dioxide- 5.2% or 40 torr n Water vapor- 6.2% or 47 torr 39 Why difference of gases in the body? n n n Air entering body is humidified Exchange of O2 and CO2 between alveoli and blood Incomplete emptying of alveoli with expiration 40 20 9/13/16 Pulmonary circulation n n n Inspired gas enters the lungs; the respiratory system brings O2 to the blood and removes CO2 Blood low in O2 converges in the heart; passes through the R heart and into the lungs through the pulmonary artery Alveoli fill and empty 15,000X day 41 Pulmonary circulation n n n Alveoli filled with O2 have pressure gradient required for gas exchange O2 moves into capillaries and CO2 into alveoli to be exhaled Blood rich in flows into pulmonary veins L atrium, L ventricle, aorta and tissues 42 21 9/13/16 Partial pressures n n n Differences in partial pressures of O2 and CO2 on the two sides of the respiratory membrane (alveoli) result in diffusion of O2 into the blood and CO2 into the alveoli Capillary blood PO2 rises and PCO2 falls Stops when alveolar and capillary partial pressure equalize 43 Partial pressures n n n Exchange is so rapid that the blood leaving the lungs has nearly the same PO2 and PCO2 as alveolar air PO2 of blood returning to heart from veins is 40 mm Hg & alveoli is 100 mm Hg PCO2 of blood returning to heart from veins is 46 mm Hg & alveoli is 40 mm Hg 44 22 9/13/16 Partial pressures 45 What changes gas exchange? n Loss of surface area of alveoli or an increase in distance between alveoli decrease gas exchange in the alveoli n Hypoxia—too little oxygen in the cells. n Hypercapnia—elevated concentrations of CO2 46 23 9/13/16 Oxygen transport 1. O2 is slightly soluble in fluid—transported by 2 ways: Hemoglobin (Hb)—O2-binding protein in red blood cells n >98% of oxygen transported n Each hemoglobin molecule binds up to four oxygen molecules n HbO2 (oxyhemoglobin—hemoglobin bound to O2) n PO2 of cells determines how much oxygen will be release by Hb 47 Oxygen transport Dissolved in the plasma 2. n n n Only 3 mL of oxygen/liter of blood (5 L blood/minute) 15 mL of dissolved oxygen through the systemic tissues each minute not enough to meet the needs of the tissues (<10% of metabolic needs) 48 24 9/13/16 Oxygen dissociation curve Oxygen-hb dissociation curve shows that hb is almost completely saturated when P02 is 80 mm Hg or above. At lower partial pressures, the hb releases oxygen 49 Factors affecting dissociation curve A shift of the curve to the left because of n Increase in pH n Decrease in carbon dioxide n Decrease in temperature - increase in the ability of hemoglobin to hold oxygen n 2.3-bisphosphoglycerate increases the ability of hemoglobin to release oxygen 50 25 9/13/16 Factors affecting dissociation curve 51 Carbon dioxide Hydrogen Ion: •Increased H+ (decreased pH) increases H+ binding to Hb and reduces O2 affinity (HbO2+H+↔HbH++O2). • Carbon Dioxide (Bohr s effect): •Increased PCO2 increases CO2 binding to Hb and reduces O2 affinity (increased O2 delivery to tissue). •Increased PCO2 increases H+ and reduces O2 affinity 52 26 9/13/16 Bohr effect 53 Temperature effect 54 27 9/13/16 2,3-diphosphoglycerate No 2,3-DPG High amount of 2,3-DPG 55 Fetal curve 56 28 9/13/16 Shifting the curve 57 Transport of carbon dioxide Mainly 3 ways 1. Bicarbonate ions (70%) 2. In combination with blood proteins (23%) 3. In solution with plasma (7%) Haldane effect In tissue capillaries, carbon dioxide combines with water inside RBCs to form carbonic acid which dissociates to form bicarbonate ions and hydrogen ions 58 29 9/13/16 Haldane effect n In lung capillaries, bicarbonate ions and hydrogen ions move into RBCs and chloride ions move out. Bicarbonate ions combine with hydrogen ions to form carbonic acid. The carbonic acid is converted to carbon dioxide and water. The carbon dioxide diffuses out of the RBCs. 59 Carbon dioxide & Cl- movement 60 30 9/13/16 THE CHALLENGES OF HYPOXIA Barometric pressure decreases with alt. and partial pressure of O2 is a constant 20.9%. CO2 and water vapor dilute alveolar O2 . water vapor a function of T b, 47 mm Hg at normal T b eg. On Mt. Everest BP=253 mm Hg water vapor 47, CO2 8, O2 40! Saturation of Hb: 10,000 ft PO2 =110 %Hb sat = 90 20,000 ft PO2 = 73 %Hb sat = 73 30,000 ft PO2 = 26 %Hb sat = 24 61 CHEYNE STOKES BREATHING Alternating periods of slow and rapid breathing. Diffusion gradient for CO2 does not decrease with altitude, but the gradient for O2 diffusion decreases substantially. Small stimulus to breathing due to hypoxia is sufficient to reduce arterial O2 which results in decreased breathing. Decreased breathing increases & allows CO2 to build up again along with hypoxia. 62 31 9/13/16 THE EFFECTS OF HYPOXIA Acute effects: beginning at about 12,000 ft. drowsiness, mental and muscle fatigue, headache, nausea. Progress to twitching and seizures at 18,000 ft. and coma at 23,000 ft. Acclimation effects: Days to weeks -- increased pulmonary ventilation, increased hematocrit (erythropoietin mediated), increased diffusion capacity of lungs, increased capillarity. 63 THE EFFECTS OF HYPOXIA Acute mountain sickness (few hrs and couple of days after ascent): Cerebral edema and pulmonary edema (due to pulmonary vascular reactivity). Chronic mountain sickness (days to weeks after ascent): Exceptionally high hematocrit, high pulmonary arterial pressure, enlargement of right heart, fall in peripheral pressure, congestive heart failure. 64 32 9/13/16 Special adaptations 65 Diving Animals • • • Emperor bird dive up to 500m, cetaceans up to 1000m & sperm whale more than 1km. They exhale before diving. Contains massive organs filled with waxes; spermaceti oil – buoyancy Echolocations enable to distance, size & direction locate prey 66 33 9/13/16 Diving Animals • • • Humans : with short distance, large amount of blood in to thoracic cavity causing lung compressed. Diving animals : lungs & chests collapse as pressure increases. Diaphragm set oblique & hence lungs collapse to a fraction of the original size. Air is forced through windpipes & nasal cavity 67 Diving Animals • • Humans: hydrostatic neurological syndromes pressure causes Divers: inhibitory feedback on their CNS 68 34 9/13/16 Diving Animals • • • Humans: N partial pressure . N is absorbed in to arteries & tissues which reduce mental & motor capabilities. Decompression causes gases to expand; in arteries N bubbling occur. The Bends Divers: N tension is lower & concentration is limited by total lung collapse 69 Diving Animals • • Humans: brain anoxia due to diffusion of O in to arteries. Lung expansion causes further reduction in O tension. Further decrease in O tension will reduce pressure less than venous pressure Divers: reduce lung-blood gas exchange. Much lower partial pressures of O in their brains 70 35 9/13/16 DIVING BRADYCARDIA IN MARINE MAMMALS Heart rate falls during dive. Shut down of peripheral arteries results in blood flowing primarily to brain, eyes, and heart. Other tissues become hypometabolic At end of dive, heart rate returns, tissues are re-perfused, but oxygen payback is much less than what would have been total metabolic expenditure if seal had not dived. Diving bradycardia occurs in humans when face is submerged and it occurs during birth. 71 Diving Animals Other adaptations of divers: • Muscles act aerobically during diving. Lactic acid produced is diffuse out of muscles & burn out by the heart. • During short dives, they get enough O to burn off excess lactic acid. 72 36 9/13/16 High Altitude n Unlike high altitude animals, humans do not have left shifted- dissociation curve. 73 Regulation of respiration 74 37 9/13/16 Respiratory areas in brainstem n Medullary respiratory center n n n Dorsal groups stimulate the diaphragm Ventral groups stimulate the intercostal and abdominal muscles Carbon-dioxdie, oxygen and pH influence breathing 75 Medulla oblongata Dorsal resp. group ventral resp. group Somatic motor neurons Somatic motor neurons (Inspiration) (Expiration) Scalene external Mu. Int. Cost. Mu. Diaphragm Mu. Internal Int. Cost. Mu. Abdominal Mu. 76 38 9/13/16 senses Chemo receptors Mechano receptors Decrease oxygen Decrease pH Irritant receptors Increase PCO2 Hering-breuer reflex Exercise (TV > 1 L) Stretch receptors Signal brain to IB respiration 77 senses 78 39 9/13/16 Chemo receptors Peripheral chemo receptors Carotid & aortic bodies pH Central chemo receptors [CNS] PCO2 Cross BB barrier Resp. centers in the brain PO2 Converted to H+ & HCO3H+ Triggers chemo receptors PCO2 ventilation 79 40