Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Classification of mental disorders wikipedia , lookup
Diagnostic and Statistical Manual of Mental Disorders wikipedia , lookup
Cases of political abuse of psychiatry in the Soviet Union wikipedia , lookup
History of psychiatric institutions wikipedia , lookup
Dementia praecox wikipedia , lookup
Political abuse of psychiatry wikipedia , lookup
History of mental disorders wikipedia , lookup
Emergency psychiatry wikipedia , lookup
Dissociative identity disorder wikipedia , lookup
History of psychiatry wikipedia , lookup
Mental status examination wikipedia , lookup
Pyotr Gannushkin wikipedia , lookup
Abnormal psychology wikipedia , lookup
Controversy surrounding psychiatry wikipedia , lookup
Labeling theory wikipedia , lookup
Glossary of psychiatry wikipedia , lookup
Schizophrenia wikipedia , lookup
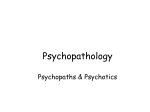
Effects of the Label "Schizophrenia" on Causal Attributions of Violence by Charles M. Boisvert and David Faust Research shows that labels can lead to biases in interpreting behavior. Darley and Gross (1983) found that a label of high versus low socioeconomic status altered undergraduates' perception of a child's academic functioning. In a study by Bromfield et al. (1988), teachers predicted less future success and urged less task persistence for a child labeled sexually abused versus an unlabeled child. Goodyear and Parish (1978) found that undergraduates viewed individuals seeking counseling more negatively when they were labeled a "patient" or "client" versus a "typical person." Research further suggests that biasing effects of labels may extend to professionals. In one study, nurses demonstrated more affective involvement and made fewer belittling statements in response to hypothetical statements made by "schizophrenia" patients versus "borderline personality disorder" patients (Gallop et al. 1989). Fryer and Cohen (1988) found that hospital staff rated patients labeled "psychiatric" as less likable and as having more unfavorable traits and fewer favorable traits than patients labeled "medical." In a study by Langer and Abelson (1974), psychoanalytic and behavioral therapists observed a videotape of a person labeled as either a patient or a job applicant. The psychoanalysts, unlike the behavior therapists, described the "patient" as significantly more disturbed than the "job applicant." Abstract We investigated the relation between the label of "schizophrenia" and causal attributions of violence. Undergraduates read 1 of 10 scenarios in which two variables were manipulated: a psychiatric label and environmental stress. The scenario described an employee who acted violently toward his boss. Subjects made causal attributions for the employee's behavior by completing an adapted version of the Causal Dimension Scale II. Subjects also completed a questionnaire designed to explore several issues concerning the effects of the schizophrenia label on perceptions of behavior. Contrary to the primary hypothesis, the schizophrenia label did not lead subjects to make significantly more personality causal attributions for violent behavior. With increasing environmental stress, subjects did make significantly fewer personality attributions. A follow-up study using practicing clinicians as subjects yielded similar findings. The results of these studies are discussed in light of perceived stereotypes of persons with schizophrenia and conceptual issues in attribution research. Key words: Attributions, Causal Dimension Scale II, stereotypes, violence. Schizophrenia Bulletin, 25(3):479-491,1999. Stereotypes Labels can exert powerful effects on perception; thus, to the extent they have the potential to facilitate understanding, they have the potential to impede it as well. Labels may be applied incorrectly, may describe pseudoconglomerations of symptoms versus genuine syndromes, or may lead to stereotyping or extreme tendencies to incorporate nonrelated phenomena under the label or diagnosis. As Mirowsky and Ross (1989) have argued, diagnosis may hinder understanding, treat attributes as entities, and ignore the structure of causal relations among the variables on which it is based. Various mechanisms or processes may be involved in the biasing effects of labels. Psychiatric labels may function as a stereotype through which behavior is narrowly interpreted. At the foundation of stereotypes is what the Chapmans (1967, 1969) identified as "illusory correlations," that is, the false association between two variables Reprint requests should be sent to Dr. CM. Boisvert, 1184 Mendon Rd., Cumberland, RI02864. 479 Schizophrenia Bulletin, Vol. 25, No. 3, 1999 CM. Boisvert and D. Faust or an overperception of that association. In the case of stereotyping, an illusory correlation represents the false pairing of person and behavior (Hamilton and Gifford 1976; Hamilton and Rose 1980). For example, we may believe that individuals with schizophrenia are violent far more often than members of the general population because of stereotypic perceptions of the mentally ill. However, epidemiological research shows that the association between mental disorder and violence is slight and may be present only when individuals are experiencing psychotic symptoms (Link et al. 1992; Monahan 1992). Others have suggested that schizophrenia predisposes a person to homicidal behavior particularly when the schizophrenia coexists with alcoholism (Eronen at al. 1996) and that symptom acuity in schizophrenia may contribute to an increased tendency toward criminality (Modestin andAmmann 1996). this phenomenon the "fundamental attribution error." Research, in fact, shows that professionals display dispositional biases (Batson 1975; Batson and Marz 1979; Batson et al. 1982; Jordan et al. 1988; Dumont 1993; Donnan and Pipes 1985). Limited research has examined the effects of labels on attribution. Snyder et al. (1976) found that undergraduate females made more personality attributions regarding the locus of a client's problem when told that the client was a chronic patient as opposed to someone being seen for the first time. In Shenkel et al.'s (1979) study, female social welfare students made more personality-based attributions when they had access to a pre-existing diagnosis. Snyder (1977) found that psychoanalytic therapists compared with behavioral therapists made significantly more personality attributions when identifying the locus of a person's problem when the person was labeled a "patient." However, when the person was labeled a "job applicant," no significant attributional differences were found between the two therapist groups (Snyder 1977). Pious and Zimbardo (1986) reported that psychoanalytic therapists compared with behavioral therapists were more likely to provide dispositional explanations for hypothetical client problems. In turn, much of the research that examined psychiatric labels focused on the negative effects experienced by the labeled person (Farina et al. 1971; Rosenhan 1973; Scheff 1974; Link 1987; Retzinger 1989; Parish et al. 1992) and the degree to which the labeled person is accepted socially (Bentz and Edgerton 1971; Loman and Larkin 1976; Link 1987; Link et al. 1987, 1989). Other research has examined attitudes toward the mentally ill (Phillips 1964; Segal 1978; Arkar and Eker 1994) and labeling theory as it relates to mental disorder (Link and Cullen 1990). Given the limited research that examines the impact of psychiatric labels on causal attributions and the potential importance of labels in shaping our judgments, this study was designed to explore the relation between the label of schizophrenia and causal attribution. We hypothesized that this label would lead individuals to make more personality causal attributions for violent behavior. We also hypothesized that as the strength of possible environmental causes for behavior increased, the degree to which individuals made personality causal attributions for violent behavior would decrease. This hypothesis was derived from the discounting principle in attribution theory, which states that "the social observer 'discounts' the role of any causal candidate in explaining an event to the extent that other plausible causes or determinants can be identified" (Ross 1977, p. 180). In Study 1, we examined our hypotheses using undergraduates as subjects. Study 2 extended this research to practicing clinicians. Labels and Causal Attribution To the extent that psychiatric labels lead the observer to focus on internal causes of behavior that are indeed internally caused and to otherwise focus externally, they shape judgment properly. Certainly, in some cases, behaviors may arise in substantial part from disturbances within the person. If identical twins reared apart and in highly contrasting environments both develop the belief that they are the Messiah, we are probably justified in believing that the problem, in good part, lies within them. Forming personality attributions for a behavior that is symptomatic of a person's illness may also be justified. For example, auditory hallucinations are experienced more often by people with schizophrenia than by members of the general population. Thus, one might well be justified in making internal causal attributions for this behavior (i.e., attributing the voices to the schizophrenia). However, if someone with schizophrenia is observed to be violent and is not currently experiencing psychotic symptoms, we probably would not be justified in attributing the behavior to the schizophrenia because those subjects without active psychotic symptoms apparently show no increased tendency toward violence compared with individuals without schizophrenia (Link et al. 1992; Monahan 1992). Research suggests that individuals are more inclined to attribute their own behavior to external (situational) causes, whereas an observer is more inclined to attribute the person's behavior to internal (dispositional) causes (Jones and Nisbett 1972; Ross 1977). According to Jones and Nisbett (1972), there is a "pervasive tendency for actors to attribute their actions to situational requirements, whereas observers tend to attribute the same actions to stable personal dispositions" (p. 2). Ross (1977) coined 480 Effects of the "Schizophrenia" Label Schizophrenia Bulletin, Vol. 25, No. 3, 1999 Study 1 Method Subjects. A total of 282 undergraduate students (127 males, 153 females, 2 subjects who did not indicate gender) from psychology classes at the University of Rhode Island participated voluntarily and received extra course credit for participating. Subjects were given a packet consisting of one page providing instructions and requesting demographic information, a one-page scenario, and a two-page questionnaire. Scenarios. The scenario described a divorced person who had two kids and a history of counseling and was an employee at a manufacturing company. In the scenario the employee was called into his boss's office. All information in the scenarios was kept the same except for (1) the presence or absence of a psychiatric label and (2) the level of environmental stress. Half the subjects evaluated an employee who had a label of schizophrenia, and half evaluated an employee who had no psychiatric label. Selection of the label condition. The label condition read as follows: "At the beginning of his treatment Mike underwent a series of interviews and thorough psychological, testing and was diagnosed with schizophrenia. Mike, fortunately, has not experienced psychotic symptoms since he was diagnosed." We selected the label of schizophrenia because of common stereotypes linking such disorders to dangerousness (Rabkin 1974; Link and Cullen 1986; Link et al. 1987; Wahl and Harman 1989). In addition, we selected a potentially strong but false association between a label and behavior (i.e., schizophrenia and violence). To be confident that the association was indeed false, we described the individual with schizophrenia in a nonacute stage of the disorder, and in particular in the absence of active, psychotic symptoms. This description was necessary because research suggests that under certain circumstances the association between schizophrenia and violence may be potentially true when individuals are experiencing acute psychotic episodes (Link et al. 1992; Monahan 1992). One disadvantage to describing the person in the scenario as not experiencing psychotic symptoms is that individuals with schizophrenia at such points, during which they may show relatively adequate functioning (Childers and Harding 1990; Ram et al. 1992; Eggers and Bunk 1997), may not and probably do not elicit the most powerful types of associations with violence. Furthermore, we needed to achieve a reasonable balance with the nonlabel condition. Describing an individual with acute psychotic features might lead the reader to adopt the label of schizophrenia whether explicitly mentioned or not. Thus, clearly the choice was a compromise between a powerful label that might, by itself, elicit stereotypic associations and an individual so labeled and 481 described in the vignette. Our description, while still potentially falling within the rubric of schizophrenia, certainly would appear to be a considerably less severe case and a higher functioning individual than is generally imagined. We did incorporate behavioral descriptors associated with schizophrenia, such as restricted social contacts and emotional isolation. Finally, we also indicated that the diagnosis had been firmly established to strengthen perceptions that the diagnosis was correct, even though some may have questioned this because of the "favorable characteristics" ascribed to the person in the scenario. It was expected that the schizophrenia label would lead subjects to shift attributions toward the person rather than the situation. Within each group, the level of environmental stress ranged from negligible to extreme along five conditions. In each condition, the boss conveyed different information to the employee. Subjects evaluated the employee's behavior of pushing the boss (see the appendix for a copy of the exact scenarios). Measures Causal Dimension Scale II. After reading a scenario, subjects completed an adapted version of the Causal Dimension Scale II (CDS-II; McAuley et al. 1992), a self-report instrument consisting of 12 items scored on a nine-point semantic differential scale. The CDS-II is designed to measure how individuals perceive causes along four factors: locus of causality, stability, external control, and personal control. The three questions per factor are rated on a scale from one to nine, and factor scores vary from 3 to 27. Factor analytic studies have yielded internal consistency ranging from 0.60 to 0.92 for the four factors; average internal consistencies are as follows: locus of causality, 0.67; stability, 0.67; personal control, 0.79; and external control, 0.82 (McAuley et al. 1992). The CDS-II was initially developed to assess personal causal attributions. An extensive literature review, as well as contact with a researcher directly involved in creating the CDS and CDS-II (D. Russell, personal communication, March 29, 1994), did not uncover any standardized scales for observer causal attributions. This led us to adopt the CDS-II to assess observer causal attributions. The authors were aware of only a few studies that examined observer causal attributions using the original CDS (Abraham 1987; Herr et al. 1990; Royce and Muehlke 1991). Also, a prominent attribution researcher believed that the CDS-II could be adapted to measure observer causal attributions (B. Weiner, personal communication, November 24, 1993). Finally, the CDS-II has been shown to be a more reliable and valid measure of causal dimensions than other methods (McAuley et al. Schizophrenia Bulletin, Vol. 25, No. 3, 1999 CM. Boisvert and D. Faust 1992). (A copy of the CDS-II adapted version can be obtained from the authors.) Exploratory questionnaire. Subjects also completed an exploratory questionnaire, developed by the researchers, that consisted of five items rated along a seven-point Likert scale. The items addressed the severity of the behavior, the degree to which the behavior was justified, the cause of the behavior, the degree to which the behavior was characteristic of the person, and the likelihood that the behavior had occurred previously. (A copy of the exploratory questionnaire is available from the authors.) ational than did subjects in any of the other groups; subjects in the negligible stress group attributed the cause of the employee's behavior to be significantly more dispositional than did subjects in any of the other groups; and subjects in the high stress group attributed the cause of the employee's behavior to be significantly more situational than did subjects in the mild stress group (see table 1). Follow-up univariate analysis of variance for variable ES yielded significant group differences for four of the five items from the exploratory questionnaire. These four items were "How would you rate the severity of Mike's [the protagonist in the scenario] behavior?" (F = 11.85, df = 4,270, p < 0.01); "How would you rate the degree to which Mike was justified in behaving as he did?" (F = 30.13, df = 4,270, p < 0.01); "How would you best explain the cause of Mike's behavior?" (F = 27.01, df = 4,270, p < 0.01); and "How likely is it that Mike has acted violently in other situations?" (F •= 12.03, df = 4,270, p < 0.01). Post hoc Tukey HSD tests at the p < 0.05 level for the exploratory questionnaire items indicated that with increasing environmental stress, subjects were less likely to rate violent behavior as severe, but more likely to rate the person as justified in acting violently, the cause of behavior as more situational, and the person as less likely to have a history of acting violently. Interestingly, subjects perceived violent behavior similarly regardless of the presence or absence of the schizophrenia label. Results did not support the primary hypothesis: the label of schizophrenia did not lead subjects to make more personality causal attributions for behavior. Results did support the secondary hypothesis: as the strength of possible environmental causes for behavior increased, the degree to which subjects made personality causal attributions for behavior decreased (figure 1). Several possibilities may explain the negative results for the primary hypothesis. The undergraduates in this study may have taken (or possibly were taking) psychology courses that "debiased" them and challenged common stereotypes concerning the relationship between mental illness and violence. In addition, professionals may be more inclined than laypersons to make personality attributions for another person's behavior, as some research has suggested (Batson 1975; Batson and Marz 1979). To explore the latter possibility, we extended our research to practicing clinicians. Procedure. The design was a randomized 2 X 5 factorial with the following variables: schizophrenia label (present or absent) and environmental stress (negligible, mild, moderate, high, or extreme). Subjects read and signed an informed consent and then were tested in small groups ranging from 2 to 30. Subjects read the scenario and answered first the CDS-II and then the exploratory questionnaire. Subjects were debriefed in small groups. Results. The results were analyzed using a 2 X 5 multivariate analysis of variance (MANOVA). A significant multivariate main effect was found for environmental stress (ES). Wilk's Lambda was 0.49, F = 5.75, df = 36,983, p < 0.01. The MANOVA analysis produced no other main or interaction effects, suggesting that the schizophrenia label, compared with no label, did not lead subjects to make more personality causal attributions for behavior. The power of our design to detect group differences for the label variable was approximately 0.96 (Cohen 1988). In addition, personality causal attributions for the schizophrenia label group, compared with the nolabel group, did not decrease at a reduced rate across the increasing levels of stress. Follow-up univariate analysis of variance for ES found significant group differences for three of the four CDS-n factors: the locus factor (F = 28.10, df = 4,270, p < 0.01), the external control factor (F = 3.46, df = 4,270, p < 0.01), and the personal control factor (F = 3.17, df = 4,270, p < 0.01). The stability factor did not yield significant results F = 1.59, df = 4,270, p > 0.05). Post hoc Tukey honestly significant difference (HSD) tests at the p < 0.05 level for the locus of causality factor (the researchers' primary interest) indicated that the extreme stress group and negligible stress group were significantly different from all the other groups, and the high stress group was significantly different from the mild and negligible stress groups. Regardless of the presence or absence of the schizophrenia label, subjects in the extreme environmental stress group attributed the cause of the employee's violent behavior to be significantly more situ- Study 2 Method Subjects. Eighty mental health professionals from a community mental health center in New England were randomly selected to participate in the study. This group 482 Schizophrenia Bulletin, Vol. 25, No. 3, 1999 Effects of the "Schizophrenia" Label Figure 1. Study 1 (Undergraduates): group means for CDS-II locus of causality factor Person 27 (A o O Situation Negligible Mild Moderate Stress Note.—CDS-II = Causal Dimension Scale II; SCZ = schizophrenia. 483 High Severe Schizophrenia Bulletin, Vol. 25, No. 3, 1999 CM. Boisvert and D. Faust was selected because of geographical convenience. Subjects were assured of anonymity, and participation was voluntary. Fifty-eight subjects returned the questionnaire: 4 psychiatrists, 10 registered nurses, 18 master'slevel clinicians, 2 clinicians with certificates of advanced graduate studies degrees, 20 bachelor's-level clinicians, 1 associate's-level clinician, 1 certified case manager, 1 person without a postsecondary degree, and 1 who did notindicate a degree. The subjects' years of clinical experience ranged from 1 to 10 or more years. Subjects received a packet consisting of one page providing instructions and requesting demographic information, a one-page scenario, a two-page questionnaire, and one page requesting professional information (i.e., degree, years of clinical experience, and theoretical orientation). Scenarios. The scenarios were identical to those used with the undergraduates. Half the subjects evaluated an employee who had a label of schizophrenia, and half evaluated an employee who had no psychiatric label. Within each of these groups, the level of stress ranged along two conditions (negligible or moderate). We chose only two stress conditions partly because we had access to a relatively small sample size. We chose the negligible condition because we believed it would elicit dispositional attributions more easily than the other stress conditions would (as evidenced by results from Study 1) and the moderate stress condition because we believed it was the most ambiguous and thus would be most sensitive to the effects of stereotypes (Hamilton et al. 1990). Procedure. The design was a randomized 2 X 2 factorial with the following variables: schizophrenia label (present or absent) and environmental stress (negligible or moderate). Subjects received the research packet via interoffice mail. They read and signed an informed con- sent and forwarded it to the researcher, then read a scenario and answered the CDS-II and the exploratory questionnaire. Subjects sent completed materials anonymously through interoffice mail to the researcher. Following the study, subjects received a summary of the results and were given the option of contacting the researcher to be debriefed. Results. The results were analyzed using a 2 X 2 MANOVA. A significant multivariate main effect was found for ES (Wilk's Lambda = 0.51, F = 5.01, df = 9,46, p < 0.01). The MANOVA analysis produced no other main or interaction effects, suggesting that practicing clinicians did not perceive the cause of violent behavior to be more dispositional than situational when the person was given a label of schizophrenia as opposed to no label. The power of our design to detect group differences for the label variable was approximately 0.36 (Cohen 1988). Follow-up univariate analysis of variance for ES found significant group differences for the locus factor (F = 26.10, df = 1,54, p < 0.01). The external control factor also yielded significant results (F = 9.79, df = 1,54, p < 0.01). Neither the personal control factor nor the stability factor yielded significant results (see table 2). Follow-up univariate analysis of variance for variable ES yielded significant group differences for two of the five items from the exploratory questionnaire. These two items were "How would you rate the degree to which Mike was justified in behaving as he did?" (F = 17.77, df = 1,54, p < 0.01); and "How would you best explain the cause of Mike's behavior?" (F = 6.42, df = 1,54, p < 0.01). These results suggested that with increasing environmental stress, professionals were more likely to rate the person as justified in acting violently and the cause of behavior as more situational. Table 1. Study 1 (Undergraduates): group mean scores on the CDS-II locus of causality factor Label condition No label Schizophrenia Stress Negligible Mild Moderate High Extreme CDS-II Mean Group mean SD Group mean SD 21.70 16.52 15.81 13.39 11.96 15.91 3.34 4.59 4.72 5.01 6.16 — 21.33 18.68 16.63 15.47 11.43 16.71 4.31 4.70 4.68 4.13 6.01 — CDS-II mean 21.521 17.60 16.30 14.432 11.703 — Note.—Scores range from 3, maximal situational attribution, to 27, maximal personal attribution. CDS-II = Causal Dimension Scale SD = standard deviation. 1 2 3 p < 0.05 for Negligible group > Mild, Moderate, High, and Extreme groups. p < 0.05 for High group < Mild and Negligible groups. p < 0.05 for Extreme group < High, Moderate, Mild, Negligible groups. 484 Schizophrenia Bulletin, Vol. 25, No. 3, 1999 Effects of the "Schizophrenia" Label Table 2. Study 2 (Clinicians): group mean scores on the CDS-II locus of causality factor Label condition Schizophrenia Stress Group mean No label Group mean SD SD CDS-II mean Negligible 20.24 20.86 4.82 20.531 4.10 Moderate 13.58 16.27 3.53 4.03 14.931 CDS-II Mean 16.91 18.55 Note.—Scores range from 3, maximal situational attribution, to 27, maximal personal attribution. CDS-II = Causal Dimension Scale SD = standard deviation. 1 p < 0.01 for Negligible group > Moderate group. nonbiased judgment in the face of stimuli (e.g., the label of schizophrenia) potentially expected to create biasing effects. However, as noted, our particular vignette description of a person with schizophrenia may have been less likely to elicit strong stereotypes. Regardless of the presence or absence of the schizophrenia label, subjects in the moderate environmental stress group, compared with the negligible stress group, attributed the cause of the employee's violent behavior to be significantly more situational. These results suggest that as the strength of environmental causes for behavior increased, subjects made fewer personality causal attributions (figure 2). However, the results did not suggest that the label of schizophrenia led practicing clinicians to make more personality causal attributions. Methodological Concerns. The null result for the label variable, on the other hand, may have resulted from methodological limitations, which raises issues related to experimental design and measurement; in particular, is the analogue approach, which measures perceptions of hypothetical situations, a proper test of the research hypotheses? However, analogue approaches of the type applied in this study are commonly used to investigate the effects of labels on clinical judgment (Link 1987; Link et al. 1987; Loring and Powell 1988; Penn et al. 1994). Moreover, a clear trend was detected regarding the ES variable, indicating that our attempts to manipulate this variable were successful. Nevertheless, reactions, stereotypic or otherwise, that are elicited from an analogue study may be different from reactions elicited in more naturalistic settings. Thus, although our findings suggest that some stereotypes of schizophrenia may be attenuated under certain circumstances and given specific measurement conditions (e.g., using vignettes to elicit perceptions of causality), generalizing the result to naturalistic conditions and circumstances across which they apply requires further study. Discussion The significant main effect for environmental stress in both studies suggests that attempts to manipulate perceived level of stress were successful. Overall, there was a clear and consistent trend toward increasing situational attributions with increasing degrees of environmental stress. At the same time, both the undergraduates and the practicing clinicians perceived the situation as a substantial contributor to behavior even when the degree of situational stress was mild, which may suggest something about attributions toward and attitudes about violent behavior. Extreme environmental stress was not required for subjects to believe that violent behavior was justified. Although environmental stress influenced the degree to which undergraduates and practicing clinicians made personality causal attributions, the schizophrenia label did not; nor was there evidence for an interaction between the two variables. The null result for the label variable may reflect the true state of nature; that is, at least in the context studied, the label of schizophrenia may not distort or bias attribution. Such a result runs contrary to other research suggesting that psychiatric labels skew lay and, particularly, professional judgment. The findings in this study raise the possibility that judgmental biases of this type might not be as broad or pervasive as is sometimes assumed. This study, then, may provide a contrary example of proper or Another possible reason for the null result is that the manipulation of the label may not have been strong enough to yield group differences. Even in the no-label condition, subjects may have perceived the person as a "mental patient" simply by virtue of involvement in psychotherapy. Past studies, in fact, have shown that labels such as "patient" or "client" can be stigmatizing (Parish et al. 1992) and that information such as "a history of treatment" can lead to dispositional biases (Snyder et al. 1976). However, the subjects, at least in making causal attributions for violent behavior, did not differentiate significantly between a "maladjusted divorced person" and someone "diagnosed with schizophrenia." 485 CM. Boisvert and D. Faust Schizophrenia Bulletin, Vol. 25, No. 3, 1999 Figure 2. Study 2 (Clinicians): group means for CDS-II locus of causality factor Person 27 24 • scz El No Label 21 18 15 tf) o o 12 6 ' '• ^^B ^^B '::;;:^ ^ ^ ^ H " " ^ •^^B ^ Situation ^ ^ ^ ^ ^ ^ ^ ^ ^ "•••• T' '.'• , • . . / ; : . • .;::;.• ..,;:,.•:• , ; , HBI1MB Moderate '.At/^i..t..Ai ° Negligible Stress Note.—CDS-II = Causal Dimension Scale II; SCZ = schizophrenia. 486 < Schizophrenia Bulletin, Vol. 25, No. 3,1999 Effects of the "Schizophrenia" Label with schizophrenia or borderline personality disorder to dispositional factors. However, these dispositional attributions may represent different judgments that are not easily distinguishable if measured on a dichotomous situationaldispositional scale. Furthermore, these dispositional attributions may be influenced by the degree to which clinicians perceive the person to have control over the behavior. For example, clinicians may understand various features of schizophrenia as a biological problem, certainly residing in the person but over which the person has little control. Alternatively, clinicians may understand borderline personality disorder as a personality problem, also residing within the person but over which the person does have control. Thus, clinicians may be less inclined to evoke personality attributions to explain the behavior of an individual with schizophrenia than to explain the behavior of an individual with borderline personality disorder. Penn et al. (1994) similarly suggested that labels may be stigmatizing to the extent that they suggest the person has control over the behavior and subsequently could be "blamed" for the behavior. As some research has suggested, attributional biases (differences) may be modified by other variables. For example, professionals' theoretical orientation can contribute to attributional biases (Snyder 1977; Pious and Zimbardo 1986) and may influence attributions of responsibility for problems (McGovern et al. 1986). Considering past attribution research and preliminary findings from this study, it seems reasonable to suggest that causal attributions ultimately may be arrived at through an understanding of dispositional and situational factors as phenomena that are not static, dichotomized, and easily predictable occurrences, but fluid, dynamic, and influenced potentially by multiple variables (e.g., psychiatric labels, setting, particular behavior, theoretical orientation, sociocultural factors). Research findings suggesting that professionals display attributional biases are based on only a few studies (Batson 1975; Batson and Marz 1979; Donnan and Pipes 1985). Additionally, in the context of these studies, the claim of "professional bias" may be questionable. Professionals may be justified in attributing a client's problem to dispositional characteristics, particularly when given ambiguous information (Davis 1979). A Bayesian would argue that the prior odds should inform the appraisal of information, and base rates for dispositional characteristics need to be considered before concluding that clinicians display dispositional biases. For example, a clinician may be asked to identify the cause of a client's social withdrawal, which may be co-occurring with stressful events. If the client has a diagnosis of schizophrenia and if social withdrawal is far more common in those with schizophrenia in comparison to those without this label, Schizophrenia Stereotypes. It is notable that the label of schizophrenia itself, compared with no label, did not significantly alter subjects' causal attributions of violence. Such a finding raises questions about whether the label of schizophrenia, by itself, is enough to evoke stereotypes and to what extent information beyond the label contributes to stereotypic perceptions. Penn et al. (1994) studied the effect that various levels of information about a recovered person with mental illness had on emotional and social reactions to that person. They found that those who had had previous contact with the mentally ill perceived them as less dangerous and that descriptions of previous symptomatology in the acute phase of schizophrenia were more stigmatizing than the label of schizophrenia alone. The apparent public stereotype of the mentally ill as dangerous (Segal 1978; Link and Cullen 1986; Landrine 1992; Monahan 1992) may have attenuated over recent years (Skinner et al. 1995), possibly as a result of the community mental health and consumer-organized movements to counter erroneous perceptions of the mentally ill. The "dangerousness" stereotype may have been mollified in the study because the person in the scenario was assuming an acceptable role in society (i.e., employee), possibly a role not perceived as stereotypic of an individual with schizophrenia. Some research suggests, indeed, that stereotypes of the mentally ill are evoked more easily when an individual is observed in a role presumably associated with the mentally ill (Segal 1978). In our study we might have found a label effect had we described the person with schizophrenia as experiencing psychotic symptoms and distress. However, such a description would have added surplus meaning connecting the individual to violent behavior, and subjects may have been more justified in attributing the behavior to the person (see Link et al. 1992; Monahan 1992; Junginger 1996). Moreover, we recognize at the same time that our description may have vitiated some stereotypes of schizophrenia and that other descriptions of a person with schizophrenia may not have aroused the same perceptions. Ultimately, subjects may have perceived the person with schizophrenia as relatively unimpaired compared with the average person with schizophrenia, and consequently were less inclined to make personality attributions for behavior. Conceptual Issues in Attribution Research. Causal attributions may, in fact, represent cognitive processes that are not understood easily through traditional concepts (i.e., the fundamental attribution error) or easily measured through the available methodology (Solomon 1978; Miller et al. 1981; Watkins 1986; White 1991). For example, clinicians could attribute the behavior of someone 487 Schizophrenia Bulletin, Vol. 25, No. 3, 1999 CM. Boisvert and D. Faust then the clinician would be justified in shifting attributions about social withdrawal in the direction of individual versus situational factors. Research suggesting that professionals display fundamental attributional errors may be inconclusive and possibly misleading. Future Directions. Our study raises several questions about perceived stereotypes of people with schizophrenia and the potential impact of labels in shaping clinical judgment. Our findings suggest that the label schizophrenia, alone, may not evoke stereotypic perceptions of violence. In addition, some stereotypic perceptions may be mollified when a supposed stereotypic label (e.g., schizophrenia) exists in the presence of more favorable characteristics (e.g., a work history, providing for a family). Although it would be naive to conclude that stereotypes of people with schizophrenia do not exist, our findings suggest that stereotypic perceptions may be influenced by several variables. In some cases the psychiatric label may be one of those variables, but in other situations, the label alone may be insufficient to evoke a negative stereotype. Moreover, given our findings and the dearth of research examining the relation between psychiatric labels and causal attribution, research is needed to clarify the extent to which psychiatric labels influence causal analysis. For example, attribution research may need to include more detailed inquiries into the cognitive activity of the perceiver; that is, it may be necessary to assess individuals' decision processes underlying causal attributions. Although self-reports of causal attributions or cue utilization may be prone to error (Nisbett and Wilson 1977), methods are available for analyzing and comparing subjective impressions with objective measures of cue utilization (Faust 1984). Research is also needed to develop a technology to assess observer causal attributions. A first step may be to examine whether the CDS-II can be adapted for this purpose. Considering the potential impact of stereotypic perceptions and judgments on causal analysis and clinical decision making, research on stereotypes of schizophrenia seems worth pursuing. In clinical matters in which stereotypic perceptions of people with schizophrenia are likely to influence the selection of treatment, altering such perceptions becomes critical, particularly when it leads to improved treatment outcomes. After all, if it is not really the patient's schizophrenia but rather the loss of a job that caused his or her agitation, then vocational counseling rather than psychotropic medication may be indicated. Although our findings are hopeful in their suggestion that stereotypic perceptions of people with schizophrenia as more violent than members of the general population may not be evoked in some situations, this does not mean that the label conveys no stereotyped information. The 488 label may evoke other stereotypes (e.g., "unemployable," "dependent," "stricken") that influence various perceptions and reactions, including clinicians' selection of treatment. Furthermore, not only psychiatric labels, but other descriptors (e.g., "mental patient," "on psychiatric medication," "work history") may share a powerful role in influencing and altering stereotypes and thus also deserve our attention. Appendix Scenarios. Mike has been employed at Fisher Manufacturing as a line worker for the past 6 years. Although Mike has had conflicts with his coworkers and has been described as distant and moody, his job performance has been satisfactory. Mike has maintained a good work attendance record despite taking a 3-week leave of absence 4 years ago because of severe marital problems, which eventuated in a divorce. Mike sought counseling with a psychologist following his divorce, continued in treatment for 6 months, and came to accept his divorce. LABEL: At the beginning of his treatment Mike underwent a series of interviews and thorough psychological testing and was diagnosed with schizophrenia. Mike, fortunately, has not experienced psychotic symptoms since he was diagnosed. Mike's ex-wife has custody of their two children, a daughter Melissa, age 5, and a son Jeremy, age 7. Mike, however, sees his children regularly and is a good provider for them. Mike's social life is limited; except for membership in the Elks Club, he has few outside interests. Fisher Manufacturing has a history of episodic financial difficulties, and occasionally employees have been asked to take a cut in pay or have been laid off temporarily. Upon his arrival at work this morning, Mike's supervisor called him into his office. Mike found this unusual as his supervisor had never asked to meet with him at an unscheduled time. Mike did not question his supervisor and came to his office immediately following his supervisor's request. Upon entering his supervisor's office, Mike noticed that his personnel file was on his supervisor's desk. Mike's supervisor invited him to sit down and informed him that: [one of the five stress conditions followed; see below]. Mike then grabbed his supervisor by the shirt and forcibly threw him against the wall hard enough to cause a minor concussion. The Five Stress Conditions 1. Negligible stress: Despite recent layoffs, he would not be laid off. In fact, because his work performance had been so good, he would be receiving a raise, but it would be delayed a few weeks because of problems at the com- Effects of the "Schizophrenia" Label Schizophrenia Bulletin, Vol. 25, No. 3, 1999 pany. Mike then stood up and asked if there was any way he could receive his raise sooner. His supervisor told him that there were limits to what he could do. 2. Mild stress: He would be terminated very soon. His supervisor told him that he was sorry about the circumstances and that the company would do what it could to help him find another job. Mike then stood up and asked if he had any options at this time. His supervisor informed him that unfortunately the decision had been made and there was nothing he could do. 3. Moderate stress: He would be terminated very soon. His supervisor told him that he was lucky that he lasted this long with the company and that he was never considered to be a particularly good worker anyway. Mike then stood up and asked if he had any options at this time. His supervisor became noticeably angry, glared directly at Mike, stood up, clenched his fist, and told him that if he questioned him further he would be sorry. 4. High stress: He would be terminated very soon. His supervisor told him that he was lucky that he lasted this long with the company and that he was never considered to be a particularly good worker anyway. Mike then stood up and asked if he had any options at this time. His supervisor became noticeably angry, glared directly at Mike, stood up, clenched his fist, told him that if he questioned him further he would be sorry, and pushed Mike back into his chair. 5. Extreme stress: He would be terminated very soon. His supervisor told him that he was lucky that he lasted this long with the company and that he was never considered to be a particularly worker anyway. Mike then stood up and asked if he had any options at this time. His supervisor became noticeably angry, glared directly at Mike, stood up, clenched his fist, told him that if he questioned him further he would be sorry, grabbed Mike by the throat and began choking him until his face turned red, and pushed Mike back into his chair. Mike then proceeded to leave the room, but his supervisor approached the doorway quickly and stood guarding the door. References Abraham, I.L. Causal analysis in the clinical inference of depression: The influence of general cognitions about causality. Journal of Human Behavior and Learning, 4:61-66, 1987. Batson, CD., and Marz, B. Dispositional bias in trained therapists' diagnosis: Does it exist? Journal of Applied Social Psychology, 9:476-489, 1979. Batson, C D . ; O'Quin, K.; and Pych, V. An attribution theory analysis of trained helpers' inferences about clients' needs. In: Wills, T.A., ed. Basic Processes in Helping Relationships. New York, NY: Academic Press, 1982. pp. 59-80. Bentz, K.W., and Edgerton, W.J. The consequences of labeling a person mentally ill. Social Psychiatry, 6:29-33, 1971. Bromfield, R.; Bromfield, D.; and Weiss, B. Influence of the sexually abused label on perceptions of a child's failure. Journal of Educational Research, 82:96-98, 1988. Chapman, L.J., and Chapman, J.P. Genesis of popular but erroneous psychodiagnostic observations. Journal of Abnormal Psychology, 72:193-204, 1967. Chapman, L.J., and Chapman, J.P. Illusory correlation as an obstacle to the use of valid psychodiagnostic signs. Journal of Abnormal Psychology, 74:271-280, 1969. Childers, S.E., and Harding, C M . Gender, premorbid social functioning, and long-term outcome in DSM-IH schizophrenia. Schizophrenia Bulletin, 16:309-318, 1990. Cohen, J. Statistical power analysts for the behavioral sciences. 2nd ed. Hillside, NJ: Lawrence Erlbaum Associates, 1988. Darley, J.M., and Gross, P.H. A hypothesis-confirming bias in labeling effects. Journal of Personality and Social Psychology, 44:20-33, 1983. Davis, D.A. What's in a name? A Bayesian rethinking of attributional biases in clinical judgment. Journal of Consulting and Clinical Psychology, 47:1109-1114, 1979. Donnan, H.H., and Pipes, R.B. Counselor trainees' explanations of behavior: Attributions to traits, situations, and interactions. Journal of Clinical Psychology, 41:729-733, 1985. Dumont, F. Inferential heuristics in clinical problem formulation: Selective review of their strengths and weaknesses. Professional Psychology: Research and Practice, 24:196-205, 1993. Eggers, C , and Bunk, D. The long-term course of childhood-onset schizophrenia: A 42-year followup. Schizophrenia Bulletin, 23:105-117, 1997. Eronen, M.; Tiihonen, J.; and Hakola, P. Schizophrenia Arkar, H., and Eker, D. Effect of psychiatric labels on attitudes toward mental illness in a Turkish sample. International Journal of Social Psychology, 40:205-213, 1994. and homicidal behavior. Schizophrenia Bulletin, 22:83-89, 1996. Farina, A.; Gliha, D.; Boudreau, L.A.; Allen, J.G.; and Sherman, M. Mental illness and the impact of believing others know about it. Journal of Abnormal Psychology, 77:1-5, 1971. Batson, C D . Attribution as a mediator of bias in helping. Journal of Personality and Social Psychology, 32:455466, 1975. 489 Schizophrenia Bulletin, Vol. 25, No. 3, 1999 CM. Boisvert and D. Faust Faust, D. The Limits of Scientific Reasoning. Minneapolis, MN: University of Minnesota Press, 1984. Link, B.G.; Andrews, H.; and Cullen, F.T. The violent and illegal behavior of mental patients reconsidered. American Sociological Review, 57:275-292, 1992. Fryer, J.H., and Cohen, L. Effects of labeling patients "psychiatric" or "medical": Favorability of traits ascribed by hospital staff. Psychological Reports, 62:779-793, 1988. Gallop, R.; Lancee, W.J.; and Garfinkel, P. How nursing staff respond to the label "borderline personality disorder." Hospital and Community Psychiatry, 40:815-819, 1989. Goodyear, R.K., and Parish, T.S. Perceived attributes of the terms client, patient, and typical person. Journal of Counseling Psychology, 25:356-358, 1978. Link, B.G., and Cullen, F.T. Contact with the mentally ill and perceptions of how dangerous they are. Journal of Health and Social Behavior, 27:289-303, 1986. Link, B.G., and Cullen, F.T. The labeling theory of mental disorder: A review of the evidence. In: Greenley, J.R., ed. Research in Community and Mental Health, Vol. 6. Greenwich, CT: JAI Press, 1990. pp. 203-233. Link, B.G.; Cullen, F T ; Frank, J.; and Wozniak, J.F. The social rejection of former mental patients: Understanding why labels matter. American Journal of Sociology, 92:1461-1500, 1987. Hamilton, D.L., and Gifford, R.K. Illusory correlation in interpersonal perception: A cognitive basis of stereotypic judgments. Journal of Experimental Social Psychology, 12:392^07, 1976. Link, B.G.; Struening, E.; Cullen, F T ; Shrout, P.E.; and Dohrenwend, B.P. A modified labeling theory approach to mental disorders: An empirical assessment. American Sociological Review, 54:400-423, 1989. Hamilton, D.L., and Rose, T.L. Illusory correlation and the maintenance of stereotypic beliefs. Journal of Personality and Social Psychology, 39:832-845, 1980. Hamilton, D.L.; Sherman, S.J.; and Ruvolo, C M . Stereotype-based expectancies: Effects on information processing and social behavior. Journal of Social Issues, 46:35-60, 1990. Loman, A.L., and Larkin, W.E. Rejection of the mentally ill: An experiment in labeling. Sociological Quarterly, 17:555-560, 1976. Loring, M., and Powell, B. Gender, race, and DSM-III: A study of the objectivity of psychiatric diagnostic behavior. Journal of Health and Social Behavior, 29:1-22, 1988. Herr, P.N.; Perkins, D.V.; and Whitley, B.E. Interpersonal reactions to a depressed, schizotypal, or normal individual: An attributional perspective. Journal of Research in Personality, 24:454-467, 1990. McAuley, E.; Duncan, T.E.; and Russell, D.W. Measuring causal attributions: The revised Causal Dimension Scale (CDS-II). Personality and Social Psychology Bulletin, 18:566-573, 1992. Jones, E.E., and Nisbett, R.E. The actor and observer: Divergent perceptions of the causes of behavior. In: Jones, E.E.; Kanouse, D.E.; Kelley, H.H.; Nisbett, R.E.; Valins, S.; and Weiner, B., eds. Attribution: Perceiving the Causes of Behavior. Morristown, NJ: General Learning Press, 1972. pp. 79-94. McGovern, M.P.; Newman, F.L.; and Kopta, S.M. Metatheoretical assumptions and psychotherapy orientation: Clinician attributions of patients' problem causality and responsibility for treatment outcome. Journal of Consulting and Clinical Psychology, 54:476-481, 1986. Jordan, J.S.; Harvey, J.H.; and Weary, G. Attributional biases in clinical decision making. In: Turk, D.C., and Salovey, P., eds. Reasoning, Inference, and Judgment in Clinical Psychology. New York, NY: The Free Press, 1988. pp. 90-106. Miller, F.D.; Smith, E.R.; and Uleman, J. Measurement and interpretation of situational and dispositional attributions. Journal of Experimental Social Psychology, 17:80-95, 1981. Junginger, J. Psychosis and violence: The case for a content analysis of psychotic experience. Schizophrenia Bulletin, 22(l):91-103, 1996. Mirowsky, J., and Ross, C.E. Psychiatric diagnosis as reified measurement. Journal of Health and Social Behavior, 30:11-25, 1989. Landrine, H. The Politics of Madness. New York, NY: Peter Lang Publishing, Inc., 1992. Modestin, J., and Ammann, R. Mental disorder and criminality: Male schizophrenia. Schizophrenia Bulletin, 22(l):69-82, 1996. Langer, E.J., and Abelson, R.P. A patient by another name...: Clinician group difference in labeling bias. Journal of Consulting and Clinical Psychology, 42:4-9, 1974. Monahan, J. Mental disorder and violent behavior: Perceptions and evidence. American Psychologist, 47:511-521,1992. Link, B.G. Understanding labeling effects in the area of mental disorders: An assessment of the effects of expecta- Nisbett, R.E., and Wilson, T.D. The halo effect: Evidence for unconscious alteration of judgments. Journal of Personality and Social Psychology, 35:250-256, 1977. tions of rejection. American Sociological Review, 52:96-112, 1987. 490 Effects of the "Schizophrenia" Label Schizophrenia Bulletin, Vol. 25, No. 3,1999 Parish, T.S.; Grosdidier, L.M.; and Emmerson, G.J. Psychiatrogenic effects of counseling: Self-concepts and the negative effects of labeling. College Student Journal, 26:202-204, 1992. Penn, D.L.; Guynan, K.; Daily, T.; Spaulding, W.D.; Garbin, C.P.; and Sullivan, M. Dispelling the stigma of schizophrenia: What sort of information is best? Schizophrenia Bulletin, 20:567-574, 1994. Segal, S.P. Attitudes toward the mentally ill: A review. Social Work, 23:211-217, 1978. Shenkel, R.J.; Snyder, C.R.; Batson, C D . ; and Clark, G.M. Effects of prior diagnostic information on clinicians' causal attributions of a client's problems. Journal of Consulting and Clinical Psychology, 47:404-406, 1979. Phillips, D.L. Rejection of the mentally ill: The influence of behavior and sex. American Sociological Review, 29:679-687, 1964. Skinner, L.J.; Berry, K.K.; Griffith, S.E.; and Byers, B. Generalizability and specificity of the stigma associated with the mental illness label: A reconsideration twentyfive years later. Journal of Community Psychology, 23:3-17, 1995. Pious, S., and Zimbardo, P.G. Attributional biases among clinicians: A comparison of psychoanalysts and behavior therapists. Journal of Consulting and Clinical Psychology, 54:568-570, 1986. Snyder, C.R. "A patient by another name" revisited: Maladjustment or attributional locus of problem? Journal of Consulting and Clinical Psychology, 45:101-103, 1977. Rabkin, J. Public attitudes toward mental illness: A review of the literature. Schizophrenia Bulletin, 1 (Experimental Issue No. 10):9-33, 1974. Snyder, C.R.; Shenkel, R.J.; and Schmidt, A. Effects of role perspective and client psychiatric history on locus of problem. Journal of Consulting and Clinical Psychology, 44:467-472, 1976. Ram, R.; Bromet, E.J.; Eaton, W.W.; Pato, C ; and Schwartz, J.E. The natural course of schizophrenia: A review of first-admission studies. Schizophrenia Bulletin, 18:185-207,1992. Solomon, S. Measuring dispositional and situational attributions. Personality and Social Psychology Bulletin, 4:589-594, 1978. Wahl, O.F., and Harman, C.R. Family views of stigma. Schizophrenia Bulletin, 15:131-139, 1989. Retzinger, S.M. A theory of mental illness: Integrating social and emotional aspects. Psychiatry, 52:325-335, 1989. Watkins, D. Assessing causal dimensions. Australian Psychologist, 21:467-472,1986. Rosenhan, D.L. On being sane in insane places. Science, 179:250-258, 1973. White, P.A. Ambiguity in the internal/external distinction in causal attribution. Journal of Experimental Social Psychology, 27:259-270, 1991. Ross, L. The intuitive psychologist and his shortcomings: Distortions in the attribution process. In: Berkowitz, L., ed. Advances in Experimental Social Psychology, Vol. 10. New York, NY: Academic Press, 1977. pp. 173-220. The Authors Royce, W.S., and Muehlke, C.V. Therapists' causal attributions of clients' problems and selection of intervention strategies. Psychological Reports, 68:379-386, 1991. Charles M. Boisvert, Ph.D., received his doctorate in Clinical Psychology and David Faust, Ph.D., is a Professor of Psychology at the University of Rhode Island, Kingston, RI. Scheff, T.J. The labeling theory of mental illness. American Sociological Review, 39:444-452, 1974. 491