Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Management of acute coronary syndrome wikipedia , lookup
Coronary artery disease wikipedia , lookup
Cardiac surgery wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Myocardial infarction wikipedia , lookup
Jatene procedure wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
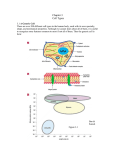
Blood Chapter 16 Composition of Blood • Body’s only fluid tissue • It is composed of liquid plasma (54%) and formed elements (Cells) (46%) • Erythrocytes, or red blood cells (RBCs)- 45% • Leukocytes, or white blood cells (WBCs) and Platelets (1%) Physical Characteristics and Volume • The pH of blood is 7.35–7.45 • Temperature is 38C, slightly higher than “normal” body temperature • 5–6 L for males, and 4–5 L for females Color depends on its oxygen content. – Bright red when oxygenated (e.g., arterial blood) – Dark red when deoxygenated (e.g., venous blood). Without O2 With O2 Functions of Blood • Distribution – Gases, nutrients, signaling molecules, wastes, heat • Regulation – Body fluid volume – Body fluid pH – Body T° – Electrolyte levels • Protection from pathogens and fluid loss Body Temperature Regulation Notice how the distribution of blood varies with temperature. Under warm conditions, blood is shunted to the surface so that heat can radiate away. Under cold conditions, blood (and thus heat) are conserved within the core of the body. Plasma • 55% of blood • Mostly water • Dissolved Solutes Contains: – Proteins – Electrolytes – Gases – Nutrients – Wastes – Signaling molecules – Buffers Some of the Plasma Proteins – Albumin • 60% of plasma proteins. • Produced by the liver. • Primary function is to maintain the osmotic pressure of the plasma. Also involved in transport of certain substances (steroids, bilirubin). – Globulins • Some globulins are produced in the liver and are transport proteins for lipids, metal ions, and fat-soluble vitamins. • Other globulins are produced by plasma cells (a type of leukocyte) during the immune response. These globulins are also known as antibodies. – Clotting proteins • Most produced in the liver. • Two important examples are prothrombin and fibrinogen. Erythrocytes (RBCs) • • • • • • • Small Biconcave disks Anucleate No organelles Stuffed with hemoglobin Transport O2 4-6 million per μL of blood Figure 16.3 Hemoglobin • Note the 4 heme groups associated with the 4 polypeptide chains of the hemoglobin protein. Each has an iron in its center. How many O2 molecules could a single hemoglobin carry? Hemopoiesis • Blood cell formation = hemopoiesis • All blood cell production occurs in the red bone marrow, which is found in the: – Axial skeleton – Pelvic and pectoral girdles – Proximal epiphyses of the humerus and femurs. • What must happen as a hemocytoblast differentiates into an RBC? • - What must be lost? • - What must be made? • - What must change? RBC Production RBC Lifespan Born in the red marrow Circulate for 120d Swallowed by a macrophage (usually in the spleen) Hemoglobin Heme Globin Iron Bilirubin Carried by albumin to the liver Carried by transferrin to the liver Secreted into the small intestine as part of bile Stored in the liver as hemosiderin or ferritin Converted to stercobilin and urobilin and excreted in feces Amino acids Back into the plasma for reuse/recycling Red Blood Cells An important measurement involving RBCs is the hematocrit. The hematocrit is the % of whole blood occupied by RBCs. It’s reflective of the body’s O2 carrying capacity. What’s the hematocrit in the sample below? Homeostatic Imbalance Anemias • Anything that lowers oxygen carrying capacity Too Few RBC • Hemorrhagic, Hemolytic, Aplastic Low Hemoglobin • Iron-deficiency, athlete’s anemia Homeostatic Imbalance Genetic Thalassemias • Missing a globin chain • RBC fragile and ruputre easy Homeostatic Imbalance Sickle-cell anemia -Results from a defective gene coding for an abnormal hemoglobin called hemoglobin S (HbS) - HbS has a single amino acid substitution (287) - This defect causes RBCs to become sickle-shaped in low-oxygen situations Leukocytes (WBCs) • Only blood components that are complete cells: – 4000 – 11,000 WBC’s /mm3 – Make up 1% of the total blood volume – Can leave capillaries via diapedesis – Move through tissue spaces – Most are found in lymphatic organs and loose connective tissues. Here we see a WBC squeezing its way out of a blood vessel – in other words, performing diapedesis. Damaged Cell WBC WBC Releases chemicals that attract WBCs (known as chemotactants). WBC WBC WBCs converge on the area – i.e., they exhibit positive chemotaxis. They then release more chemotactants to attract more WBCs. Classification of Leukocytes: 1. Granulocytes- Contain granules that are dyed by Wright’s stain -neutrophils, eosinophils, and basophils -all phagocytotic cells 2. Agranulocytes -lack any visible granules that take up Wright’s Stain -lymphocytes and moncytes Neutrophils • Most numerous. 60% of circulating WBCs. • A.k.a. polymorphonuclear leukocytes b/c of their multilobed nucleus. • Function primarily in killing bacteria. • Contain pale, lilac colored granules Eosinophils • • • • 3% of circulating WBCs. Function primarily in killing parasitic worms. Also help reduce the severity of allergy attacks. Contain reddish/orangish granules Basophils • Least numerous. <1% of circulating WBCs. • Involved in inflammation. • Contain purplish granules that contain: – Histamine – a vasodilator – Heparin – an anticoagulant Lymphocytes • 25% of circulating WBCs. • No granules. Large purple nucleus dominates most of the cell. • 2 main types: – T lymphocytes • Control/coordinate immune response • Kill virus-infected and cancerous cells – B lymphocytes • Secrete antibodies (immunoglobulins) Monocytes • • • • 6% of circulating WBCs. No granules. Large pale cells w/ U or kidney-shaped nucleus. Travel in the blood. Become macrophages w/in the tissue spaces. In this picture, find: RBCs, 2 neutrophils, an eosinophil, a basophil, a monocyte, a lymphocyte, and a platelet. What can you find here? Homeostatic Imbalance Leukemias • Cancerous bone marrow cell that send immature white blood cells into blood stream • Immune response lessen Platelets • Cell fragments of megakaryocytes (giant cells created from mitosis w/o cytokinesis) • Contain chemicals vital to coagulation. • A.k.a. thrombocytes. Hemostasis • Designed for healing the vasculature and providing a framework for tissue repair Three phases 1. Vascular spasms – immediate vasoconstriction in response to injury 2. Platelet plug formation 3. Coagulation (blood clotting) Clotting Factors Multiple substances are involved in the clotting process. – Most of these clotting factors are formed in the liver. • • Vitamin K is required for the synthesis of many of them. Calcium is also required for coagulation. Two ways to make prothrombin activator 1. Extrinsic Pathway – quick 2. Intrinsic Pathway – amplification, large quanities Clot Retraction • Healing of the blood vessel is taking place as clot retraction occurs • Platelets retract like muscle fibers • Eventually the blood clot dissolves in fibrinolysis – Plasmin digests fibrin Mosquito saliva contains an enzyme called apyrase. Which of the following is it most likely to do? a. b. c. d. Inhibit fibrinolysis Promote thrombin production Inhibit platelet aggregation Promote fibrin production • • • • Antiprostaglandin Aspirin Low dose helps reduce risk of heart attack Reduces platelet aggregation and plug formation Reduces risks to embolism Heart attack and stroke Blood Groups • Humans have 30 varieties of naturally occurring RBC antigens • The antigens of the ABO and Rh blood groups cause vigorous transfusion reactions with agglutination (cell clumping) and severe consequences when they are improperly transfused • RBC membranes have glycoprotein antigens on their external surface • These antigens are: – Unique to the individual – Recognized as foreign if transfused into another individual • Presence/absence of these antigens are used to classify blood groups AB0 blood grouping system • Blood group A – A antigens on the surface of their red blood cells and B antibodies in their blood plasma. • Blood group B – B antigens on the surface of their RBCs and A antibodies • Blood group AB – A and B antigens on the surface of their RBCs and no A or B antibodies at all • Blood group 0 (null) – No antigens on the surface of their RBCs but both A and B antibodies = red blood cell ABO Blood Groups Universal donor Universal receiver - Table 16.4 Blood Typing http://nobelprize.org/medicine/educational/landsteiner/readmore.html • When serum containing anti-A or anti-B antibodies is added to blood, agglutination (cell clumping) will occur between the antibody and the corresponding antigens • Positive reactions indicate agglutination (cell clumping) Blood typ e being tested RBC agglutinog ens AB B A O A and B B A none Serum Reaction Anti-A Anti -B + + – + + – – – Rh factor blood grouping system Rh+ • Have Rh factor on RBCs • Do not make Rh antibodies Rh• Do not have Rh factor on RBCs • Do not make Rh antibodies unless exposed to Rh factor!!! What will occur??? http://nobelprize.org/medicine/educational/landsteiner/readmore.html Women and Pregnacy • Rh- women with Rh+ babies • Pregnancy okay, but mother builds Rh antibodies • If next pregnancy is Rh+ again mothers antibodies will kill fetus RBCs • RhoGAM blocks the Rh+ affect and does not allow mother to make antibodies Chapter 17 The Heart Base of Heart Apex of Heart Figure 17.1 Heart Coverings • Pericardium- membranes that cover the heart • Fibrous Pericardium- outermost layer, Elastic fibrous tissue » Anchors the heart in place staying attached to diaphragm and lungs • Parietal Pericardium- directly attached to fibrous pericardium • Visceral Pericardium- attaches directly to heart Pericardial fluid fills the space between the parietal and visceral Layers FUNCTION: lubrication, reduces friction Homeostatic Imbalance • Pericarditis Inflammation of the pericardium Heart Wall Layers • Epicardium – outermost layer • (same as visceral pericardium) • Myocardium – inner layer • cardiac muscle layer forming the bulk of the heart • Endocardium – endothelial layer that lines the chambers of the heart Chambers and Associated Great Vessels BODY Superior Portion of the body Coronary veins Superior and Inferior Vena Cavae Right Atrium Inferior Portion of the body Tricuspid Valve Pulmonary Semilunar Valve Right Ventricle LUNGS Aorta Left Atrium Mitral (bicuspid) valve Aortic Semilunar Valve Left Ventricle Interventricular Septum Coronary Circulation- the heart’s own blood supply • Heart works continuously thus requires a constant supply of oxygen and nutrients Aorta Right atrium Coronary Sinus Coronary Arteries Right Coronary Artery Left Coronary Artery Supplies: Right atrium, Supplies: Left atrium, portions of both Portions of both ventricles Ventricles and the Interventricular septum And portions of the hearts Electrical conduction system Coronary Veins Branches of the right and left arteries merge at junctions Called Anastomoses This creates Collateral circulation- Homeostatic Imbalance Arthrosclerosis • Plaque build up in coronary artery • Videos Homeostatic Imbalance Heart Attack • Often the result of blockage of a coronary artery • Thus a portion of the heart is not being supplied with oxygen • Angina pectoralis- pain in the chest • Myocardial Infarction- prolonged blockage with death of cardiac muscle tissue External Heart: Anterior View Figure 17.4b External Heart: Posterior View Figure 17.4d Gross Anatomy of Heart: Frontal Section Figure 17.4e Heart Valves • Heart valves insure unidirectional blood flow through the heart • Atrioventricular (AV) valves lie between the atria and the ventricles • AV valves prevent backflow into the atria when ventricles contract • Chordae tendineae anchor AV valves to papillary muscles Heart Valves – AV Valves Figure 17.9 Heart Valves – Semilunar Valves Figure 17.10 Semilunar Valves prevent backflow of blood into the ventricles Microscopic Heart Muscle Anatomy • • • • Intercalated discs anchor cardiac cells together and allow free passage of ions Heart muscle behaves as a functional syncytium (as a unit) Does not need input from nervous system to contract (automaticity) The heart is made up of two types of muscle fibers: 1. 2. Contractile cells – for contraction of muscle Cells of the conducting system (autorhythmic cells) –control electrical activity Contractile Cells Cardiac contractile muscle is similar to skeletal muscle contraction needs (1) Action potential (2) Release of Calcium into cells (3) Binding of calcium to troponins Difference: Skeletal fibers have a Short refractory period while cardiac has a long refractory period. WHY??? Figure 17.11b Cells of the Conductive System Autorhythmic cells – Initiate action potentials – Have unstable resting potentials called pacemaker potentials – Use calcium influx (rather than sodium) for rising phase of the action potential – Rate of depolarization varies but Fastest rate of depolarization is in sinoatrial (SA) node known as pacemaker Electrical Events 1. 2. 3. 4. 5. Sinoatrial (SA) node generates impulses about 75 times/minute thus is the pacemaker Electical impulse from SA node spreads across both atria causing contraction Atrioventricular (AV) node delays the impulse approximately 0.1 second. AV bundle splits into two pathways in the interventricular septum (bundle branches) Impulse passes from atria to ventricles via the atrioventricular bundle (bundle of His) – – Bundle branches carry the impulse toward the apex of the heart Purkinje fibers carry the impulse to the heart apex and ventricular walls Sequence of Electrical Events VIDEO Figure 17.14a Regulation of Heart Rate • Remember the heart does not need nervous system stimulation to contract but the autonomic nervous system can modify heart rate – Parasympathetic- Conserve – Sympathetic- Mobilize – Vagus Nerve- Electrocardiography • What are electrical events of heart? 1. Atrial depolarization 2. Atrial repolarization 3. Ventricular depolarization 4. Ventricular repolarization • P wave corresponds to depolarization of SA node • QRS complex corresponds to ventricular depolarization • T wave corresponds to ventricular repolarization • Atrial repolarization record is masked by the larger QRS complex Heart Sounds • Heart sounds (lub-dup) are associated with closing of heart valves Figure 17.19 Cardiac Cycle • Cardiac cycle refers to all events associated with blood flow through the heart – Systole – contraction of heart muscle – Diastole – relaxation of heart muscle Phases of the Cardiac Cycle • Ventricular filling – mid-to-late diastole – Heart blood pressure is low as blood enters atria and flows into ventricles – AV valves are open, then atrial systole occurs Phases of the Cardiac Cycle • Ventricular systole – Atria relax – Rising ventricular pressure results in closing of AV valves Isovolumetric contraction phase – Ventricular ejection phase opens semilunar valves Phases of the Cardiac Cycle • Isovolumetric relaxation – early diastole – Ventricles relax – Backflow of blood in aorta and pulmonary trunk closes semilunar valves • Dicrotic notch – brief rise in aortic pressure caused by backflow of blood rebounding off semilunar valves Phases of the Cardiac Cycle Figure 17.18a Phases of the Cardiac Cycle Figure 17.18b Homeostatic Imbalance • • • • • Improper valve function Changes the sound Heart Murmurs Mitral Valve Prolapse two flaps loose LISTEN TO SOUNDS Cardiac Output (CO) and Reserve • CO is the amount of blood pumped by each ventricle in one minute • CO = HR x SV • HR is the number of heart beats per minute • SV is the amount of blood pumped out by a ventricle with each beat • Cardiac reserve is the difference between resting and maximal CO Cardiac Output: Example • CO (ml/min) = HR (75 beats/min) x SV (70 ml/beat) • CO = 5250 ml/min (5.25 L/min) Regulation of Stroke Volume • SV = end diastolic volume (EDV) minus end systolic volume (ESV) • EDV = amount of blood collected in a ventricle during diastole • ESV = amount of blood remaining in a ventricle after contraction Factors Affecting Stroke Volume 1. Preload – amount ventricles are stretched by contained blood, the greater the SV will be, described as the Frank Starling Law 2. Contractility – cardiac cell contractile force due to factors other than EDV such as SNS and PNS 3. Afterload – back pressure exerted by blood in the large arteries leaving the heart, thus the tension the ventricle must produce to push blood out the semilunar valve An increase in afterload, decreases SV Frank-Starling Law of the Heart • Preload, or degree of stretch, of cardiac muscle cells before they contract is the critical factor controlling stroke volume • Slow heartbeat and exercise increase venous return to the heart, increasing stroke volume • Blood loss and extremely rapid heartbeat decrease stroke volume Preload and Afterload Figure 17.20 CHAPTER 18 • Blood vessels Blood Vessels I. Overview of Blood Vessel Structure and Function II. Pressure Dynamics including blood flow, blood pressure and resistance Cross section of an artery, vein and nerve Generalized Structure of Blood Vessels Figure 18.1b Arterial Vessels: Greatest to smallest • • • • Elastic or Conducting Vessels Muscular Arteries Arterioles Capillaries Elastic (Conducting) Arteries • Thick-walled, large lumen arteries near the heart; the aorta and its major branches – Contain elastin in all three tunics – Withstand and smooth out large blood pressure fluctuations seen with systole and diastole – Blood = flow fairly continuous Muscular Arteries and Arterioles • Distal to elastic arteries; deliver blood to organs and muscles – Have thick tunica media with more smooth muscle and less elastic tissue – Active in vasoconstriction • Arterioles – smallest arteries; lead to capillary beds – Control flow into capillary beds via vasodilation and constriction Capillaries – smallest blood vessels • Allow only a single RBC to pass at a time; usually one cell layer thick on a basement membrane Capillary RBC RBC RBC RBC thin tunica interna (Only 1 cell thick) Easy Gas Exchange! RBC RBC Major types of Capillary Beds • Continuous • Fenestrated • Sinusoidal Continuous Capillary Structure •Most Common •Abundant in the skin and muscles •Tight junctions •Intercellular clefts of unjoined membranes that allow the passage of water and small molecules Blood-brain barrier Continuous capillaries of the brain: Tight junctions completely around the endothelium Figure 18.3a Fenestrated Capillary Structure •Active capillary absorption or filtrate formation occurs •(e.g., small intestines, endocrine glands, and kidneys) •Pores (fenestrations) – usually covered by thin membrane •Greater permeability to solutes and fluids than other capillaries Figure 18.3b Sinusoids •Leaky with large lumens •Found in the liver, bone marrow, lymphoid tissue, and in some endocrine organs •Allow large proteins and blood cells to move through •Blood flows sluggishly, allowing for modification in various ways Protein Blood Cell Capillary Beds • Have both an arterial and venous side • Metarteriole joins arterial and venous sides through the bed • Precapillary sphincters made of smooth muscle are present; separate the metarteriole from the true capillaries • Sphincters contracted-no flow through the bed • Sphincters relaxed-blood flows through the bed Capillary Beds Figure 18.4a Capillary Beds Precapillary sphincter – cuff of smooth muscle •Blood flow is regulated by vasomotor nerves and local chemical conditions, so it can either bypass or flood the capillary bed Figure 18.4b Velocity of Blood flow Figure 18.13 Venous Vessels: Smallest to greatest Venules •Smallest veins •Lack a tunica media Veins •Composed of three tunics, with a thin tunica media and a thick tunica externa consisting of collagen fibers and elastic networks •Capacitance vessels (blood reservoirs) that contain 65% of the blood supply •Large-diameter lumens, which offer little resistance to flow •Valves (resembling semilunar heart valves), which prevent backflow of blood •Vena cavae •largest veins; where they enter the heart Homeostatic Imbalance Varicose Veins • Vein valves become loose • Obesity, hereditary, pregnancy put downward pressure on veins • Blood pools up stretches • Anal veins, hemorroids Terminology Blood Flow Actual volume of blood flowing through a vessel, an organ, or the entire circulation in a given period – Varies widely through individual organs, according to immediate needs Blood Pressure (BP) • Force per unit area exerted on the wall of a blood vessel by its contained blood – Measured in mm Hg – Measured in reference to systemic arterial BP in large arteries near the heart • *The differences in BP = provide the driving force that keeps blood moving from higher to lower pressure areas* Relationship of diastolic and systolic BPs • Systolic pressure – peak pressure exerted on an artery during ventricular contraction; top number in fraction eg. 120/80 • Diastolic pressure – lowest level of arterial pressure when the heart is relaxed; bottom number infraction eg. 120/80 Arterial Blood Pressure • Pulse pressure – the difference between systolic and diastolic pressure • Mean arterial pressure (MAP) – pressure that propels the blood to the tissues Diastole lasts longer than systole=Mean Pressurenot just halfway between systolic and diastolic • MAP = diastolic pressure + 1/3 pulse pressure Venous Blood Pressure • Only about 20 mm Hg throughout the venous system • Two ways to get blood through the venous system 1. Pressure changes in ventral body cavity push blood toward the heart 2. Skeletal Muscle Pump: the relaxation/contraction of skeletal muscle squeezes blood up past one way valves back toward the heart Maintaining Blood Pressure • Maintaining blood pressure requires: – Cooperation of the heart, blood vessels, and kidneys – Supervision of the brain Blood Pressure Controls include short and long term control mechanisms Controls of Blood Pressure • Short-term controls: – Are mediated by the nervous system and bloodborne chemicals – Counteract moment-to-moment fluctuations in blood pressure by altering peripheral resistance • Long-term controls: regulate blood volume kidney is the big player here Short-Term Mechanisms: Neural Controls • Neural controls of peripheral resistance: – Vasomotor center/Cardiac center in medulla of brain stem – Alter blood distribution to respond to specific demands – Maintain MAP by altering blood vessel diameter Short-Term Mechanisms: Vasomotor Activity • Sympathetic activity causes: – Vasoconstriction and a rise in blood pressure if increased; “Fight or flight” – Blood pressure to decline to routine levels if decreased • Vasomotor activity is modified by: – Baroreceptors (pressure-sensitive) found in aorta/carotids – Chemoreceptors (O2, CO2, and H+ sensitive) locations as above – Higher brain centers – Bloodborne chemicals and hormones Chemicals that Increase Blood Pressure • Adrenal medulla hormones – norepinephrine and epinephrine increase blood pressure • Antidiuretic hormone (ADH) – causes intense vasoconstriction in cases of extremely low BP • Angiotensin II – causes intense vasoconstriction when renal profusion is inadequate • Endothelium-derived factors – endothelin and prostaglandin-derived growth factor (PDGF) are both vasoconstrictors WHY?(Hint:rememberChapter 16 Blood) Chemicals that Decrease Blood Pressure • Atrial natriuretic peptide (ANP) – causes blood volume and pressure to decline • Nitric oxide (NO) – has brief but potent vasodilator effects • Inflammatory chemicals – histamine, etc. are potent vasodilators • Alcohol – causes BP to drop by inhibiting ADH Long-Term Mechanisms: Renal Regulation • Baroreceptors adapt to chronic high or low blood pressure • Kidneys maintain long-term BP by regulating blood volume – Increased BP stimulates the kidneys to eliminate water, thus reducing BP – Decreased BP stimulates the kidneys to increase blood volume and BP Renin-angiotensin mechanism in the kidneys (Indirect renal mechanism) BP Renin Angiotensin II Aldosterone ADH vasoconstriction Enhances renal reabsorption More water reabsorption In the kidneys • Autoregulation: Local Regulation of Blood Flow Autoregulation – routine, automatic adjustment of blood flow to each tissue in proportion to its requirements at any given point in time How does this occur? 1. Myogenic Controls- Increased stretch causes a reflex vasoconstriction 2. Metabolic Controls-Increased acidity,CO2, or lactic acid will cause vasodilation Long-Term Autoregulation • Is evoked when short-term autoregulation cannot meet tissue nutrient requirements • May evolve over weeks or months to enrich local blood flow • Angiogenesis takes place: – – – – When the number of vessels to a region increases When existing vessels enlarge When a heart vessel becomes partly occluded Routinely to people in high altitudes, where oxygen content of the air is low Capillary Blood Pressure What could happen with high Capillary pressure? • Low BP is sufficient to force filtrate out into interstitial space and distribute nutrients, gases, and hormones between blood and tissues Capillary Dynamics: Movement of Fluid • Arterial side of the capillary bed has higher blood pressure than the venous side. This pressure is higher than the oncotic pressure inside the capillary. Fluid gets forced through vessel walls. • Venous side of the capillary bed has lower blood pressure than the arterial side. The oncotic pressure is higher than the BP so fluid is pulled back into the vessel. The fluid that doesn’t make it back in gets picked up by the lymphatic system and returned to the heart Capillary Dynamics: Gas & Nutrient Exchange • O2, CO2, wastes and nutrients pass through capillary walls by diffusion which is a passive process in which molecules move from areas of high to low concentration • O2/Nutrients are in a higher concentration inside the vessel so diffuse to tissue • CO2/Wastes are in higher concentration in tissue so diffuse into the vessel Capillary Exchange of Respiratory Gases and Nutrients Figure 18.14.2 Circulatory Shock • Blood vessels are inadequately filled - blood cannot circulate normally • Results in inadequate blood flow to meet tissue needs – Hypovolemic shock – results from large-scale blood loss – Vascular shock – poor circulation resulting from extreme vasodilation – Cardiogenic shock – the heart cannot sustain adequate circulation Homeostatic Imbalance (Alterations in Blood Pressure) • Hypotension – low BP in which systolic pressure is below 100 mm Hg • Hypertension – condition of sustained elevated arterial pressure of 140/90 or higher – Transient elevations - normal – Fever, physical exertion, and emotional upset – Chronic elevation - heart failure, vascular disease, renal failure, and stroke – In general, a normal blood pressure reading for healthy adults is below 120 systolic and 80 diastolic, or 120/80. Hypotension • Orthostatic hypotension – temporary low BP and dizziness when suddenly rising from a sitting or reclining position • Chronic hypotension – hint of poor nutrition and warning sign for Addison’s disease (inadequate adrenal cortex function) • Acute hypotension – important sign of circulatory shock – Threat to patients undergoing surgery and those in intensive care units Hypertension • Hypertension – sustained BP of 140/90 or higher: – Is the major cause of heart failure, vascular disease, renal failure, and stroke – Weakens the heart and ravages the blood vessels – Causes tears in vessel endothelium that accelerate atherosclerosis • Elevated diastolic pressure is more significant than systolic – It indicates progressive occlusion and/or hardening of the arterial tree Hypertension • Primary or essential hypertension – risk factors in primary hypertension include diet, obesity, age, race, heredity, stress, and smoking; no identifiable cause is found • Secondary hypertension – due to identifiable disorders, including excessive renin secretion, arteriosclerosis, and endocrine disorders