Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Abnormal psychology wikipedia , lookup
Moral treatment wikipedia , lookup
Attachment theory wikipedia , lookup
Attachment in adults wikipedia , lookup
Attachment measures wikipedia , lookup
Reactive attachment disorder wikipedia , lookup
Mental status examination wikipedia , lookup
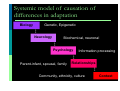
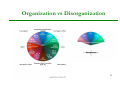
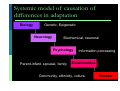
The Development of Protective Strategies across the Lifespan The DMM as a bio-psycho-social model of adaptation Postulates? Danger & dysfunction Evolution of brain for danger (Mather & Sutherland) Parallel processing to produce multiple dispositional representations (Damascio, Eagleton) Relation of exposure to danger to psychiatric disorder (Kindler et al.) Centrality of maladaptive family functioning (McLaughlin et al.) Security? No, variability. 2 What is the Dynamic-Maturational Model (DMM) of Attachment & Adaptation? A comprehensive theory about The effects of exposure to danger on Psychological and behavioural functioning 3 Theories in the DMM Bowlby Evolutionary biology Ethology General systems theory Psychoanalytic theory Information processing After Bowlby & Ainsworth Piaget Behavioral learning theory Cognitive neuroscience Vygotsky Social ecology Chaos (complexity) theory Ainsworth Gestalt theory Empirical evidence Genetics & epigenetics ABC Strategies Person-centered therapy Strange Situation Family systems theory Developmental pathways Epidemiology, etc. The DMM is a bio-psycho-social model of adaptation. 4 Systemic model of causation of differences in adaptation Biology Genetic, Epigenetic ↕ Neurology Biochemical, neuronal ↕ Psychology Information processing ↕ Parent-infant, spousal, family Relationships ↕ Community, ethnicity, culture Context The DMM is two models of adaptation Developmental model of individual differences in adaptation & maladaptation Treatment model for expanding adaptation 6 Clinically the DMM can Reframe disorder as dysfunction around protection Not symptom based (DSM, ICD) Not based on disorganization (ABCD) Reconceptualise causation in a systemic and accurately complex manner Lead to personalised mental health treatment 7 Problems with Disorganization Is theoretically incoherent (Duschinsky, Rutter et al.; Slade; Thompson & Raikes) Is neurologically inaccurate regarding fear (Le Doux; Leppänen & Nelson; McLaughlin et al) Accounts for too little variance (2%, Friedman & Boyle; 5% vs 19%, Spieker & Crittenden) Fails to identify the function of behavior (Crittenden & Ainsworth) Treats behavior as meaning rather than meaning being generated dyadically (Hoffmeyer) Assumes past is more powerful than present Not explain what the mind is doing (Crittenden) Lacks clinical utility; dysfunction in 1 category Overlooks development (Crittenden & Ainsworth) (Wilkinson) 8 Organization vs Disorganization 9 A developmental model of psychological dysfunction Individual differences in attachment across the lifespan DMM Attachment is a theory about protection from danger Danger is normal & universal (McLaughlin et al) Danger experienced by one’s parents Danger to oneself Past Current Danger to one’s children The DMM proposes that behaviour is organized in response to threat. 11 Psychological & behavioral organization Protect the self Select and protect a reproductive partner Protect one’s progeny to their reproductive maturity Safety & sex: That’s all there is! 12 Three aspects of attachment Relationship with a protective person Strategy for eliciting protection and comfort from the attachment figure Information processing that underlies attachment behaviour 13 Life cycle development of attachment relationships 14 Attachment as a protective strategy 1. Type B: Communicate thoughts & feelings openly & clearly; negotiate & compromise; 2. Type A: Don’t do the wrong thing; do the right thing; hide your negative feelings; 3. Type C: Stick to your feelings; don’t negotiate or compromise, don’t delay gratification; deceive if you must. 15 DMM Self-Protective Strategies in Infancy B3 B1-2 Comfortable Reserved A1-2 C1-2 Avoidant A+ precompulsive B4-5 Reactive Resistant/ Passive A/C precoercive C+ 16 DMM Strategies in the Preschool Years B3 B1-2 Comfortable Reserved A1-2 C1-2 Threatening/ Disarming Socially Facile/ Inhibited A3-4 Compulsively Caregiving/ Compliant B4-5 Reactive A/C C3-4 Aggressive/ Feigned Helpless 17 DMM Self-Protective Strategies in the School Years B3 B1-2 Comfortable Reserved C1-2 A1-2 Threatening/ Disarming Socially Facile/ Inhibited A3-4 Compulsively Caregiving/ Compliant B4-5 Reactive A/C C3-4 Aggressive/ Feigned Helpless C5-6 Punitive/ Seductive 18 DMM Self-Protective Strategies in Adolescence B3 B1-2 Comfortable Reserved A1-2 C1-2 Threatening/ Disarming Socially Facile/ Inhibited A3-4 Compulsively Caregiving/ Compliant A5-6 Compulsively Promiscuous/ Self-Reliant B4-5 Reactive A/C C3-4 Aggressive/ Feigned Helpless C5-6 Punitive/ Seductive 19 DMM Self-Protective Strategies in Adulthood B3 B1-2 Comfortable Reserved B4-5 Reactive A1-2 C1-2 Threatening/ Disarming Socially Facile/ Inhibited A3-4 C3-4 A/C Compulsively Caregiving/ Compliant Aggressive/ Feigned Helpless A5-6 Compulsively Promiscuous/ Self-Reliant C5-6 Punitive/ Seductive A7-8 Delusional Idealization/ Externally Assembled Self Psychopathy AC C7-8 Menacing/ Paranoid 20 21 Empirical findings: Secure, Type B attachment: Safe and comforting contexts Optimal child functioning. Anxious, Types A & C attachment: Exposure to danger and lack of comfort Developmental risk. 22 Why do we assume that anxious attachment is bad? Danger is the problem. 23 Anxious attachment is the solution! It is the child’s strategy for eliciting protection and comfort from the parent. 24 An information processing model of psychological dysfunction Individual differences in the use of affect and cognition Information Processing Sensory stimulation ⇓ Patterns of neurological activation ⇓ Representation ⇓ Disposition to behave 26 Sensory Stimulation ⇓ ⇓ ⇓ Intensity of arousal Temporal contingency Intensity of stimulation ⇓ ⇓ ⇓ Soma Cognition Affect 27 Three Types of Prediction Soma Bodily state Cognition Affect Learning of prior temporal contingencies Unfocused, context-elicited arousal: anxiety Integration Mental integration of cognitive & affective information to yield more accurately predictive information 28 Transformations of information Truly predictive Erroneous prediction Omitted from prediction Distorted for prediction Falsified for prediction Denied prediction Delusional prediction 29 Parallel Arousal Systems Arousal • • • • • Pain Fear Anger Desire for comfort Alert & comfortable • • • • Bored Tired Sleep Depression Sexual Arousal • • • • • • • • • Sexual pain Sexualized terror Sexual aggression/submission Romanticism Affection Satisfaction Afterglow Sleep Numbness Arousal enables us to adapt to the demands of the context 1 2 3 4 1 3. Optimum state of arousal 2. High Level of Arousal 4.Low Level of Arousal 31 Multiple Dispositional Representations 32 Tulving & Schacter DMM Self-Protective Strategies in Infancy Integrated True Cognition True Negative Affect B3 B1-2 Comfortable Reserved A1-2 C1-2 Avoidant A+ precompulsive B4-5 Reactive Resistant/ Passive A/C precoercive C+ 33 DMM Strategies in the Preschool Years Integrated True Cognition True Negative Affect B3 B1-2 Comfortable Reserved Omitted Negative Affect & Distorted Cognition False Positive Affect A1-2 C1-2 Threatening/ Disarming Socially Facile/ Inhibited A3-4 Compulsively Caregiving/ Compliant B4-5 Reactive A/C C3-4 Aggressive/ Feigned Helpless Omitted True Cognition & Distorted Affect Distorted Negative Affect 34 DMM Self-Protective Strategies in the School Years Integrated True Information True Negative Affect True Cognition B3 B1-2 Comfortable Reserved Omitted Negative Affect & Distorted Cognition False Positive Affect C1-2 A1-2 Threatening/ Disarming Socially Facile/ Inhibited A3-4 Compulsively Caregiving/ Compliant B4-5 Reactive A/C Omitted True Cognition & Distorted Affect C3-4 Aggressive/ Feigned Helpless C5-6 False Cognition Punitive/ Seductive 35 DMM Self-Protective Strategies in Adolescence Integrated True Information True Negative Affect True Cognition B3 B1-2 Comfortable Reserved Omitted Negative Affect & Distorted Cognition False Positive Affect A1-2 Compulsively Caregiving/ Compliant A5-6 Compulsively Promiscuous/ Self-Reliant Denied Negative Affect C1-2 Omitted True Cognition & Distorted Affect Threatening/ Disarming Socially Facile/ Inhibited A3-4 B4-5 Reactive A/C C3-4 Aggressive/ Feigned Helpless C5-6 False Cognition Punitive/ Seductive Denied True Cognition 36 DMM Self-Protective Strategies in Adulthood Integrated True Information True Cognition B1-2 Comfortable Reserved Omitted Negative Affect & Distorted Cognition False Positive Affect True Negative Affect B3 B4-5 Reactive A1-2 C1-2 A3-4 C3-4 A/C Compulsively Caregiving/ Compliant Aggressive/ Feigned Helpless A5-6 Compulsively Promiscuous/ Self-Reliant Denied Negative Affect Omitted True Cognition & Distorted Affect Threatening/ Disarming Socially Facile/ Inhibited C5-6 False Cognition Punitive/ Seductive A7-8 Delusional Idealization/ Externally Assembled Self Psychopathy AC C7-8 Denied True Cognition Menacing/ Paranoid Delusions of Repair Integrated Transformed Information Delusions of Revenge 37 Symptoms & functions Strategies lower in the circle have more symptomatic behaviour The symptoms can function protectively (e.g., deception in the context of danger) or not. Some functions are overlooked clinically Attention deficit (prevent perception of intolerable threat) Delusions (feel safe in the context of danger) Psychoses (escape untenable conflict by enlisting help) The function of symptoms can change with development 38 Which strategy is best? Each is the best for some problem. None is best for every problem. To be safe, we need them all! 39 A Dynamic-Maturational Model of personalized mental health treatment Matching treatment to individual differences in information processing Why do we need a new theory of treatment? Don’t we have enough? Not Not Not Not developmental sufficiently empirical sufficiently systemic sufficiently effective We need a way to choose among ~1000 treatments. Which is the best? 41 Treatment Efficacy Findings 40% drop out 65% short-term benefit 50% no treatment benefit!! Is 15% effectiveness enough? 10-20% harmful 42 Treatment process Assess: Danger, strategy, information processing Somatic, cognitive, affective strategies Types of transformation (true, false, omitted, distorted …) Degree of conscious awareness (implicit to integrative) Formulate the central issue regarding protection Choose techniques to fit IP & formulation Select & implement a treatment strategy Assess the effect, reformulate, etc. 43 DMM assessments: Interlocking lifespan series CARE-Index: Infancy CARE-Index: Toddlerhood Strange Situation: Infancy PAA: 2-5 years SAA: 6-13 years TAAI: 16-25 years AAI: Adulthood Parents’ Interview: Whole family 44 Systemic formulation Within a family, within cultural context Functional explanations around protection & reproduction Relational understanding of dysfunction Replace individual disorder with interpersonal adaptation to threat. 45 Novel hypotheses & treatment implications Maltreatment (Crittenden, Grey, Seefeldt) Domestic violence (Worley, Walsh & Lweis) Post-natal depression (Crittenden) Psychosis ( Crittenden & Landini) Eating disorders (Dallos; Ringer & Crittenden; Zachrisson) Autism (Crittenden, Dallos, Landini, Kozlowska) ADHD (Crittenden , Dallos, Landini, Kozlowska) PTSD (Crittenden & Heller; Kuo, Kaloupek,& Woodward) Somatic, conversion, & pain disorders (Crittenden, Kozlowska et al.) Pervasive developmental disorder (Crittenden) Child sexual abuse & sexual offending (Baim; Crittenden) Personalized mental health treatment By history of exposure to danger By protective strategy By transformation of information By extent of psychological processing Through personal, unique relationship with therapist/transitional attachment figure 47 Attachment can affect treatment as Information about current strategies & information processing Type A versus Type C Extent of processing (implicit to integrative) History of the development of the problem Promote self-respect in client/patient Suggest focus for treatment Functional use of the therapist as a transitional attachment figure to: Highlight the context Practice new behaviour Reflect on outcomes 48 An array of treatments Biology Genetic, Epigenetic Tx ↕ Neurology Biochemical, EMDR, Healing ↕ Psychology Talk therapies ↕ Family Systems, Parent-infant Relationships ↕ Professional development, Advocacy Context Attachment, adaptation, & hope: Why the DMM has utility for clinicians The DMM accepts all treatments as useful strategies for resolving some problem. It treats dysfunction as outdated attempts to stay safe when exposed to danger. It respects the strength needed to develop & diversify strategies for surviving danger. It is empirically testable. It highlights the power of therapists to use themselves to promote healing. 50 Take-away points Danger is universal & elicits protective organization. Adaptation, even ‘anxious’ adaptation, to one’s context is more important than security. Our strength is flexible use of many strategies. Change is most effectively established in a transitional attachment relationship. Personalized mental health treatment ties protection & information processing to type of therapy. 51 pmcrittenden @gmail.com For slides & references [email protected] 54 Strengths approach Flexibility of development & functioning is our species’ major strength. Flexibility permits adaptation to many niches. Plasticity permits individuals to adapt to changing circumstances. Individual differences are an advantage to a population of humans. 55 Reallocation of resources Epidemiological prevention Modify service structures & providers, avoiding overuse of services Use therapists as transitional attachment figures Select therapeutic tools from full array Act in the zone of proximal development for family members Focus on ‘critical cause’ (Crittenden & Ainsworth, 1989) 56 General treatment goals Remove any current danger Begin to establish a balanced transitional attachment relationship Teach observation & verbalization to make personal & interpersonal functioning explicit Interpret functioning from a strengths, self-, partner-, or child-protective perspective Define strategies by context Repair ‘broken’ strategies & expand array of strategies Use reflective integration to enable behavioural regulation 57 A Causal Model of Dysfunction A systemic model of influences on behaviour and adaptation Dysfunction occurs when One’s behaviour does not fit one’s current context; Distortions learned to protect the self in the past create risk in the present for oneself, one’s partner, or one’s children. The ‘causes’ are varied, complex, & interactive. 59 Systemic model of causation of differences in adaptation Biology Genetic, Epigenetic ↕ Neurology Biochemical, neuronal ↕ Psychology Information processing ↕ Parent-infant, spousal, family Relationships ↕ Community, ethnicity, culture Context